ER Exam 1 - Wound etc, Environmental, Endocrine + Hem, Back Pain
1/246
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
247 Terms
these bugs may cause infection in dorsal hand lacerations
staph
strep
corynebacterium
Eikenella
what antibiotic should be given for an infected dorsal hand laceration?
outpatient abx treatment?
Unasyn 3 grams IV
Augmentin 875mg BID
treatment of tendon lacerations
consult hand specialist (distal wrist to MCP)
defer all flexion and thumb tendon injuries (we can do extension injuries)
figure 8 knot
open lac = operative repair
closed lac = splint ± operative repair
suture size for LE
4-0 or larger
you should always document ______________ test when evaluating LE injuries
thompson
when to remove FB in laceration
potential for infection, toxicity, functional problems, persistent pain
removal of wood splinter
tend to break off, so make longitudinal incision over splinter
what is the preferred closure method for a laceration with a foreign body?
clean and irrigate, close only if low risk for infection
tertiary intention
what puncture wounds can receive low pressure irrigation?
uncomplicated clean punctures less than 6 hours old
what is the most common causative agent of infection with puncture wounds?
staph aureus (usually plantar)
abx choice for high risk (bites, plantar) puncture wound
cipro, cephalexin
infected puncture wounds should be evaluated via what to look for FB or boney destruction?
x-ray
what should the management be for high pressure puncture wounds?
- parenteral narcotics for pain
- consult hand surgeon (early surgical debridement)
(digital block contraindicated)
what bugs infect human bite wounds?
Eikenella, staph, strep
what should the initial treatment be for human bites causing lacerations?
copious irrigation + left open and prophylactic abx (Augmentin)
(give Unasyn if infected upon presentation)
what is the treatment for dog bites?
- x-ray (for boney involvement or FB)
- copious irrigation
- primary closure (unless on feet or hands)
- antibiotics (Augmentin or clinda or cipro - infection tends to be polymicrobial)
what is the treatment for cat bites?
- x-ray (for boney involvement or FB)
- copious irrigation
- closure if >2cm
- antibiotics (Augmentin or cefuroxime or doxy)
bacteria common in cat bite
pasteruella multocida
components of procedure note
clinical setting
procedure name
indication
contraindications
consent
anesthesia
description
findings
complications
NO H&P or plan or follow up
soft tissue injury resulting from prolonged exposure to nonfreezing cold and moisture
foot pale, mottled, pulseless and numb
(will not improve quickly with rewarming; will also be painful after rewarming x 2-3 days)
trench foot

painful inflammatory lesions typically affecting ears, hands, and feet from chronic exposure to intermittent damp conditions
localized edema, erythema and cyanosis appearing up to 12 hours after exposure + itching and burning paresthesia
chillblains
what is the treatment for trenchfoot and chillblains?
- elevation, warming and bandaging
- nifedipine (20 mg TID)
- pentoxifylline (400 mg TID)
freezing of tissue that presents with stinging, burning, and numbness
frostbite
how is frostbite classified?
by depth of injury and appearance after rewarming
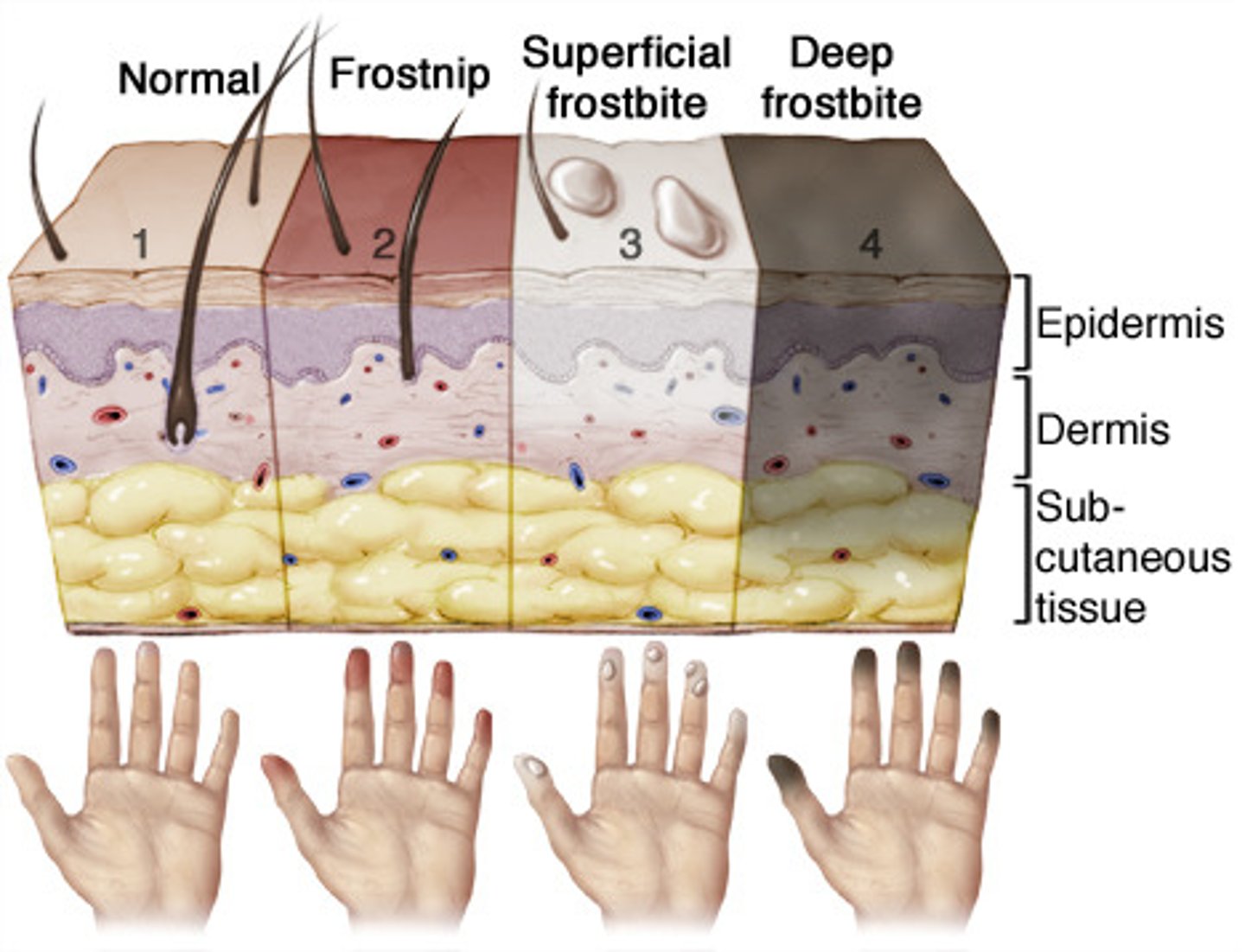
what degree of frostbite is this describing?
partial thickness skin freezing
erythema, edema and LACK of blistering
1st degree (frostnip)
what degree of frostbite is this describing?
freezing of skin and subdermal plexus
hemorrhagic bullae and skin necrosis
3rd degree
what degree of frostbite is this describing?
deeper skin freezing
formation of clear bullae, numbness followed by aching and throbbing
2nd degree
what degree of frostbite is this describing?
extends deeper into muscle, tendon and bone
mottled skin, nonblanching cyanosis with eventual dry black mummified eschar formation
4th degree
what is the treatment for frostbite?
- rapid re-warming in circulating water (20-30 min @ 37-39 C)
- topical aloe vera
- pain management
- local wound care
- splint and elevate extremity
- tetanus
hypothermia is defined as body temperature of less than ______
35 C (95 F)
what are some sxs/s of hypothermia?
shivering, tachycardia, tachypnea, hypertension (mild)
confusion, lethargy, loss of pupillary reflex, bronchorrhea
(all vitals decrease linearly)
what should the workup be for those with hypothermia?
- rectal temperature
- expose pt and remove all clothing
- CBC, BMP, TSH, Lactic acid, clotting
- CXR (looking for infection or aspiration)
- EKG
- routine labs
what are some EKG findings that may be present for hypothermia?
prolongation of PR, QRS, and QT segments
Osborn or J waves
what is the treatment for hypothermia?
- ABCs (ACLS as required)
- gentle rewarming (avoid aggressive rubbing and friction - arrhythmia risk)
- admit if symptomatic or secondary to underlying disease
(pharm therapies ineffective below 30-32 degrees C)
self limited edema in initial exposure to warmth
heat edema
blockage of sweat pores
pruritic erythematous rash
prickly heat (heat rash)
decrease vasomotor tone and peripheral blood pooling in the poorly acclimatized patient
heat syncope
painful cramps in heavily exercised skeletal muscle
treat with fluid replacement with oral electrolyte or IV normal saline
heat cramps
what are the cardinal symptoms/features of heat stroke?
hyperthermia (>40ºC), altered mental status, anhidrosis, seizure
what is the treatment for heat emergencies?
- ABCs
- cool pt down (many methods)
- ICU admissions (most likely)
what is the general local reaction of bites and stings?
pain, erythema, edema, pruritus
what type of insect can cause a sterile pustule that evolves over 6-24 hours and possible cause necrosis and scarring?
fire ant
direct venom effect with GI disturbances and bronchospasm
toxic reaction
would a reaction to a insect bite or sting be worse in severity when the reaction comes on quicker or more delayed?
quicker
what symptoms can a pt experience during a delayed reaction from an insect bite or sting?
fever, malaise, HA, urticaria, lymphadenopathy, polyarthritis
what is the treatment for reactant insect bites and stings?
- remove stinger by scraping
- ice and elevation
- oral antihistamines
- epinephrine .3mg IM
- EpiPen for home and allergist appointment
- admit if severe, >100 stings, extremes of age

Hx: target lesion after a "pinprick feeling"
induration, erythema, blistering
black widow bite
what is the treatment for spider bites?
supportive
what insect bite causes immediate pain and paresthesia with a positive "tap test"? what is the treatment?
scorpion (bark scorpion produces toxicity)
antivenom, resolves 24-48 hours without antivenom

what insect bite causes intense pruritus with burrows concentrated on web spaces, fingers, and toes?
scabies
what is the treatment for scabies?
elimite (permethrin) cream (from neck down)
or
ivermectin PO
what is the treatment for bed bug bites?
local wound care, topical steroids, oral antihistamines
_________ is the most common diving affliction and is caused by the direct mechanical effects of pressure
barotrauma
a medical condition that results from pressure changes that occur when a person descends in water or ascends in altitude
dysbarism
this results from breathing compressed air for excessive depth and time while diving
causes excessive bubble formation in tissue and circulation causing acute occlusive and delayed inflammatory response
decompression sickness (DCS)
what is the treatment for decompression sickness?
high flow oxygen and IV fluids
immediate need for hyperbaric oxygen
death from laryngospasm and hypoxemia without aspiration
dry drowning
survival following asphyxia due to submerging
near drowning
indicators of poor prognosis following near drowning
compromised NV or CV status - CPR required at some point
what assessment should be done for a patient with a "near drowning"?
- ABCs (100% O2, CPAP or intubation)
- assess GCS and O2 sat.
- routine blood work (ABG)
- EKG
- CXR + cervical films
what is disposition largely based on for a near drowning?
GCS score and O2
admit also if associated injury or comorbid condition requiring additional testing or monitoring
(if score >13 and O2 >95% they can be observed for 4-6 hours, then send home)
what type of injury from a burn increases the risk of death, and is very important to evaluate for?
inhalation injury
larger burn, female, older

what type of burn is this describing?
red painful skin without blistering
only epidermis
superficial (1st degree)

what type of burn is this describing?
blistering of skin and exposed dermis is red and moist and very painful
superficial partial thickness (2nd degree)

what type of burn is this describing?
+- blisters; exposed dermis is pale white/yellow
no cap refill and absent pain sensation (parts more superficial are still painful)
deep partial thickness (2nd degree)

what type of burn is this describing?
waxy, leathery and lifeless, +- charring
death of all skin layers, including sweat glands, hair follicles, and nerve endings
full thickness (3rd degree)

what type of burn is this describing?
charring present
epidermis, dermis, subQ, muscle, and sometimes bone involvement
4th degree
what are some clinical indications of an inhalation injury?
facial burns, singed nasal hair, soot in upper airway, hoarseness, wheezing
when estimating burn size adults what percent of the body is the chest?
18
when estimating burn size adults, what percent of the body is each arm (front and back)?
9
when estimating burn size in adults, what percent of the body is the back?
18
when estimating burn size in adults, what percent of the body is the perineum?
1
when estimating burn size in adults, what percent of the body is the whole head?
9
when estimating burn size in adults, what percent of the body is each leg (front and back)?
18
what is the treatment/management of a burn patient?
(ABCs)
airway - faicial burns, wheezing, stridor
breathing - 100% O2
circulation - aggressive IV fluids (Parkland formula)
- apply cool compresses as needed (no more than 10%)
- keep patient warm
- sedation and analgesics
- foley catheter
T/F you should apply ice to burns
FALSE - never
what is the Parkland Burn formula and how is it given?
4 mL x kg x %BSA burned
half in the first 8 hours and other half in 16 hours
(make sure to measure output as well)
an incision made into the necrotic tissue resulting from a severe burn (especially if circumferential)
may be necessary in chest to support breathing
escharotomy
what labs and diagnostics should be ordered for thermal injuries?
ABG w/ carboxyhemoglobin level, CBC, BMP, CXR
what are some treatment options for minor burns?
silvadene (avoid on face can stain) or bacitracin or triple antibiotic ointment
what is the outpatient management for less severe burns?
- cool areas
- cleanse wound
- debride larger or ruptured blisters
- dress with non-adherent dressing
- keep covered from sun
what is the minimal urine output that a burn patient should have?
0.5 mL/kg/hour
when are burn victims sent to a hospital with a specialty burn unit?
3rd degree
<10 or >50
chemical
inhalation
comorbid
trauma like fx
hospital poorly equipped
long term rehab needed
what is the treatment for chemical burns?
decontamination prior to examination
water
what is the treatment for chemical burns from sodium, potassium, calcium, or lithium?
mineral oil (not water in these circumstances)
do alkaline or acidic burns penetrate deeper?
alkaline
AC electricity (standard household electricity) causes _________
DC (ex: lightning) causes ___________
tetany, fibrillation (AC more life threatening)
instant muscle contraction, asystole
what is the treatment for electrical/lightning injuries?
- ABCs
- myoglobin level/CK level
- EKG
treatment high voltage injuries
deep burns may require amputation
acts like crush injury - rhabdomyolysis
fasciotomies
escharotomies
fluid resuscitation
what should the work-up be for lightening injuries?
- EKG
- check for rhabdo
- eye and ear injury
Distinctive feathering marking found on lightning strike victims
Lichtenberg figure
is cardiac monitoring/other testing indicated in a healthy person that has been tasered?
no (likelihood of electrical injury is very low)
Hx of exposure to gas heat, smoke inhalation, acidosis or coma
flu-like symptoms to coma
carbon monoxide poisoning
this is an important lab to measure for carbon monoxide poisoining
COHb (carboxyhemoglobin)
what is the treatment for carbon monoxide poisoning?
highest concentration O2 available
what are the clinical features of hypoglycemia?
sweating, shakiness, anxiety, nausea, dizziness, confusion, slurred speech, blurred vision, HA, lethargy
how can the diagnosis of hypoglycemia be made?
low blood sugar (<50-60) and symptomatic
what is the treatment for hypoglycemia with altered mental status?
50% dextrose 50 mL IV
may need continuous infusion of 5% dectrose to keep glucose >100 (i.e. they took a long acting sulfonylurea)
what is the treatment for hypoglycemia if no IV access?
1 mg glucagon (IM or SQ)
what is the treatment for hypoglycemia that is sulfonylurea induced?
treat as usual
if not responding, give octreotide