ceutics applications of PK
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
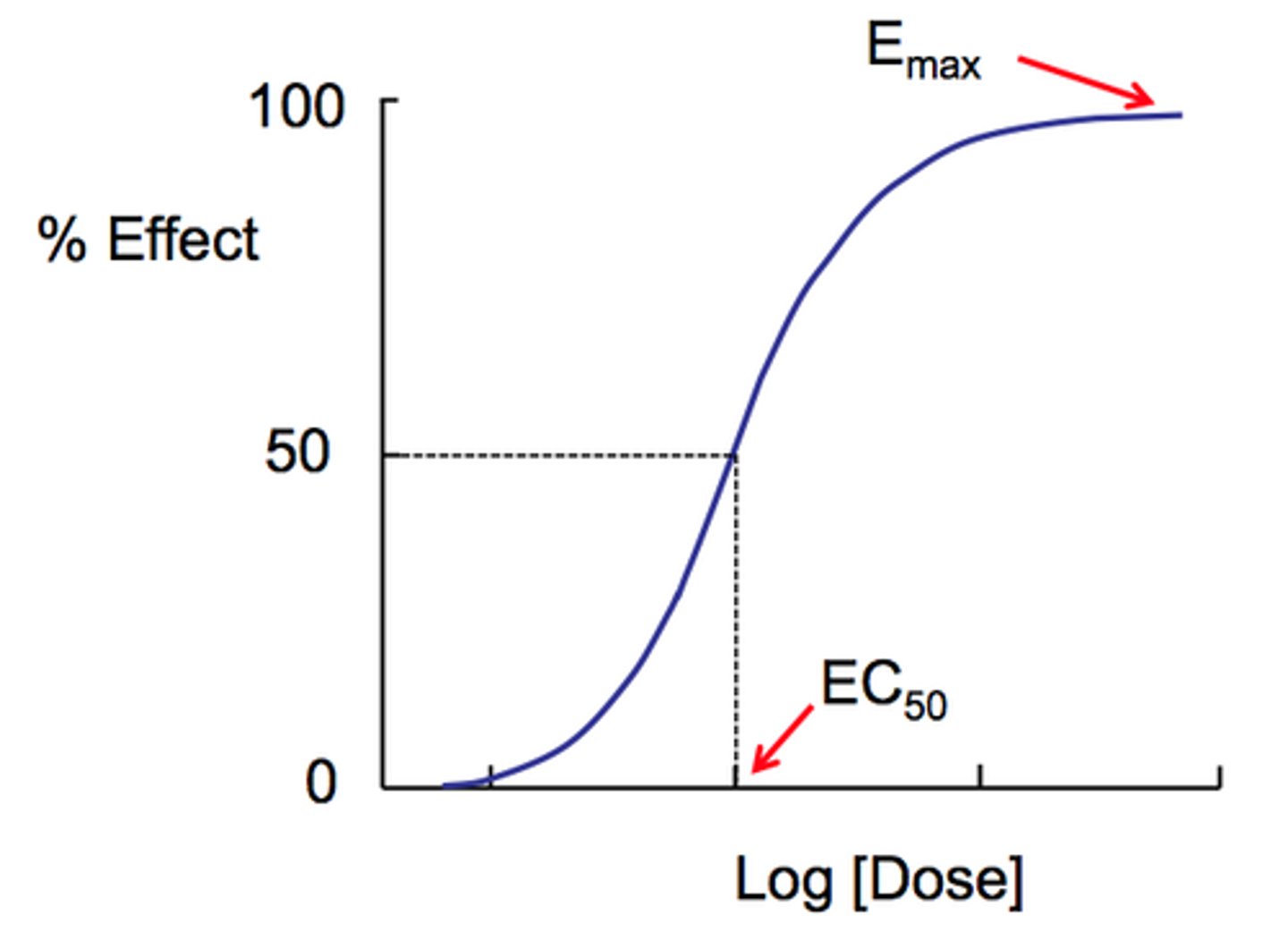
when can maximal efficacy be seen on a graph
plateau of concentration-effect curve
t/f: maximal efficacy is seen as a plateau on the concentration-time curve
false. concentration-EFFECT curve
maximal efficacy
-largest effect a drug can produce (determined by properties of drug and its receptor)
- may not be achievable bc of side effects
- NOT related to drug potency; maximal efficacy is of greater importance
efficacy vs potency? which has greater clinical importance?
Efficacy is the maximal response a drug can produce
Potency addresses how much drug (concentration or dose) to administrate for eliciting a desired response
-maximal efficacy is of greater importance
what compares the relative effectiveness of drugs acting by similar mechanisms
potency [cannot be used for drugs w different mechs!]
t/f: a drug with higher potency has greater efficacy
false. higher potency just means we may need to give less of a drug to have effect. less potent means you need to give more
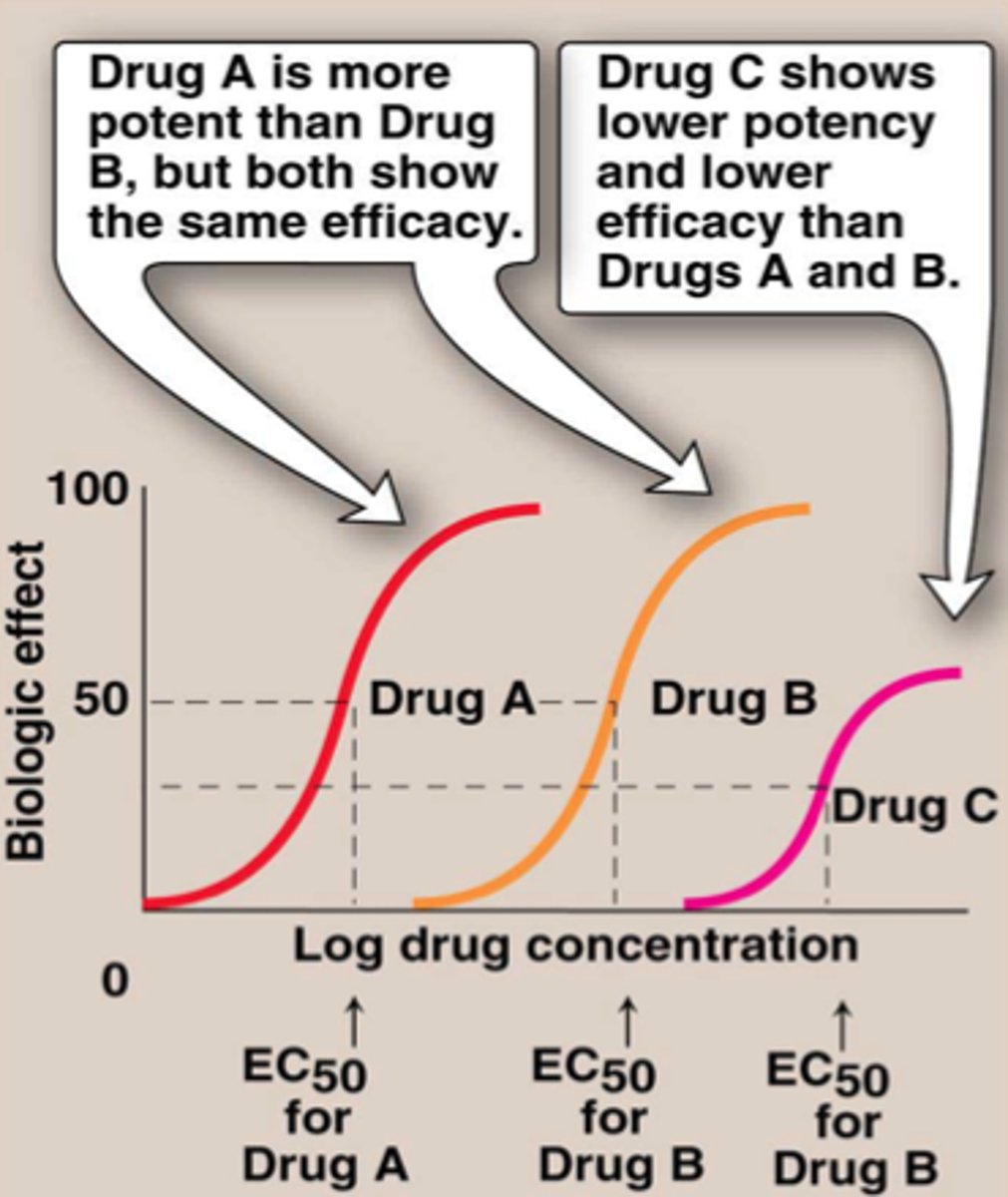
describe the difference in a more potent drug, less potent drug, and lower efficacy drug on a concentration-effect curve
-more potent drug needs less doses (lower concentration)= shift left
-less potent drug needs more doses (higher concentration)= shift right
- drug with lower efficacy= shift down
can 2 drugs with different potencies have the same efficacy
yes. just need more doses of the less potent drug, but they can both reach the same efficacy
____= the magnitude of response is decreased by subsequent drug doses of the same size as the initial dose
tolerance
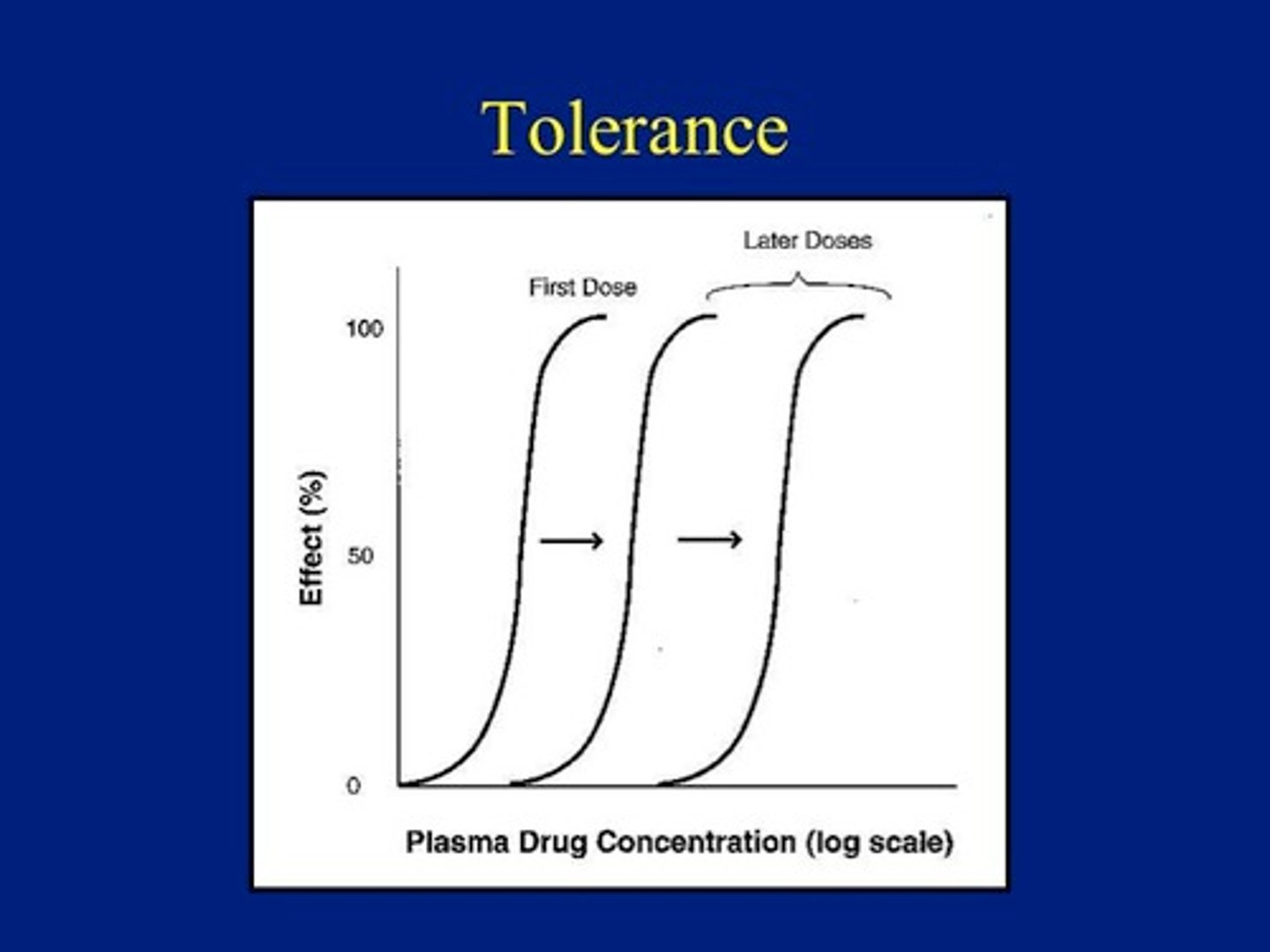
what can cause tolerance to a drug (summary)
- decreased concentration of drug at target (ex: increased protein binding)
- down regulation of receptors
- increased clearance rate (ex: increased blood flow, CO)
- PK adaptations (ex: faster metabolism, alcohol)
how can an increase in renal blood flow lead to tolerance
increasing RBF causes an increased clearance rate, which requires a higher dose of a drug
why do normal doses of drugs not work on chronic alcohol users
frequent alcohol use often leads to induction and faster metabolism of drugs= tolerance
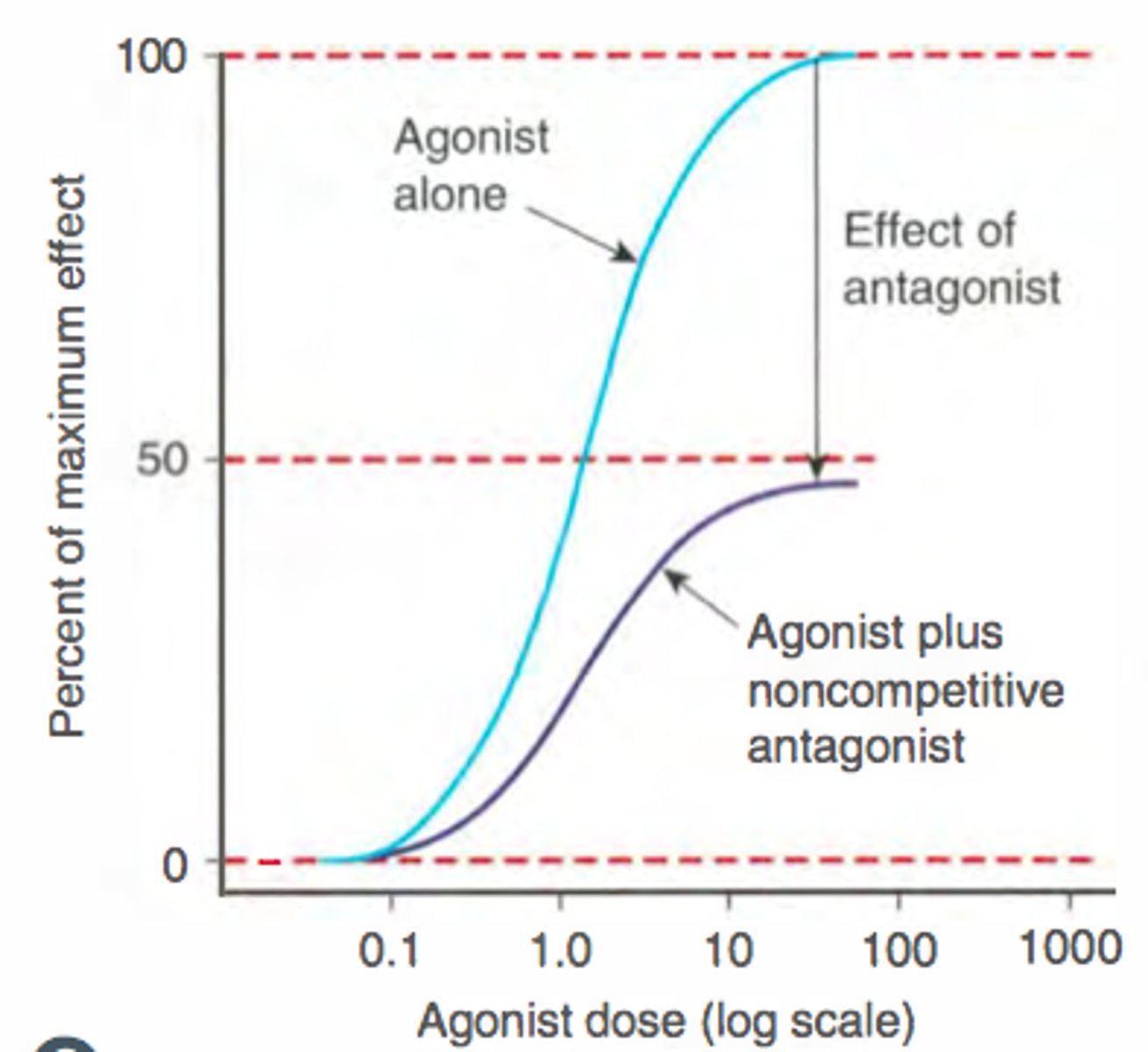
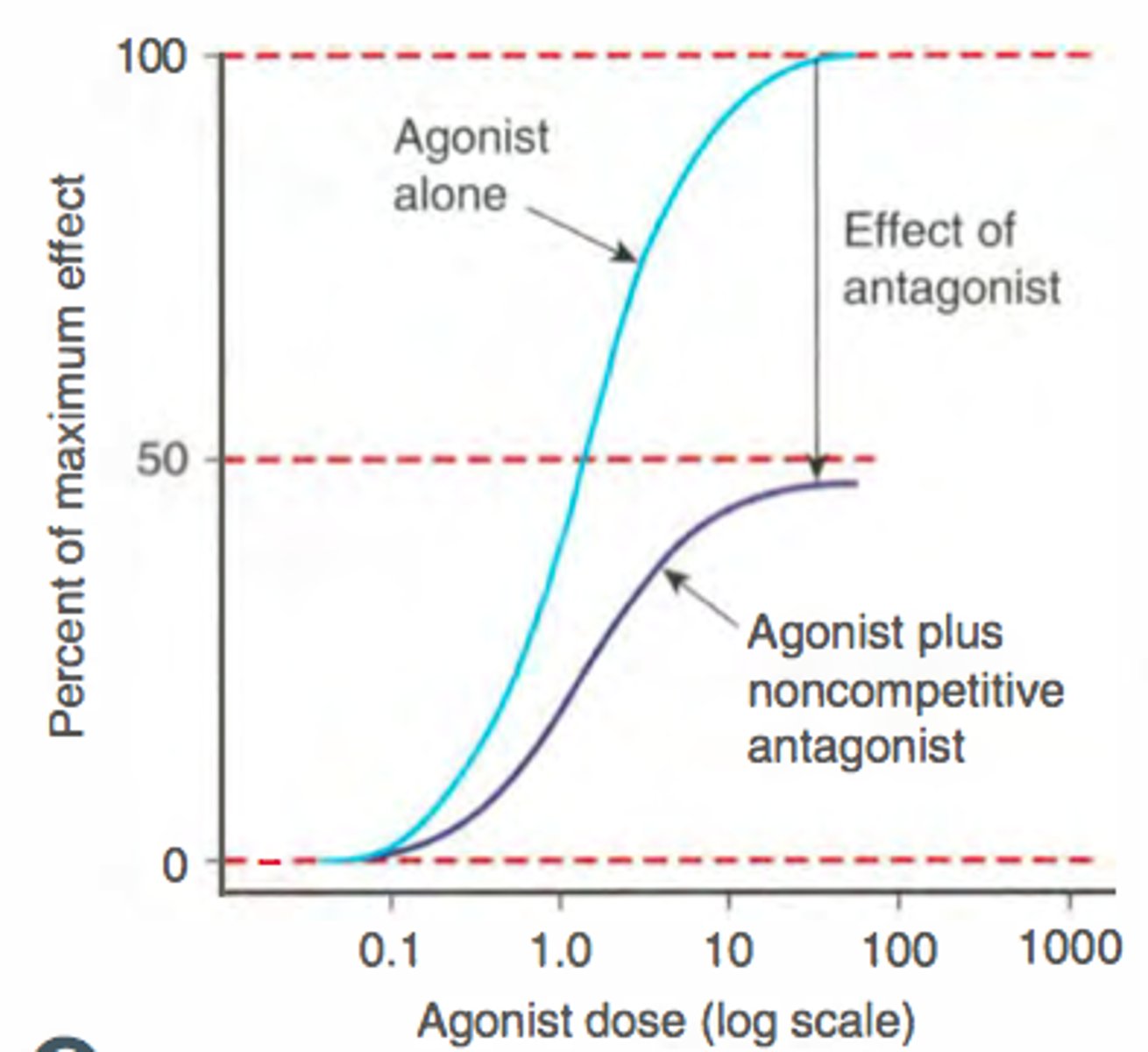
non competitive antagonist
what is it?
effect on ce curve?
-binds to a site different from the agonist, changing the receptor site; not allowing the agonist to bind
- drug + noncomp ant= shift down (lower effect always bc u cant outcompete)
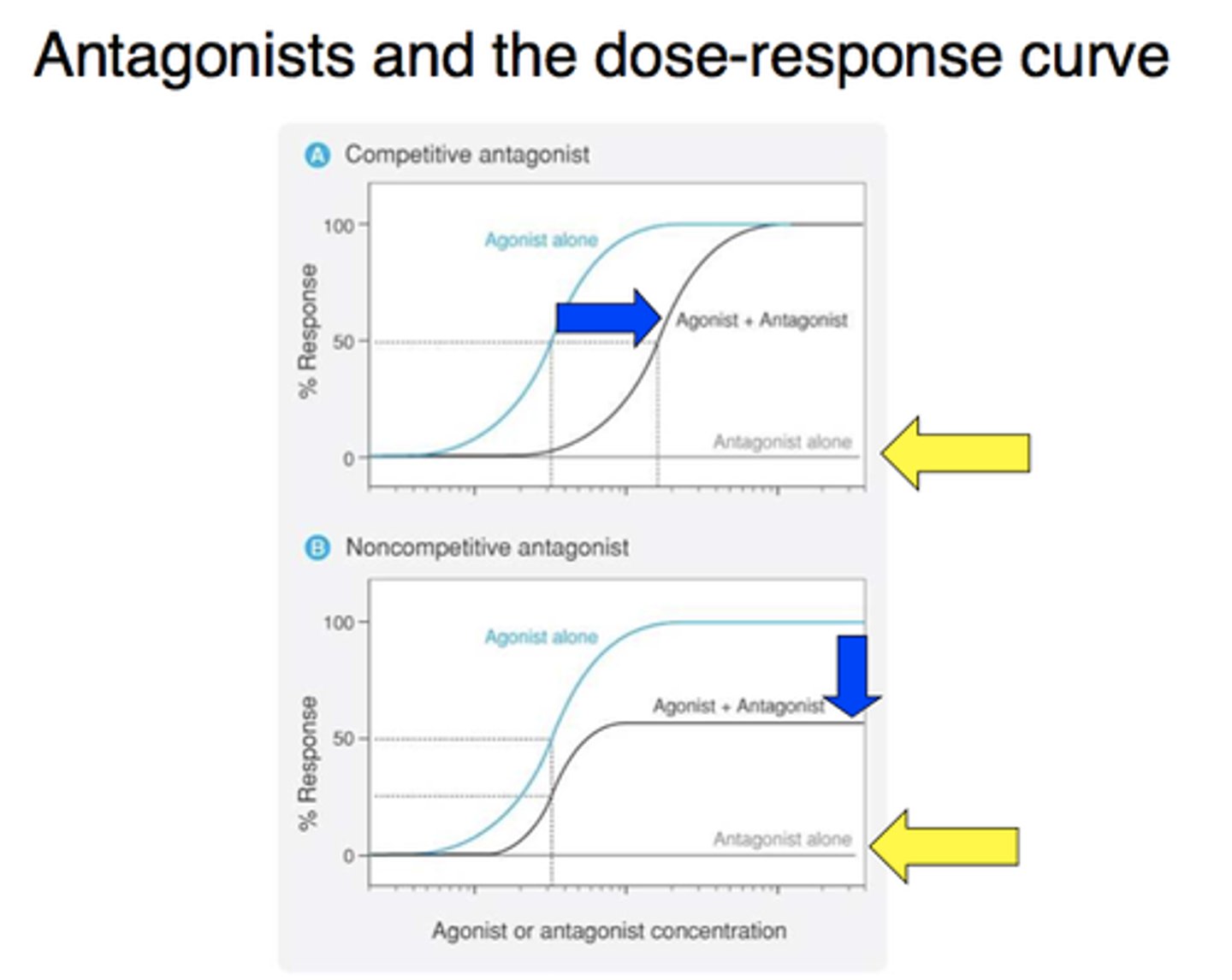
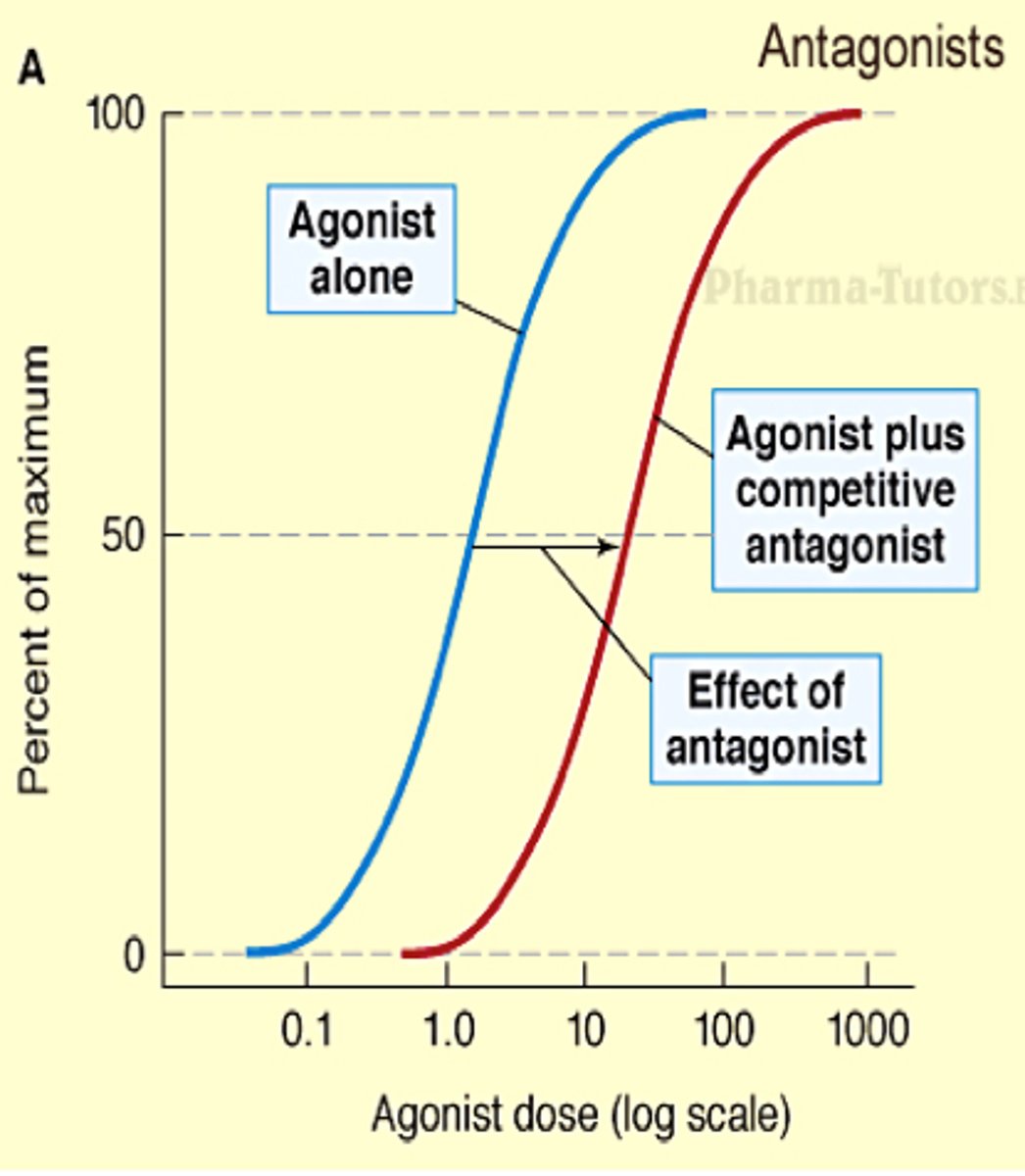
competitive antagonist
what is it?
effect on ce curve?
a pharmacologic antagonist that can be overcome by increasing the concentration of agonist
- drug + comp antag= shift right (need more of drug, but same efficacy)
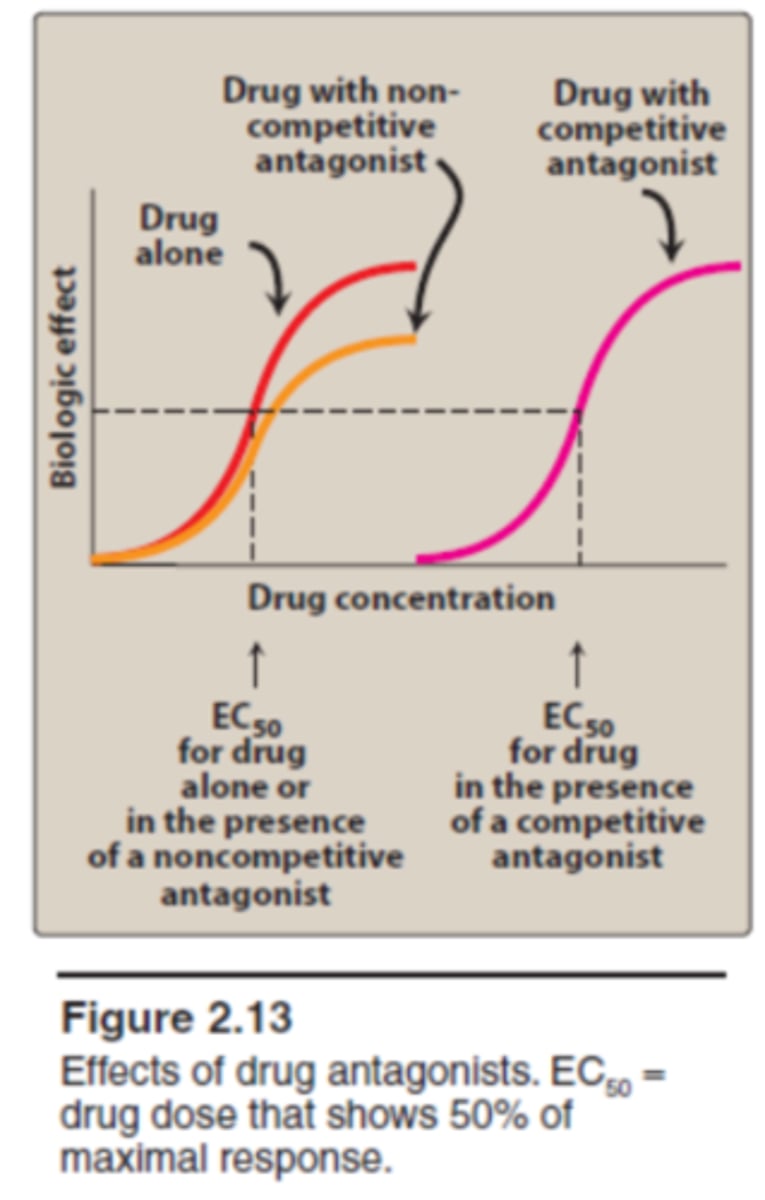
noncompetitive vs competitive antagonist effect on ce curve
drug+ noncompetitive antag= shift down (lower efficacy)
drug + competitive antag= shift right (can outcompete w higher dose to get same efficacy)
administration of a drug with a _____ antagonist would cause a shift down on the ce curve
non-competitive
administration of a drug with a _____ antagonist would cause a shift right on the ce curve
competitive
drug with partial agonist effect on ce curve
shift right + a little down
partial agonist is competing with the drug (shift right), will probs never reach 100% efficacy (small shift down)
compare concentration of drug needed to reach ED50s of drug with noncomp antag, comp antag, and partial agonist
noncomp antag= lowest dose needed (furthest to left)
- nothing at receptor, not a lot of drug needed
partial ag= middle
comp antag= highest dose needed (furthest to right)
- need more drug to outcompete
can we supercede the effects of a noncompetitive antagonist by increasing concentration
no. noncompetitive antagonist works at separate site to alter receptor. you will always have lower efficacy of a drug
can we supercede the effects of a competitive antagonist by increasing concentration
yes
ED50
Effective dose in 50% of the population
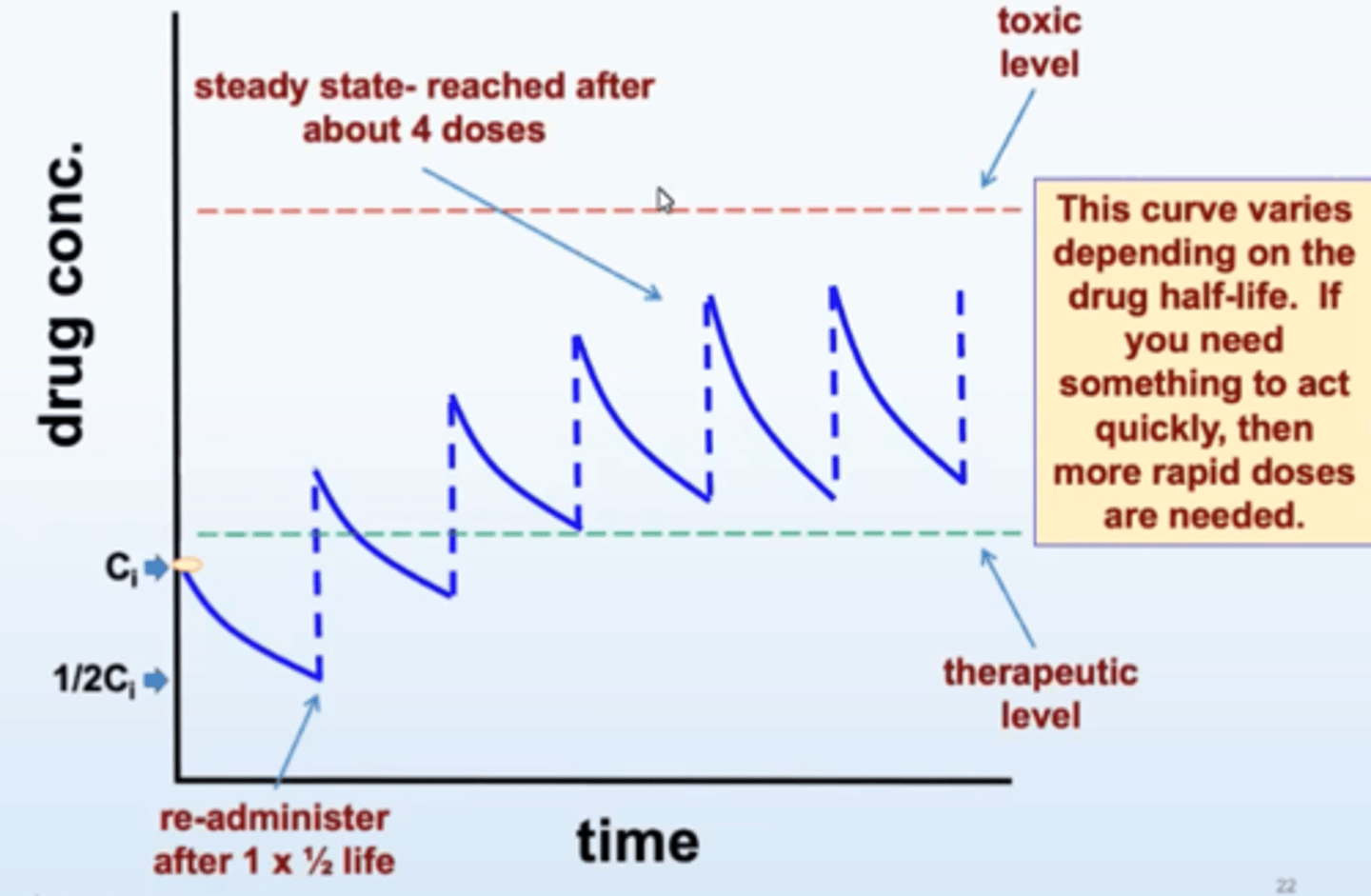
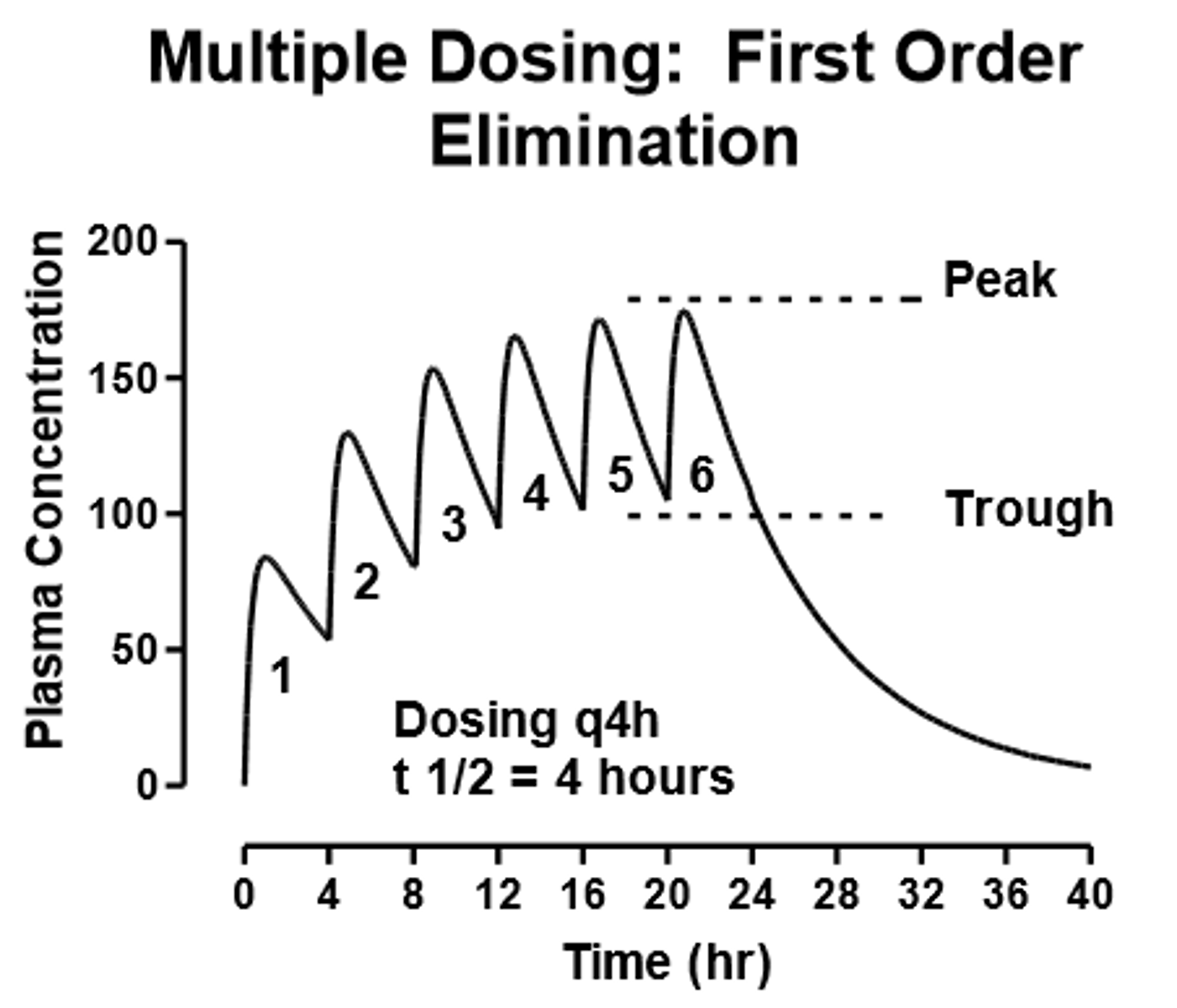
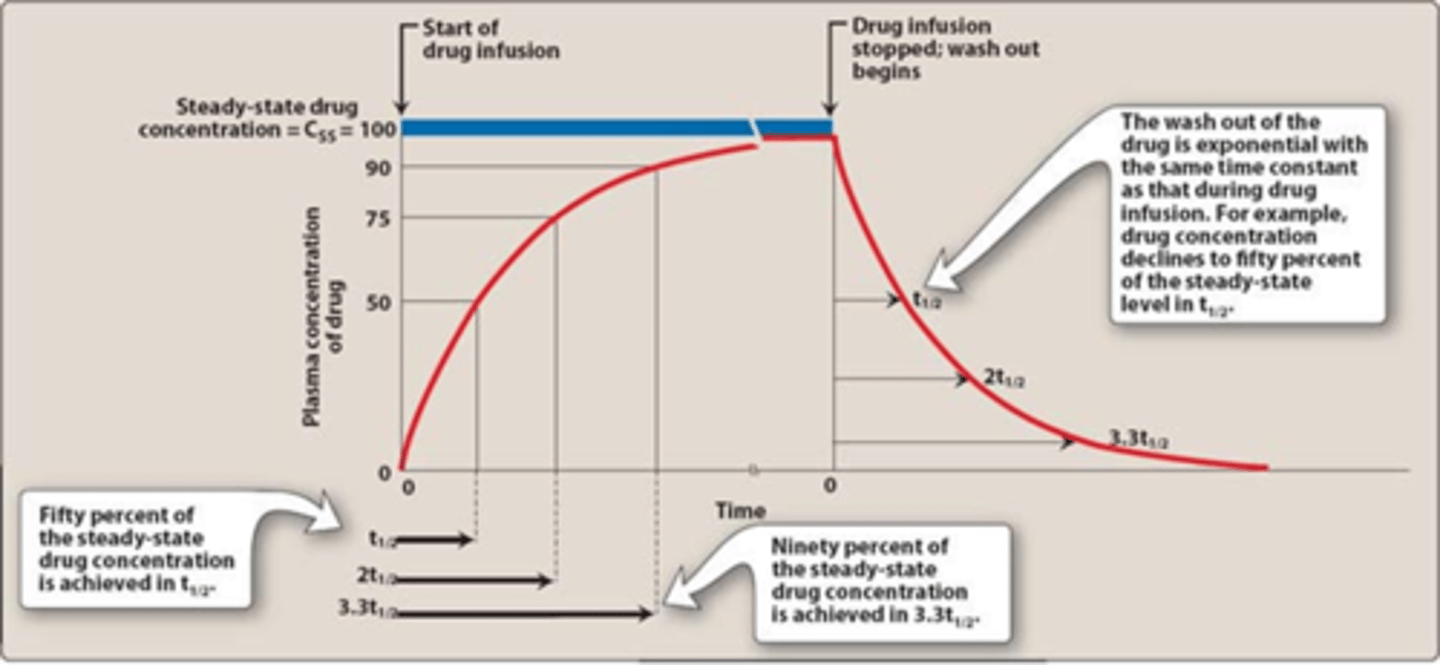
what is steady state
- concentration that will be achieved when a drug is administered at a constant rate
- rate of absorption equals the rate of elimination (horizontal line)
- achieved in about 4 half lives
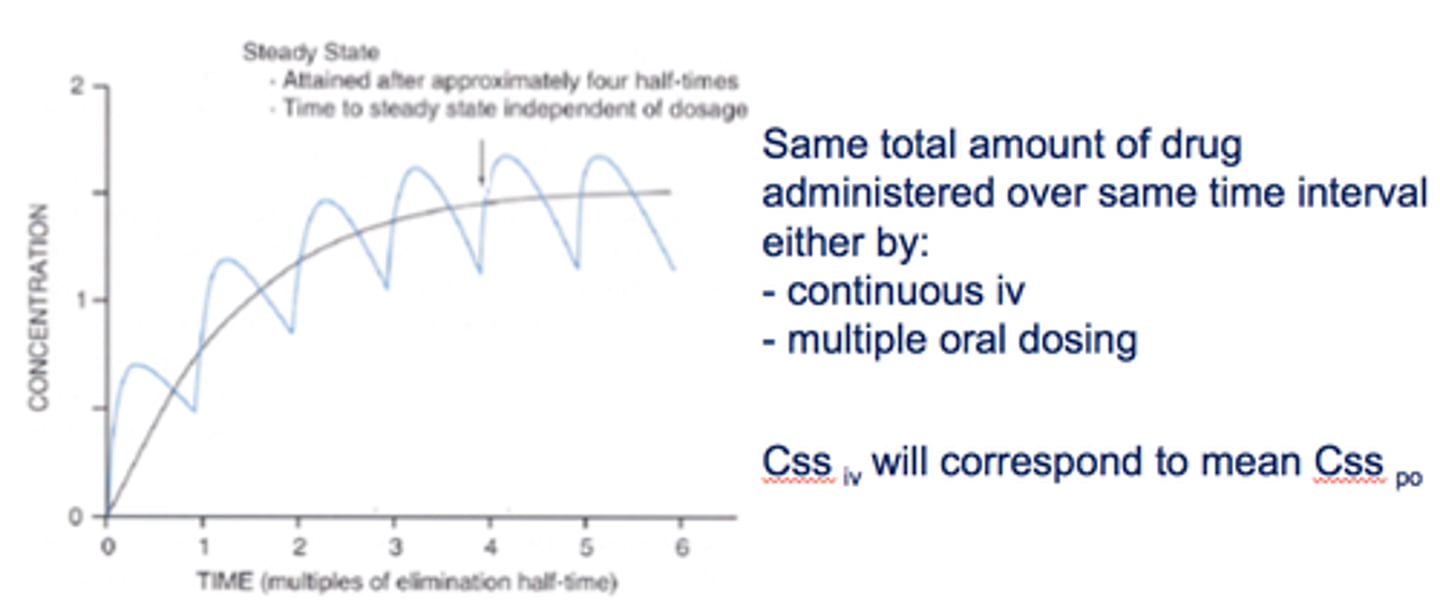
when is steady state attained
after 4 half lives
t/f: time to steady state depends on dosage
false. time to steady state is always 4 half lives, independent of dosage (this is when drug elimination is equal to absorption)
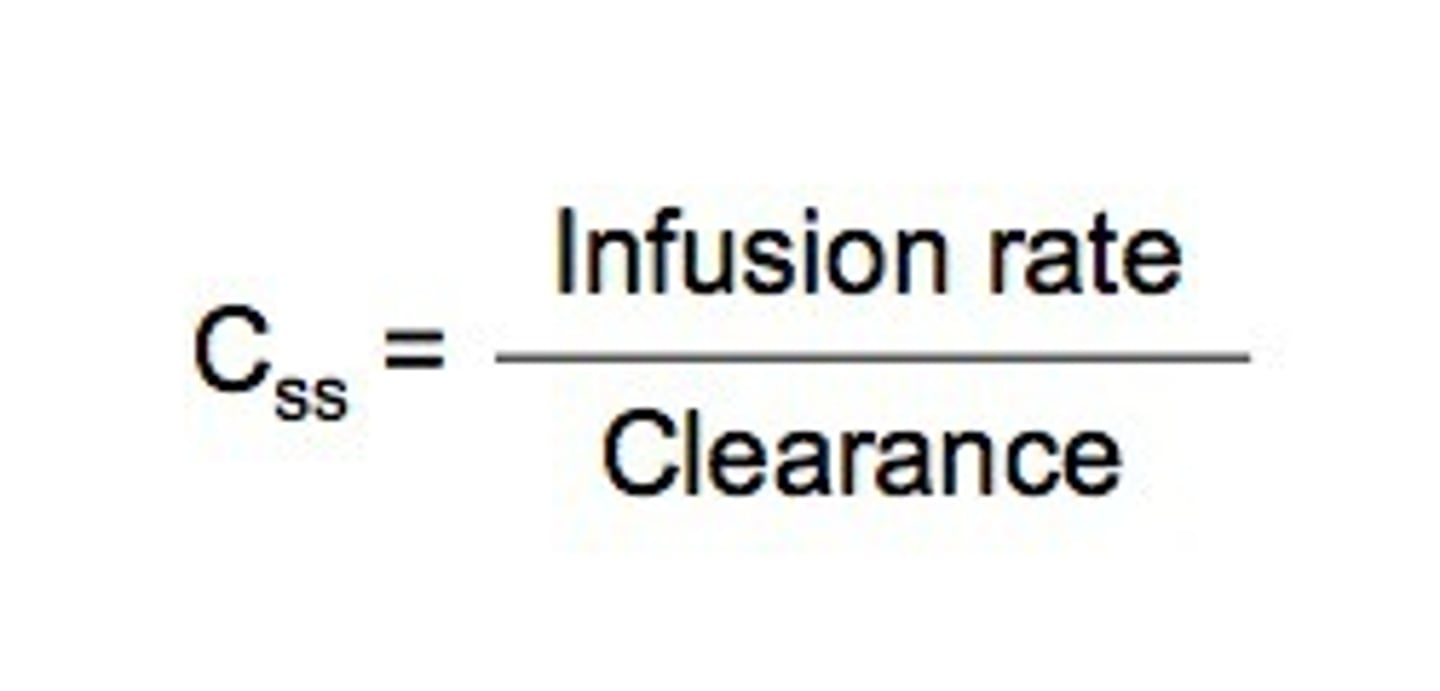
what is steady state proportional to
dose/dosage interval
F/CL (bioavailability/clearance) bc remember its when absorption equals elimination
after one half life, the drug concentration is ____% of steady state. what are the next?
one half life= 50%
two half lives= 75% (half of 50 is 25)
three half lives= 90% (+12.5)
four half lives= 100% (+6.125)
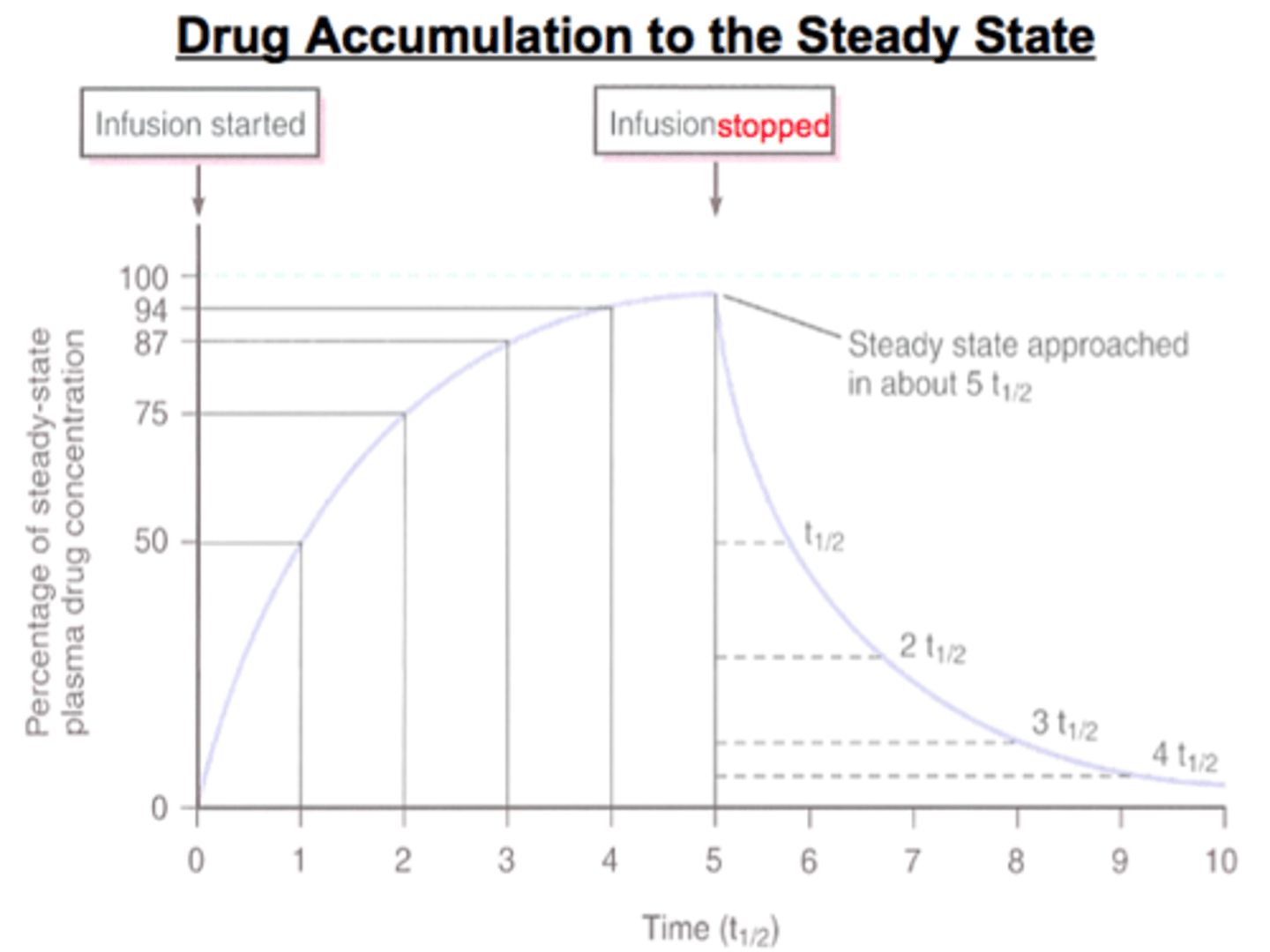
if steady state is 100mg, what concentration would be present at each half life?
100mg-> 50mg-> 25mg-> 12.5mg-> 6.125mg
(follows same pattern of half life)
if 50mg and 100mg of the same drug are injected, which one has a longer half life?
they have the same half life. remember half life is independent of dose. it will take the same time to decrease by half (and also same clearance RATE!)
if 50mg and 100mg of the same drug are injected, which one has a longer clearance rate?
same clearance RATE. 100mg will have more drug MOLECULES tho
t/f: regardless of dose injected, half life will be the same
true. time it takes to decrease by half is the same (just diff number of molecules)
will a higher or slower rate of infusion reach steady state faster
same time. 4 half lives always [but steady state concentration is different! meaning they have different effects!]
compare a faster vs slower rate of infusion on
time to half life
steady state concentration
- no difference in time to half life. half life for same drug will be the same bc its not dose dependant (always 4 half lives)
- a faster rate of infusion will have a higher steady state concentration (think of more drug accumulating bc elimination is constant)
t/f: a faster infusion rate will have a shorter half life and a larger steady state concentration than a slower infusion rate of the same drug
false. same half life, takes same time to reach steady state.
but it WILL have a larger steady state concentration. it will just take same time to reach it
if Drug A has a clearance rate of 5L/hr and Drug B has a clearance rate of 10L/hr, can these be the same drugs?
no. remember clearance rate is always constant for same drug, regardless of dose. so this cant be same drug
if Drug A has a clearance rate of 5L/hr and Drug B has a clearance rate of 10L/hr, which has a higher steady state concentration?
Drug A bc cleared slower
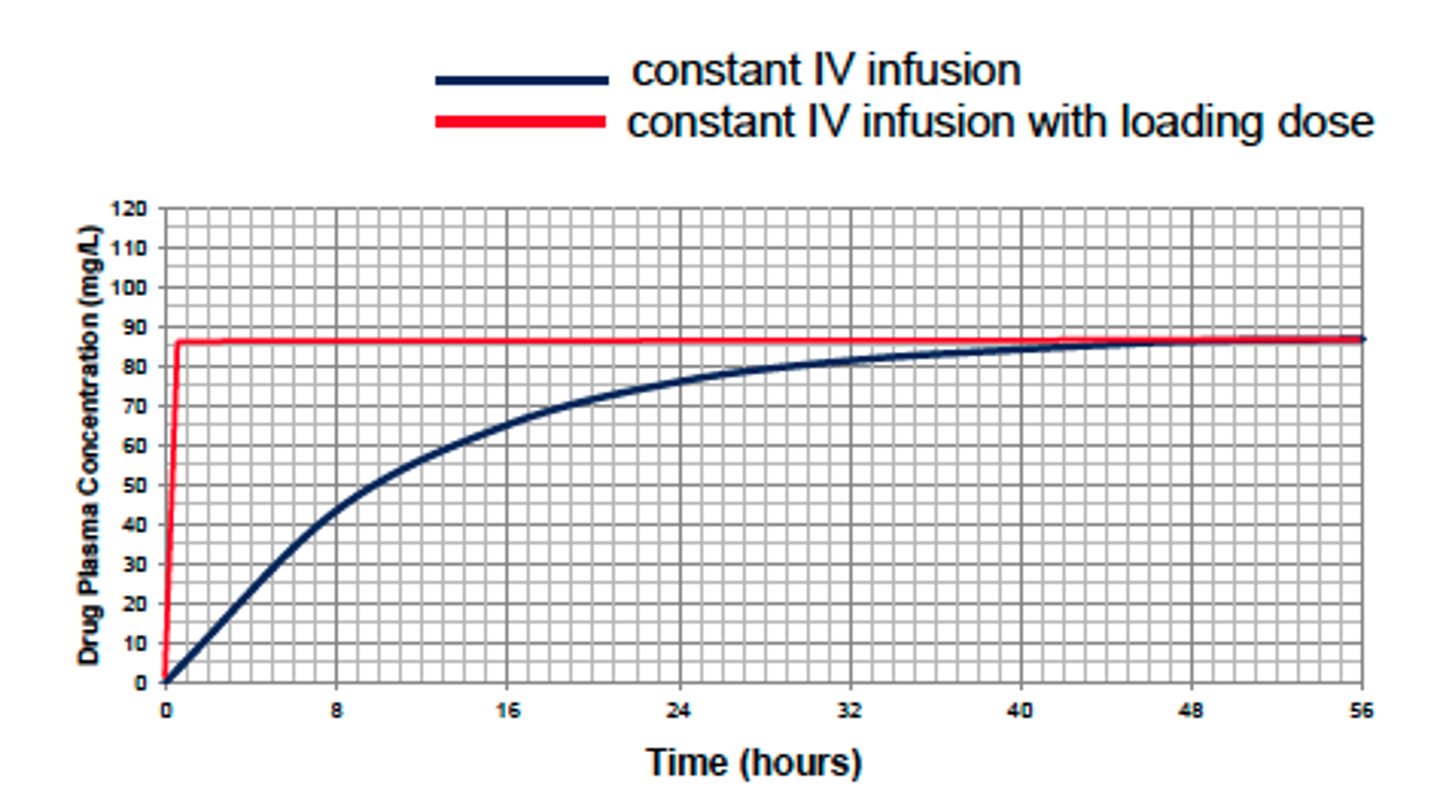
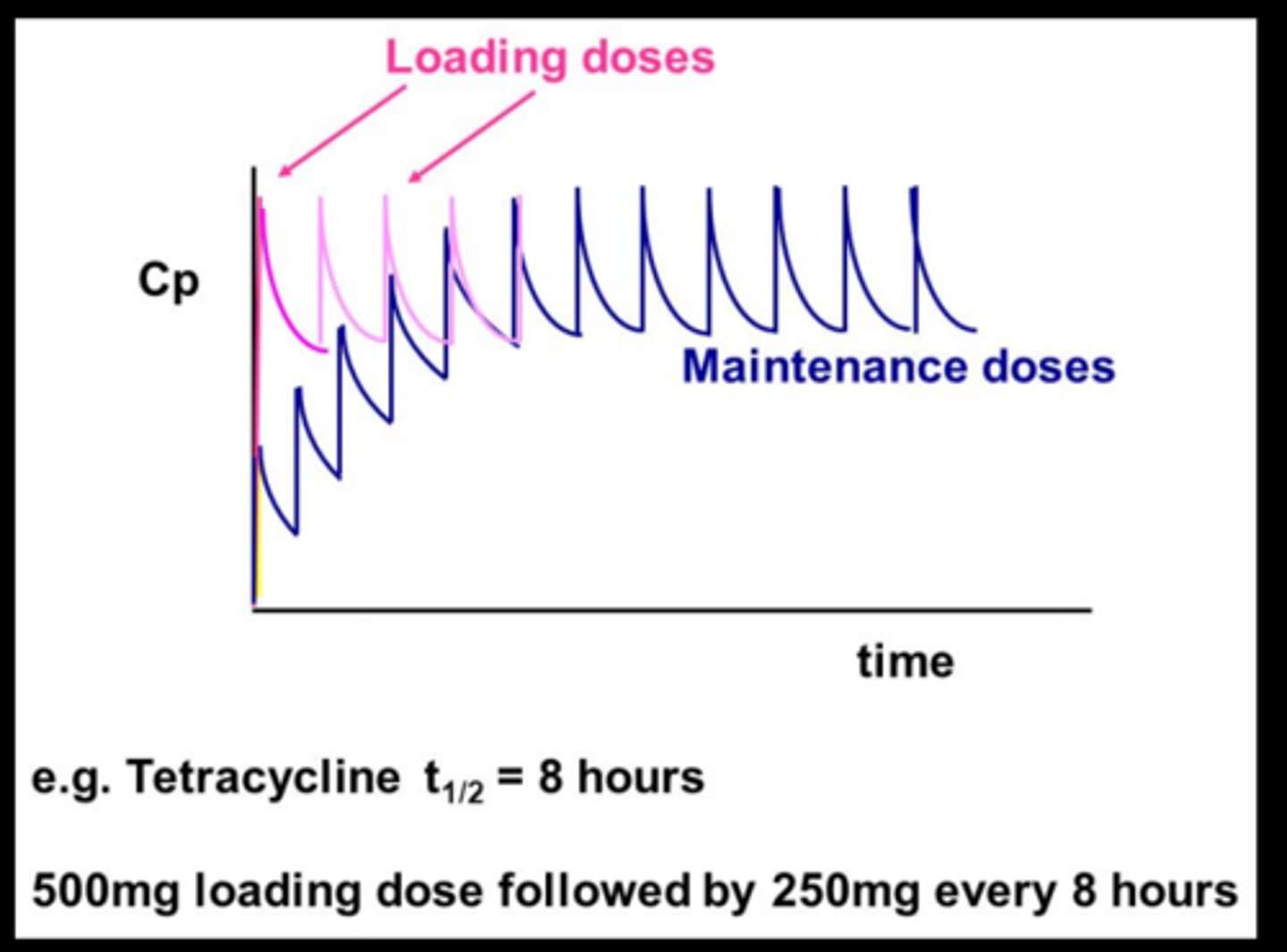
whats a loading dose
one or a series of doses given at the start of therapy to reach target concentration faster
how is loading dose calculated
Vd x desired ss concentration

what happens if the loading dose over or under shoots the steady state concentration
it will take 3-5 half lives to reach Css BUT the concentration will be closer to steady state concentration
[so still same number of half lives, diff initial concentration]
what happens if you overcalculate the loading dose
potential toxicity
will take 3-5 half lives to reach steady state
maintenance dose
drugs administered in a series of repetitive doses or as a continuous infusion in order to maintain a Css within a given therapeutic range
what does a dosing rate depend on? eq?
steady state concentration, clearance, bioavailability
dosing rate= (Css)(Cl/F)
t/f: a single oral dose may have a steady state concentration
false. a single dose just goes up and down.. you need accumulation to reach a steady state (multiple doses or constant infusion)
if a drug reaches steady state but continues to accumulate, what may be happening?
elimination is inhibited (bc absorption is surpassing; theyre not equal)
- could be renal issue
if a drug reaches steady state but begins to drop down, even though the pt is compliant with maintenance doses, what could be the reason?
acceleration of elimination (ex: increase in renal blood flow or glomerular filtration)
t/f: a higher drug concentration will be cleared faster
false. clearance rate is constant. a higher drug concentration will clear more drug molecules per unit time
t/f: a higher drug concentration will clear more drug molecules per unit time
true. but same clearance RATE
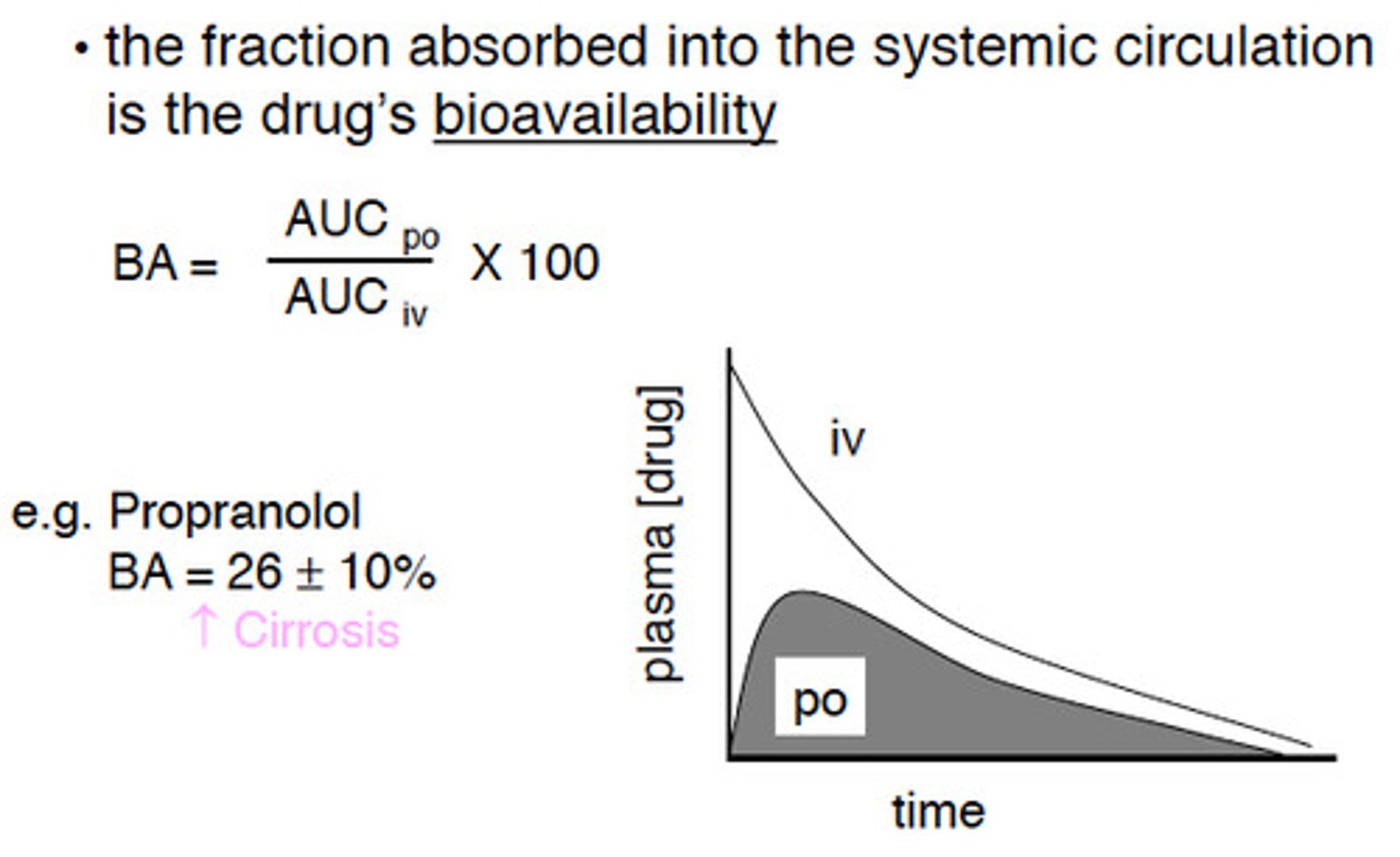
what is the bioavailability of an IV administered drug
100%
bioavailability of an orally ingested drug
(auc oral)/(auc IV) x 100
at low doses, drug metabolism is ____ order
at high doses (near steady state), drug metabolism is ____ order
low dose: first order (proportional to drug dose)
high dose: zero order (constant and independent of drug dose) bc enzymes are maxed out
which phase of metabolism is faster and dominant
phase 1
t/f: some drugs can directly enter phase 2 metabolism
true (ex: already polar, dont need phase 1)
steady state is exhibited by
a. first order kinetics
b. zero order kinetics
b. zero order kinetics