6. Opioid Med Chem
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
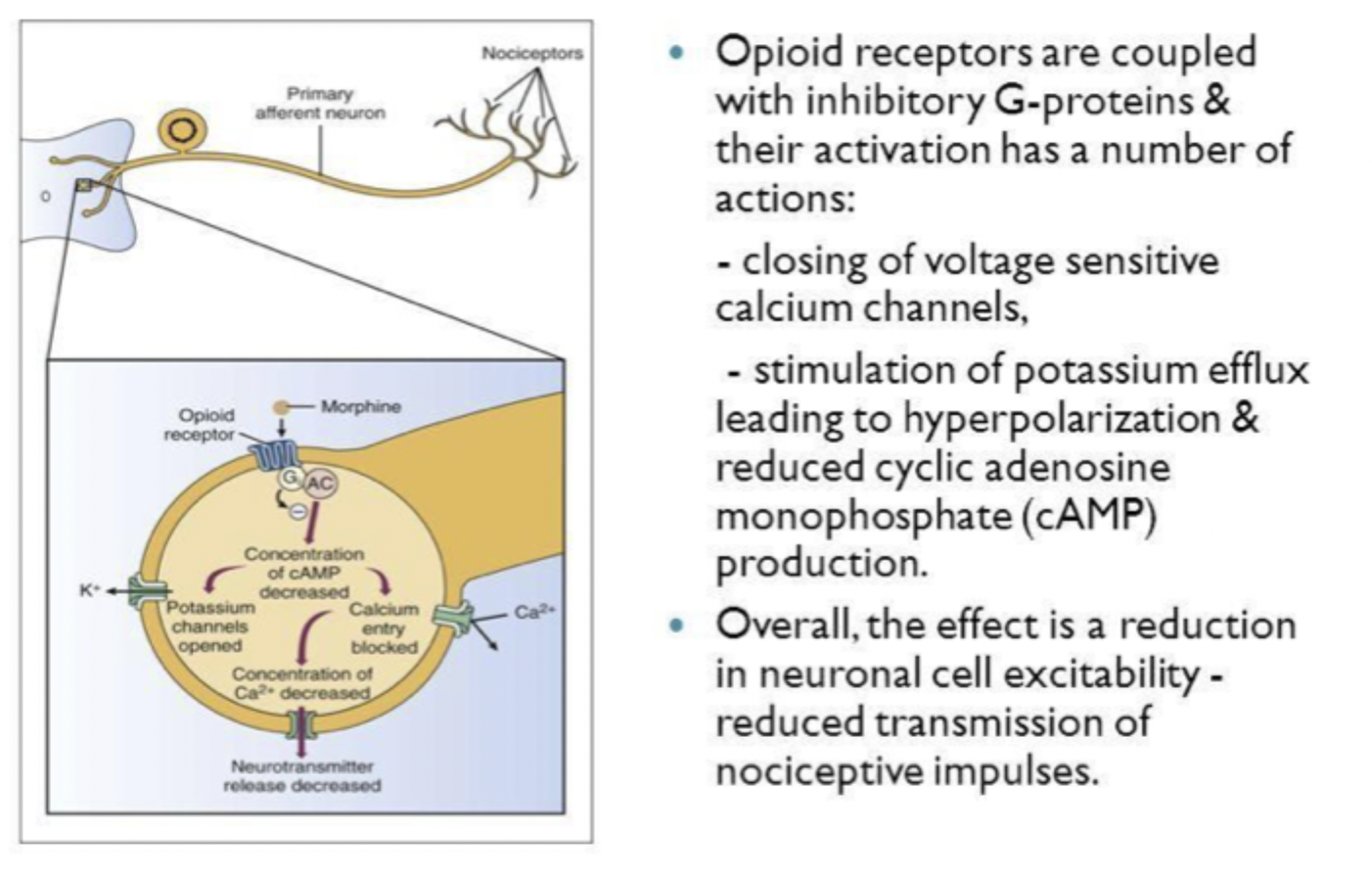
Mechanism of action
Opioid effects
Analgesia
Euphoria
Respiratory depression
Emetic effects
Constipation
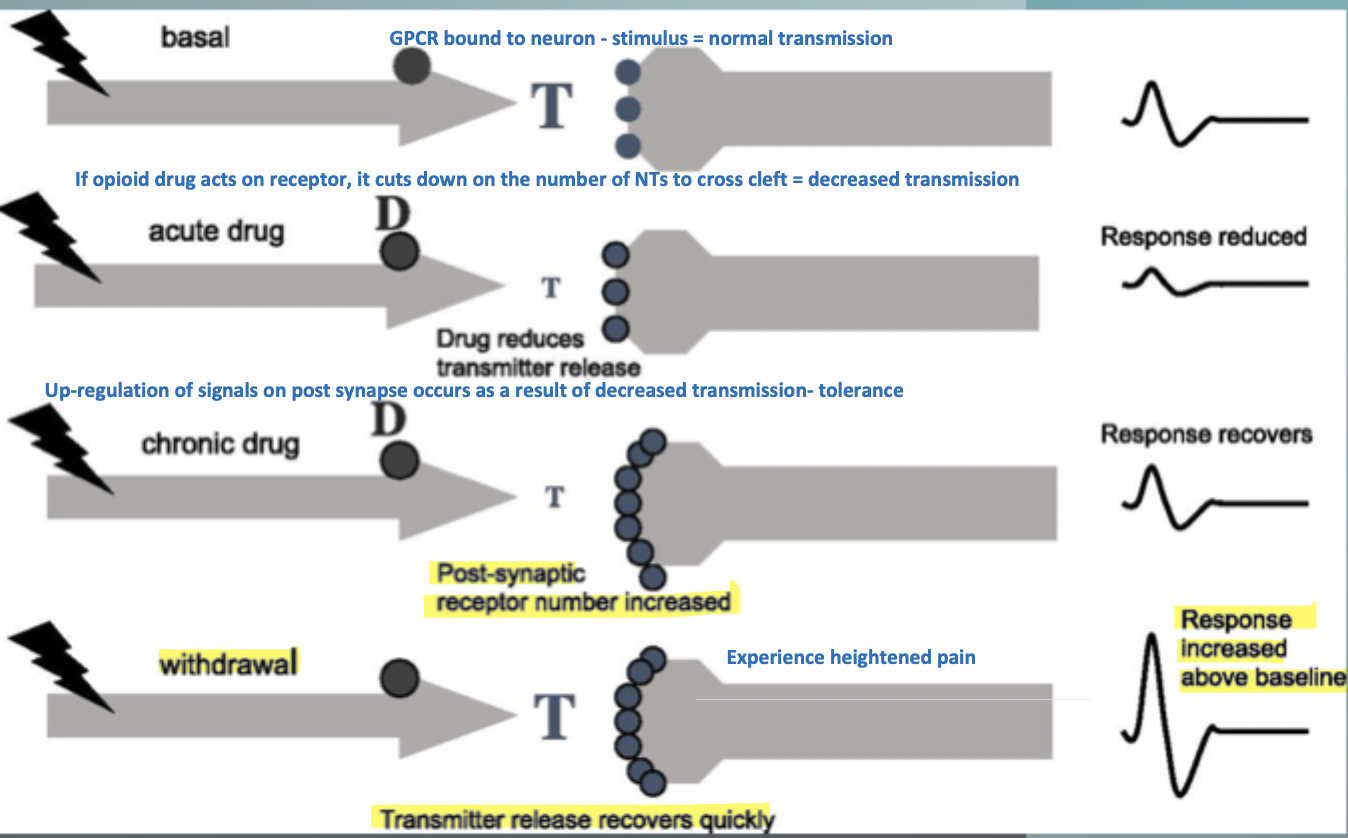
Tolerance/dependence
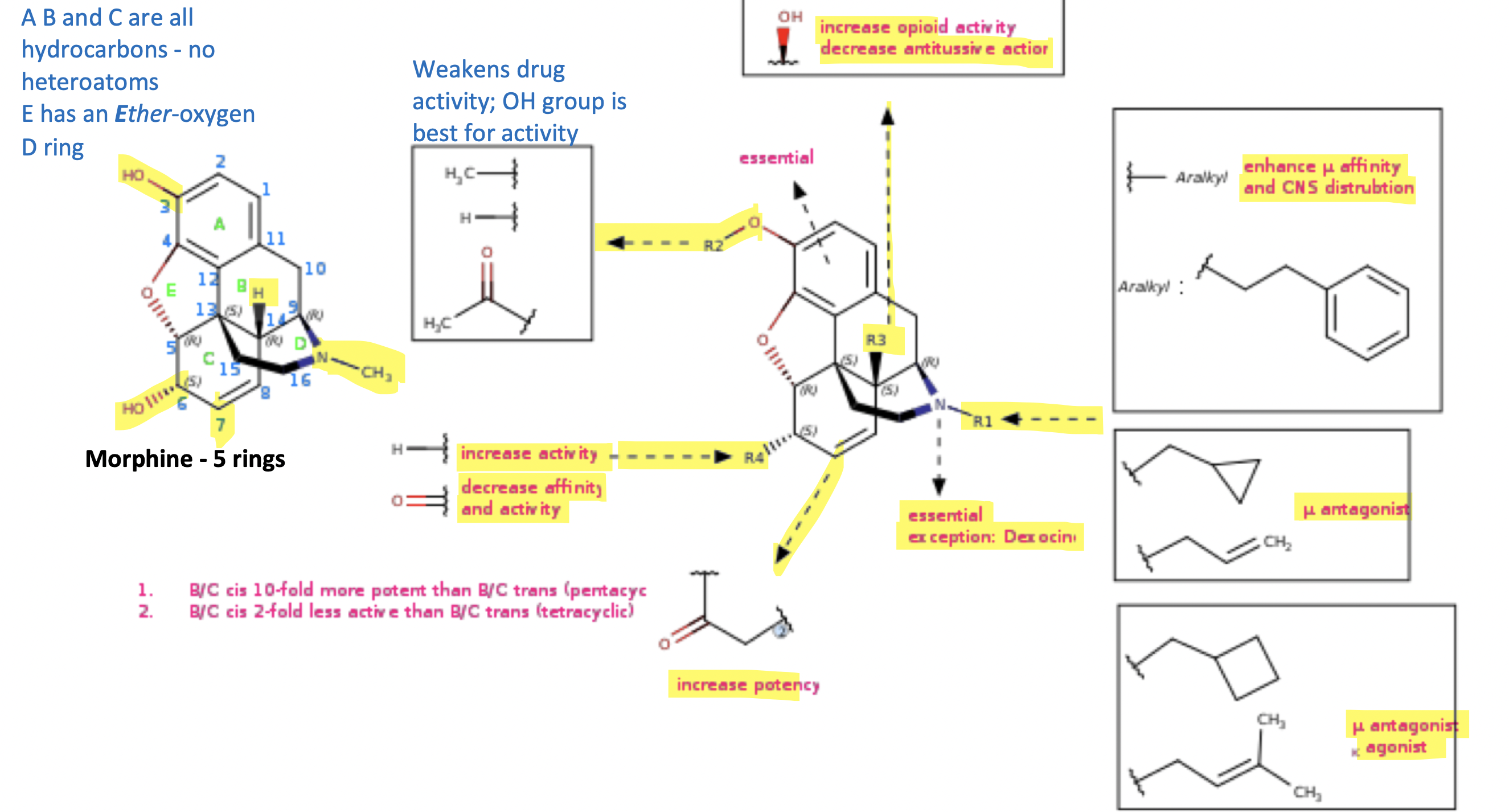
Opioid SAR
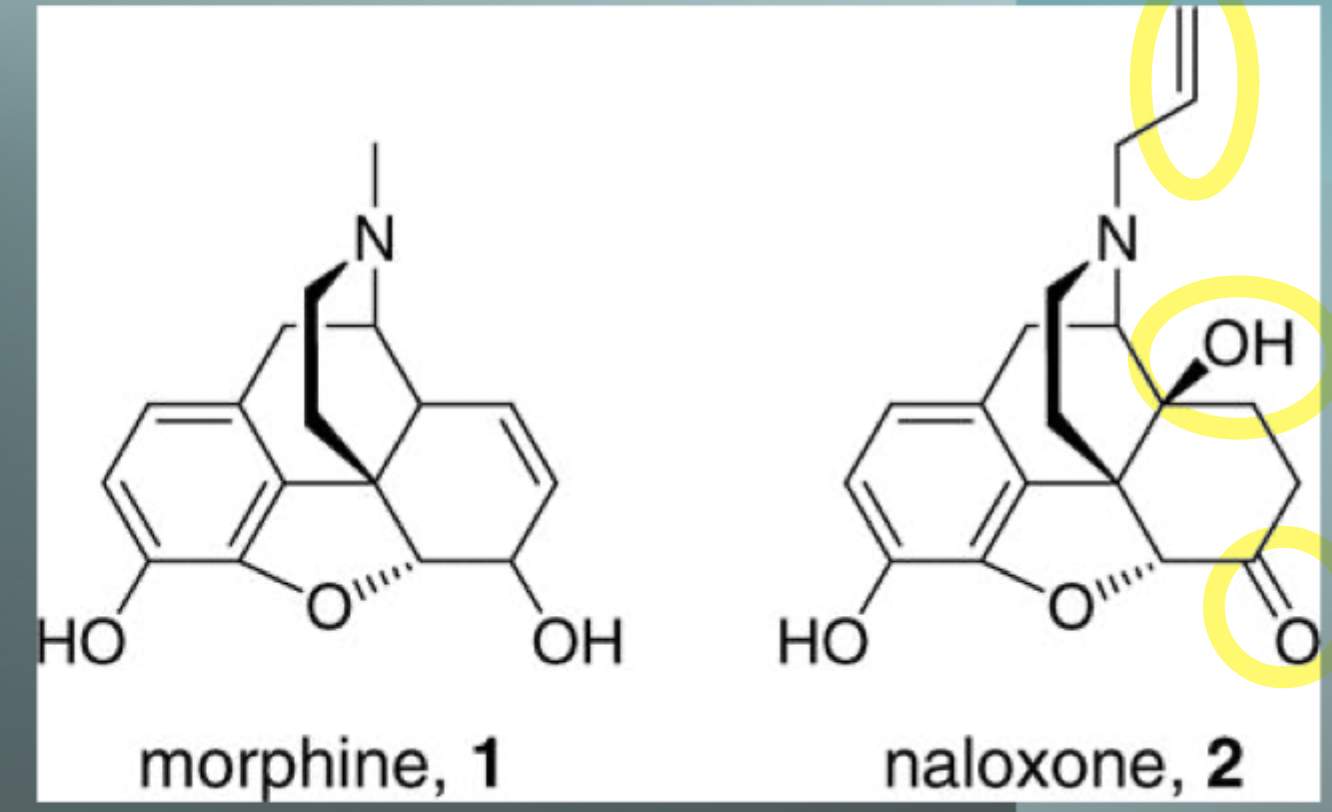
Exam question:
What is the difference between the morphine and naloxone molecule?
What is the structural difference between opioid agonists and antagonists?
In naloxone, the methyl group is replaced with an allylic group on the amino group, changing it from an agonist to an antagonist
Hydroxyl group changed to a ketone = higher affinity for the receptor, a more potent molecule
OH group added and no double bond changes from having cough suppression to something that is not going to have that activity
Opioid Agonists
Agonists activate the μ-opioid receptor and produce effects such as:
Analgesia
Euphoria
Respiratory depression
Sedation
Examples:
Morphine
Hydromorphone
Oxycodone
Structural Feature
Agonists typically have a small N-substituent, such as:
N-methyl (−CH₃)
Example:
Morphine contains an N-methyl group, making it a strong agonist.
Opioid Antagonists
Antagonists bind to the receptor but do not activate it.
They block the effects of opioids.
Examples:
Naloxone
Naltrexone
Structural Feature
Antagonists usually have a larger N-substituent, such as:
Allyl group (−CH₂CH=CH₂)
Cyclopropylmethyl group
These larger groups change how the molecule interacts with the receptor and prevent activation.
Examples:
Naloxone = N-allyl derivative of oxymorphone
Naltrexone = N-cyclopropylmethyl derivative
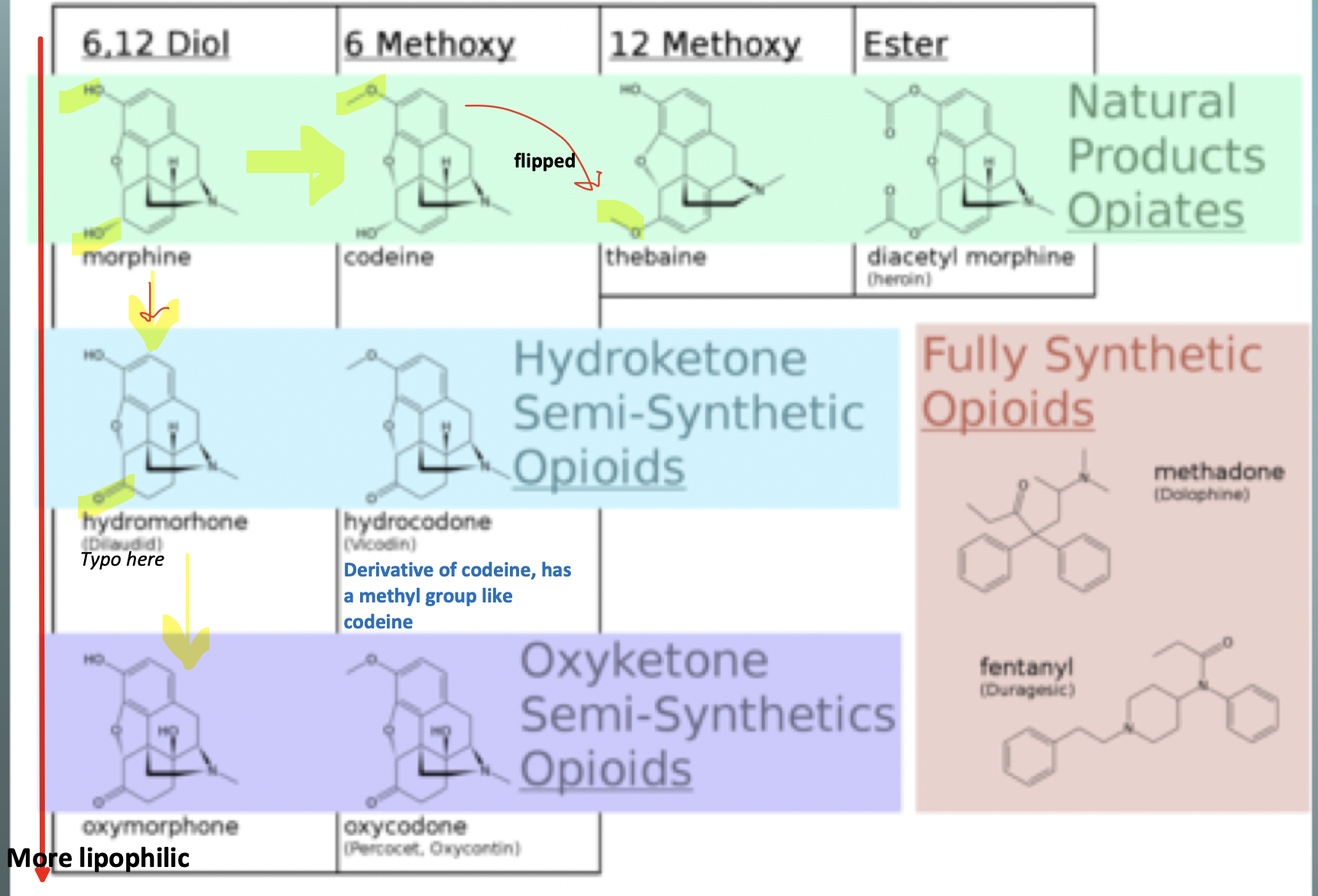
Exam question: What is the difference between morphine and heroin; why does heroin produce more intense euphoria than morphine
Lipophilicity
heroin enhanced lipophilicity allows for higher BBB penetration, higher concentration in CNS
then converted to morphine in that space
Heroin is a pro-drug for morphine
Heroin produces more intense euphoria than morphine because it is more lipid-soluble (more fat-soluble), so it crosses the blood-brain barrier much faster.
Once heroin enters the brain, it is rapidly converted into morphine, leading to a faster and higher concentration of morphine in the brain, which causes a stronger "rush" and more intense euphoria.
Simple memory:
Morphine: enters the brain slower → less intense euphoria
Heroin: enters the brain faster → more intense euphoria and "rush"
The reason heroin enters the brain faster is that its two hydroxyl (OH) groups have been acetylated, making it more lipophilic.
What is the structural difference between opioids that are cough suppressants and those that are not?
Cough suppressing opioids typically have the 3-phenolic OH methylated to a 3-methoxy group (OCH₃), as seen in codeine. This reduces analgesic activity while maintaining antitussive activity.
Memory Trick
3-OH = stronger pain relief (morphine)
3-OCH₃ = better cough suppressant (codeine)
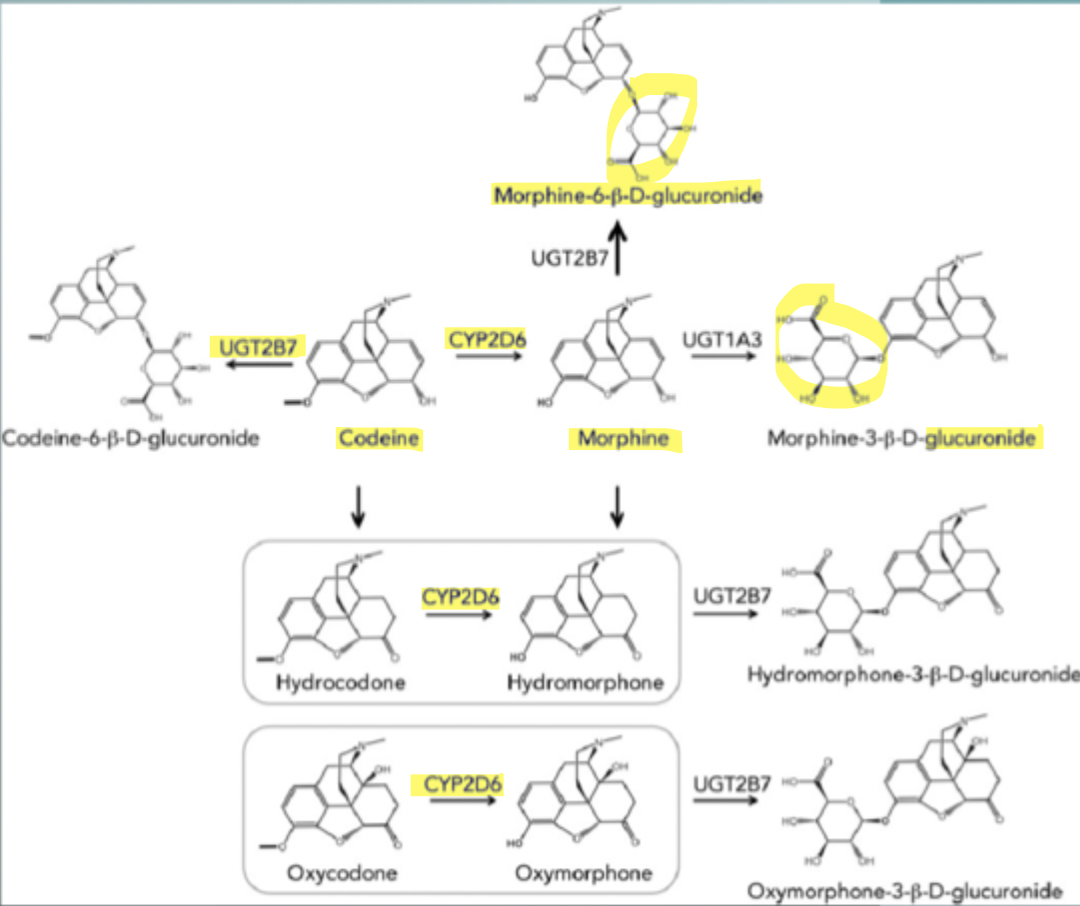
Opioid metabolism
metabolism occurs primarily in liver
metabolites excretes in urine - renal function important for effectively clearing metabolites and the drug molecule
codeine has analgesic activity, but it is weaker than morphine
CYP2D6 necessary for codeine conversion to morphine
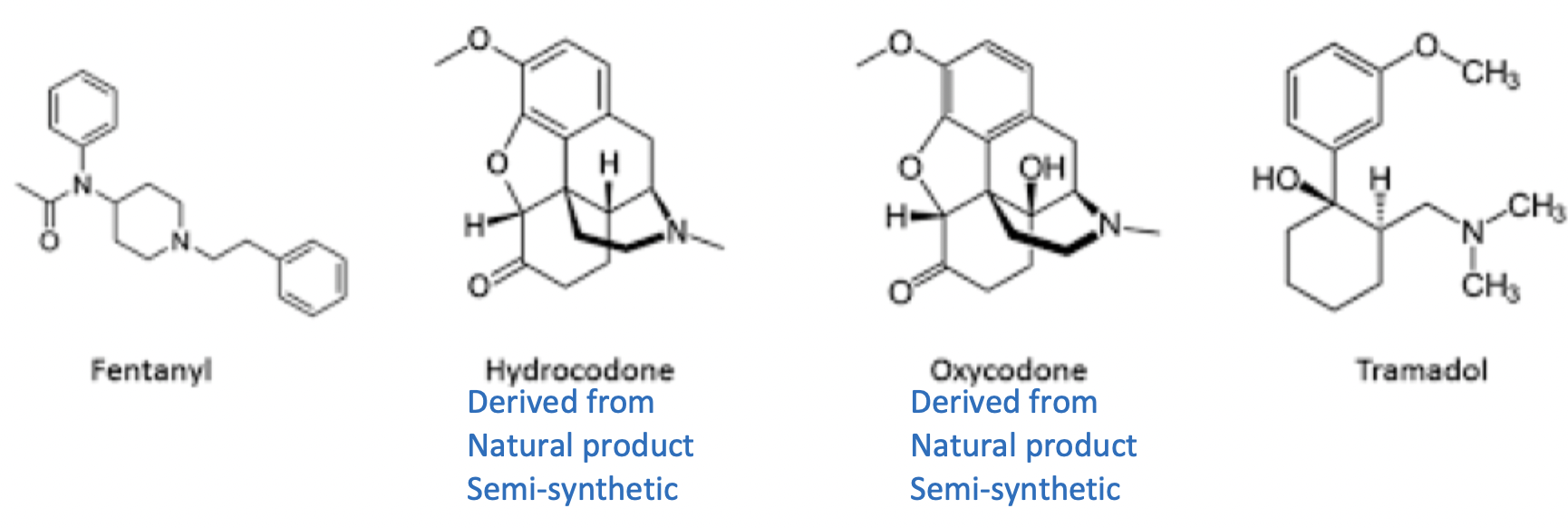
Other opioid agents (4)
Opioid disjunctive pharmacophore ID
Describe the general pharmacophore of natural product-based opioids
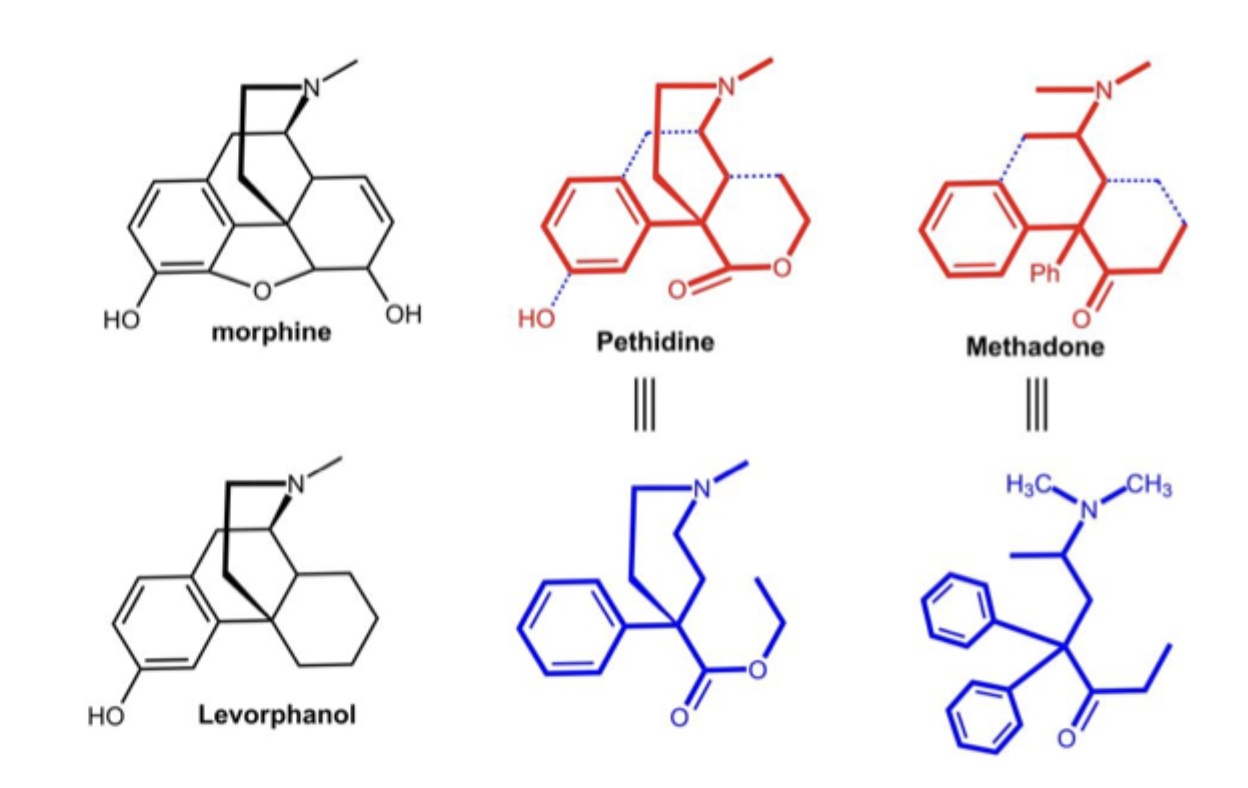
Start with morphine molecule:
Multiple fused rings, bridge structure, tertiary amine (nitrogen), oxygen-containing group that can hydrogen bind
Because of these rings, morphine is rigid
Morphine --> Meperidine (Demerol)
Remove some of morphine's ring systems created Meperidine
Even with these changes, Demerol still relieves pain and binds to opioid receptors
Morphine --> Methadone
Remove more structural complexity forming methadone, it looks even less like morphine but still act as an opioid
If morphine, meperidine, and methadone all activate opioid receptors despite looking different, they must share common essential features:
A basic nitrogen (Amine)
Positive charge interacts with negative charged site on the opioid receptor
An aromatic ring (usually a phenyl ring)
Provides hydrophobic interactions with the receptor
Oxygen containing group to participate in hydrogen binding
Phenol OH
Ether Oxygen
Carbonyl oxygen
Proper distance between the aromatic ring and nitrogen
The receptor cares less about the exact rings and more about:
Where the aromatic ring is
Where the nitrogen is
How far a part they are
The molecule can look completely different as long as these features are positioned correctly in 3D space
Why did removing the rings still work?
The rings mainly:
Hold the pharmacophore in a specific shape
Control flexibility
Affect potency and pharmacokinetics
But the rings themselves are not always required for receptor activation
Chemists learned that receptor recognizes the pharmacophore, not necessarily the entire morphine skeleton
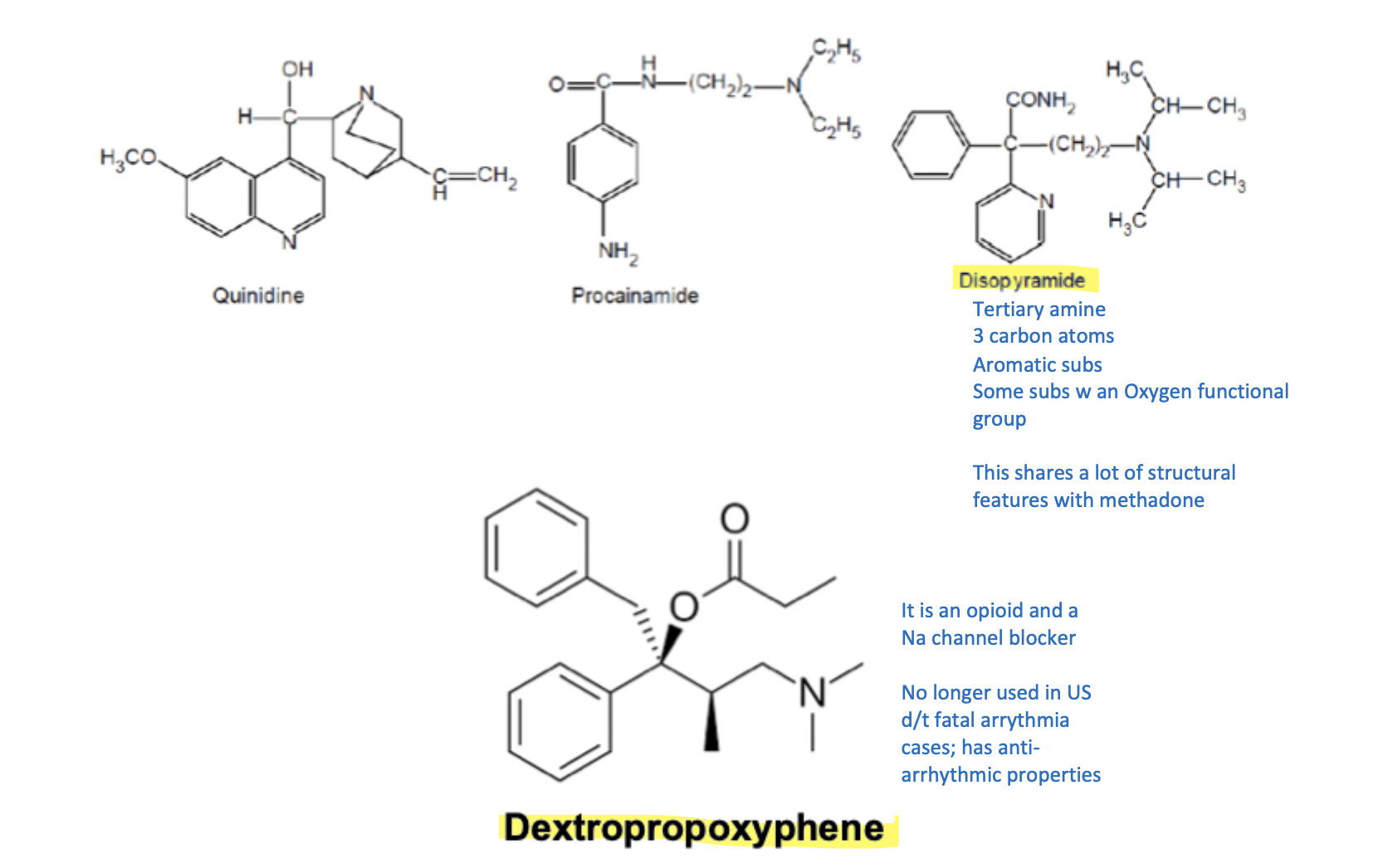
Opioid Pharmacophore Similar to Antiarrhithmics
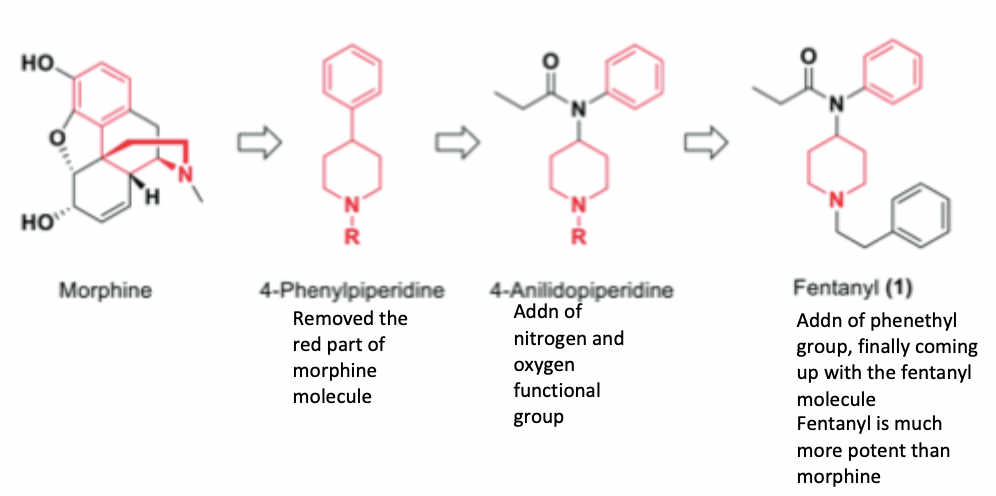
Fentanyl Discovery
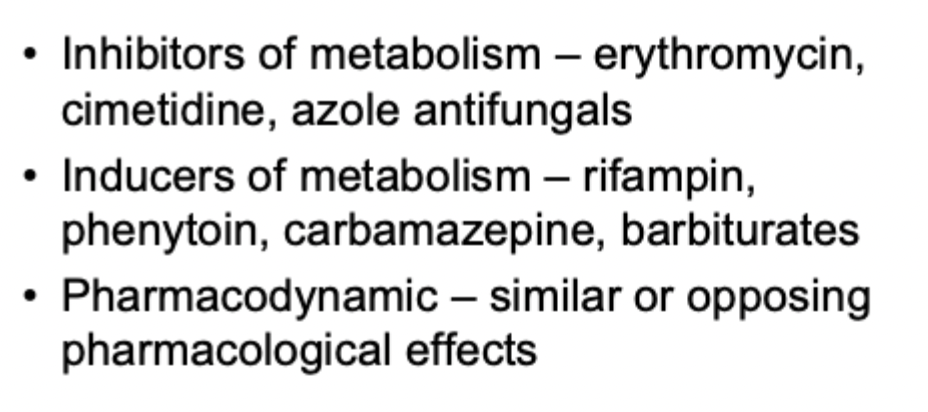
Opioid DDIs
Dosage forms
Morphones are often preferred rectally because they undergo more extensive first-pass metabolism and have lower oral bioavailability, so rectal administration can increase systemic exposure. In contrast, -codones already have good oral bioavailability, making the rectal route less advantageous.
Are there potential clinical uses with use of opioids in patients polymorphic in enzymes responsible for metabolizing opioids?
Yes. Genetic polymorphisms in opioid-metabolizing enzymes (especially CYP2D6) can be used to individualize opioid therapy. Poor metabolizers may not obtain analgesia from prodrugs like codeine, while ultrarapid metabolizers may experience toxicity. Therefore, genotype-guided opioid selection can improve efficacy and safety.
CYP2D6 Polymorphism
Poor Metabolizers (PMs)
They have little or no CYP2D6 activity.
Codeine is poorly converted to morphine.
May get little or no pain relief.
Similar issue with Tramadol.
Clinical use: Avoid codeine/tramadol and choose opioids that do not require CYP2D6 activation (e.g., morphine, hydromorphone).
Ultrarapid Metabolizers (UMs)
They have very high CYP2D6 activity.
Convert codeine to morphine very quickly.
Can develop excessive opioid effects:
Sedation
Respiratory depression
Toxicity
Clinical use: Avoid codeine/tramadol because of overdose risk.