emt 29 30 31
1/151
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
152 Terms
3 components of circulatory system
Heart (pump), vessels (pipes), blood (fluid)
Arteries function
Carry oxygenated blood AWAY from heart (high pressure)
Veins function
Return deoxygenated blood TO heart (low pressure, valves)
Capillaries function
Exchange oxygen, nutrients, waste with cellls
Perfusion vs hypoperfusion
Perfusion = normal oxygen delivery
Hypoperfusion = inadequate → shock
Definition of shock
Inadequate perfusion → cells don’t get oxygen → organ failure
4 causes of shock
Volume loss
Pump failure
Vessel dilation
Obstruction
Hypovolemic shock
Loss of blood or fluid → ↓ volume
Hemorrhagic shock
Specific type of hypovolemic shock from blood loss
Absolute vs relative hypovolemia
Absolute = Actual loss of blood or fluid from the body
Relative = Blood is still in the body, BUT vessels get bigger or fluid shifts out
Cardiogenic shock
Heart fails to pump effectively (MI, CHF)
Distributive shock
Blood vessels lose tone and dilate → pressure drops → blood isn’t effectively delivered to organs
Anaphylactic shock
Severe allergic reaction → vasodilation + permeability
Neurogenic shock
Shock caused by loss of nervous system control of blood vessels (usually from spinal cord injury)
Low blood pressure (hypotension)
Slow heart rate (bradycardia)
Warm, dry skin (no sweating below injury)
Septic shock
A type of distributive shock caused by a severe infection → body-wide inflammatory response → vasodilation + leaky vessels
Obstructive shock
Shock caused by a physical blockage that prevents blood from moving through the heart/lungs (PE, tamponade, tension pneumo)
Which cells die fastest?
Brain + heart (minutes)
What happens during compensation?
Body tries to maintain perfusion
3 compensation methods
Fluid retention (kidneys)
Vasoconstriction
↑ HR + ↑ RR
What triggers compensation?
Baroreceptors + chemoreceptors
Fight-or-flight response effect
Epinephrine → ↑ HR, vasoconstriction, sweating
Compensated shock
Early stage of shock where the body is still maintaining blood pressure using compensation.
If BP is normal BUT:
fast HR
fast RR
pale skin
Decompensated shock
The stage of shock where the body’s compensation fails → it can no longer maintain blood pressure or perfusion.
HR may drop or become weak
RR becomes irregular/slow
BP ↓
Why compensation shock fails
Body runs out of oxygen + energy
Late signs of shock
Hypotension
Altered LOC
Cyanosis
Weak/slow pulse
Why skin is pale/cool in shock
Vasoconstriction shunts blood to core
Why nausea occurs in shock
Blood diverted from GI system
Narrowing pulse pressure meaning
Vasoconstriction → worsening shock
Pediatric shock difference
for kids:
BP stays NORMAL until VERY late
tachycardia
pale skin
delayed cap refill
tachypnea
Best early indicator of shock
Vital sign trends (HR ↑, RR ↑)
Tachycardia (increased heart rate)
Arterial bleeding
Bright red, spurting, severe
Venous bleeding
Dark red, steady
Capillary bleeding
Slow ooze
Massive hemorrhage definition
Rapid, life-threatening blood loss
Junctional bleeding locations
Neck, armpit (axilla), groin
Why junctional bleeding is dangerous
Involves major vessels and cannot be easily controlled with a tourniquet
Bleeding control order
Direct pressure
Wound packing
Hemostatic agents
Tourniquet
How direct pressure works
Compresses vessels → allows clotting
Key rule with dressings
DON’T remove once applied
When to use wound packing
Deep wounds/junctional areas
Key technique for wound packing
Pack until FULL → then apply pressure
What hemostatic agents do
Speed up clotting
STILL need direct pressure
When to use tourniquet
Severe extremity bleeding not controlled
Improvised tourniquet rule
Must be wide (≥2 inches), never rope/wire
Elevation purpose
↓ blood pressure in limb
Cold application purpose
Vasoconstriction + ↓ bleeding
Head injury bleeding what u dont do vs what u do
DO NOT stop fluid from ears/nose
DO:
Let fluid drain freely
Place a loose sterile dressing to catch it
DO NOT apply pressure
Nosebleed treatment
Lean forward + pinch nostrils
5 core treatments for shock
Rapid transport
Oxygen
Control bleeding
Keep warm
Supine
Signs of internal bleeding
Bruising
Tender abdomen
Vomiting blood
Blood in stool
Shock signs
Best clue for internal bleeding
Mechanism of injury
What are soft tissues?
Skin, fat, muscles, vessels, nerves, connective tissue, glands
3 layers of skin
Epidermis → outer, no blood vessels → less bleeding
Dermis → blood vessels + nerves → pain + bleeding
Subcutaneous → fat layer → insulation + shock absorption
Epidermis characteristics
No blood vessels or nerves → superficial injuries less severe
Why is dermis injury serious?
Dermis has blood vessels + nerves → bleeding + pain + infection risk
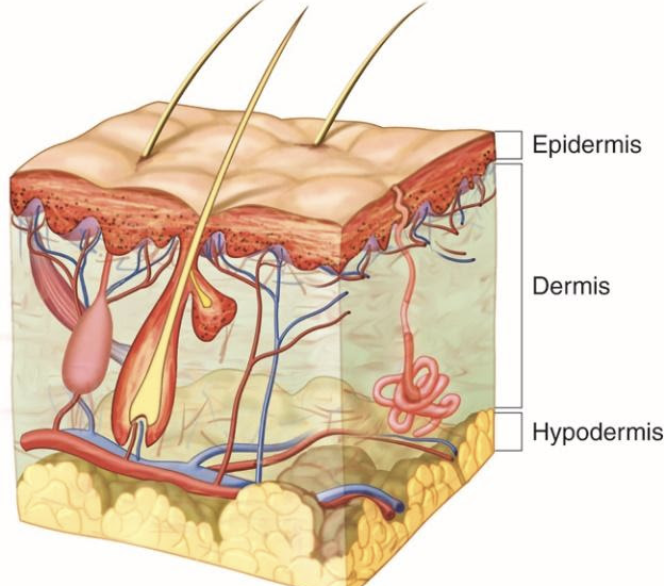
Subcutaneous layer function
Insulation + shock absorption
Closed wound definition
Skin intact, internal damage
Types of closed wounds
Contusion, hematoma, crush injury, blast injury
Contusion
A closed soft-tissue injury where the skin is intact but underlying blood vessels are damaged, causing bleeding into the tissues
Assess ABCs
Treat for possible internal injury/shock if MOI is significant
Cold pack (not directly on skin)
Monitor

Why swelling happens
Blood + inflammation
Hematoma
A localized collection of blood under the skin or in tissue from a damaged blood vessel (usually a closed injury).
ABCs, assess MOI
Consider internal injury/shock if large or high-risk location
Cold pack (not directly on skin)
Splint if associated with extremity injury
Monitor

Key difference contusion vs hematoma
Contusion = small vessel bleeding (flat bruise)
Hematoma = larger vessel bleeding (raised blood collection)ore severe bleeding
Crush injury
Injury caused by strong compressive force that damages internal tissues/organs (with or without breaking the skin).
Why crush injuries are dangerous
Internal bleeding + organ rupture
Closed wound care priorities
ABCs
Treat for shock
Splint
Cold packs
Rapid transport
Open wound definition
Skin broken → infection risk
Abrasion
A superficial open wound where the top layer of skin is scraped off
Scrape (high infection risk, painful)
Laceration
A cut or tear in the skin caused by a sharp or blunt object (can damage vessels/tendons)
Puncture wound
Deep penetration → small outside, severe inside
Why punctures are dangerous
Internal bleeding + infection + hidden damage
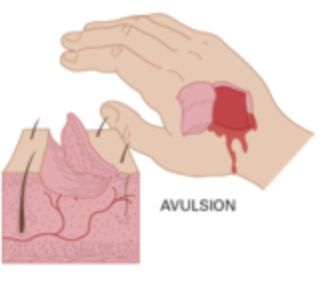
Avulsion
A wound where skin or tissue is torn away (partially or completely)
Rule for impaled objects
DO NOT remove
When can you remove impaled object in cheek?
If it passes through AND both ends visible
Steps for open wound care
Expose
Control bleeding
Prevent contamination
Dress + bandage
Treat shock
Always check PMS (pulse, motor, sensation) distal to injury
Biggest mistake with wounds
Focusing on gross wound → missing ABCs
Dressing
Covers wound (sterile)
Bandage
Holds dressing in place
Pressure dressing
Tight bandage to control bleeding
Occlusive dressing
A dressing that creates an airtight seal over a wound (chest, neck, abdomen)
Universal dressing
Large bulky dressing
3 ways to classify burns
Agent/source
Depth
Severity
Burn agents
Thermal, chemical, electrical, radiation, light
Superficial burn
Epidermis only → red, painful, no blisters
Partial thickness burn
Epidermis + dermis → blisters, very painful
Full thickness burn
All layers → charred/white, NO pain (nerve damage)
High-risk burn locations
Face, hands, feet, genitalia, joints
Why circumferential burns dangerous
(Burns that go all the way around a body part (arm, leg, chest, etc.))
Restrict circulation/breathing
Rule of nines
Body divided into 9% sections (adult)
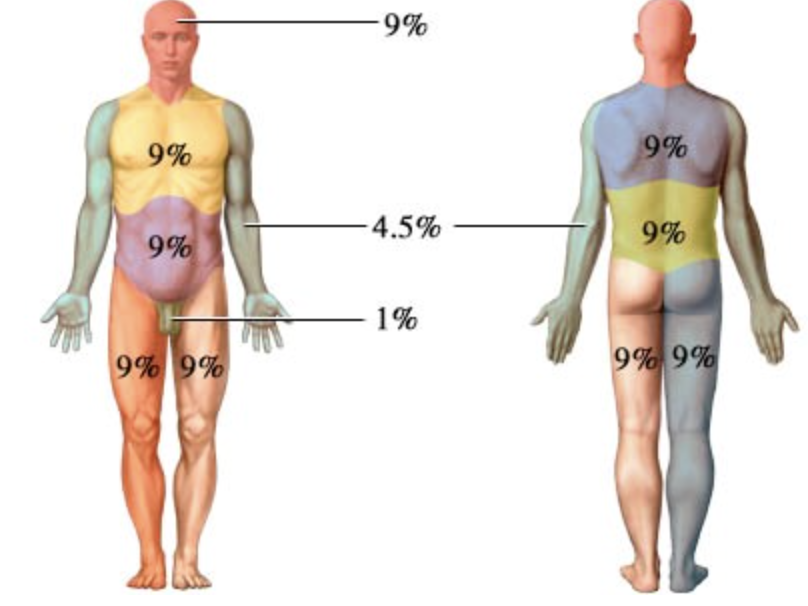
Rule of palm
Patient palm = 1% body surface
Burns requiring burn center
10% partial thickness
ANY full thickness
Face/hands/feet/genitals
Electrical
Inhalation
First step thermal burn
Stop burning process
What NOT to do for burns
No ice
No ointments
Don’t pop blisters
Key treatment for burns
Dry sterile dressing
Oxygen
Treat shock
Signs of airway burn
Hoarse voice
Soot
Burned hair
Stridor
Why airway burns dangerous
Swelling → delayed airway closure
Main treatment for chemical burns
Flush with water (≥20 min)
Do NOT use neutralizers (like vinegar/baking soda)
Exception chemical burns (dry chemicals)
Brush off first, THEN flush
Why alkali burns worse
Alkalis penetrate deeper and keep destroying tissue
Why electrical injuries dangerous
Small outside, massive internal damage
Electrical injury signs
Entry/exit wounds
Arrhythmias
paralysis
fractures