Module 6 (Reproductive system)
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
Pregnancy
The period from fertilization until the infant is born.
Conceptus
Everything that develops from the fertilised egg inside the uterus.
Gestation Period
The time from the last menstrual period (LMP) until birth, approximately 280 days (40 weeks).
Embryo
The conceptus from fertilisation until the end of week 8.
Fetus
The conceptus from week 9 until birth.
Gamete
A reproductive cell; sperm in males and oocyte (egg) in females.
Fertilisation (Conception)
The union of a sperm and an oocyte, resulting in a zygote.
Zygote
The single cell formed immediately after fertilisation.
Cleavage
A series of rapid cell divisions that occur after fertilisation as the zygote travels to the uterus.
Blastomeres
The cells produced during cleavage.
Morula
A solid ball of blastomeres formed about 72 hours after fertilisation.
Blastocyst
A hollow structure formed from the morula (100 cells) around days 4–5 that contains an inner cell mass and trophoblast.
It is here where the zona Pellucida breaks down with the blastocyst escaping from it
Inner Cell Mass
The group of cells within the blastocyst that develops into the baby and other tissues.
Trophoblast
The outer layer of the blastocyst that develops into the placenta.
Implantation
Beginning around day 7 after fertilisation where the blastocyst attaches to the endometrium of the uterus
Bilaminar Embryo
The two-layer embryo formed during week 2, consisting of the epiblast and hypoblast from the inner mass.
Epiblast
One layer of the bilaminar embryo that gives rise to all three germ layers (baby’s body).
Hypoblast
The second layer of the bilaminar embryo that contributes to yolk sac (placenta stand in - transfer nutrients and waste removal)
Gastrulation
The process during week 3 that converts the bilaminar embryo (epiblast) into a trilaminar embryo.
Trilaminar Embryo
The three-layer embryo formed after gastrulation.
Ectoderm
Outer germ layer; forms the nervous system and epidermis.
Mesoderm
Middle germ layer; forms muscles, bones, connective tissue, blood, and many organs.
Endoderm
Inner germ layer; forms the lining of the digestive and respiratory systems.
Placenta
A temporary organ formed largely from trophoblast tissue that supports fetal growth and exchange of nutrients and wastes.
Summary of that in sequence
Fertilisation → Zygote (contains zone pellucida, the Corona radiata shedded once the sperm came in contact) → Cleavage → Blastomeres → Morula → Blastocyst (escapes from the zona pellcida) → Implantation → Bilaminar Embryo (epiblast and hypoblast) → Gastrulation → Trilaminar Embryo (ectoderm, mesoderm, endoderm) → Embryo → Fetus.
What conditions are necessary for fertilisation to occur
Sperm must reach the ovulated oocyte.
Oocyte remains viable for ~24 hours.
Sperm remain viable for ~48 hours after ejaculation.
Intercourse must occur within 2 days before or 24 hours after ovulation.
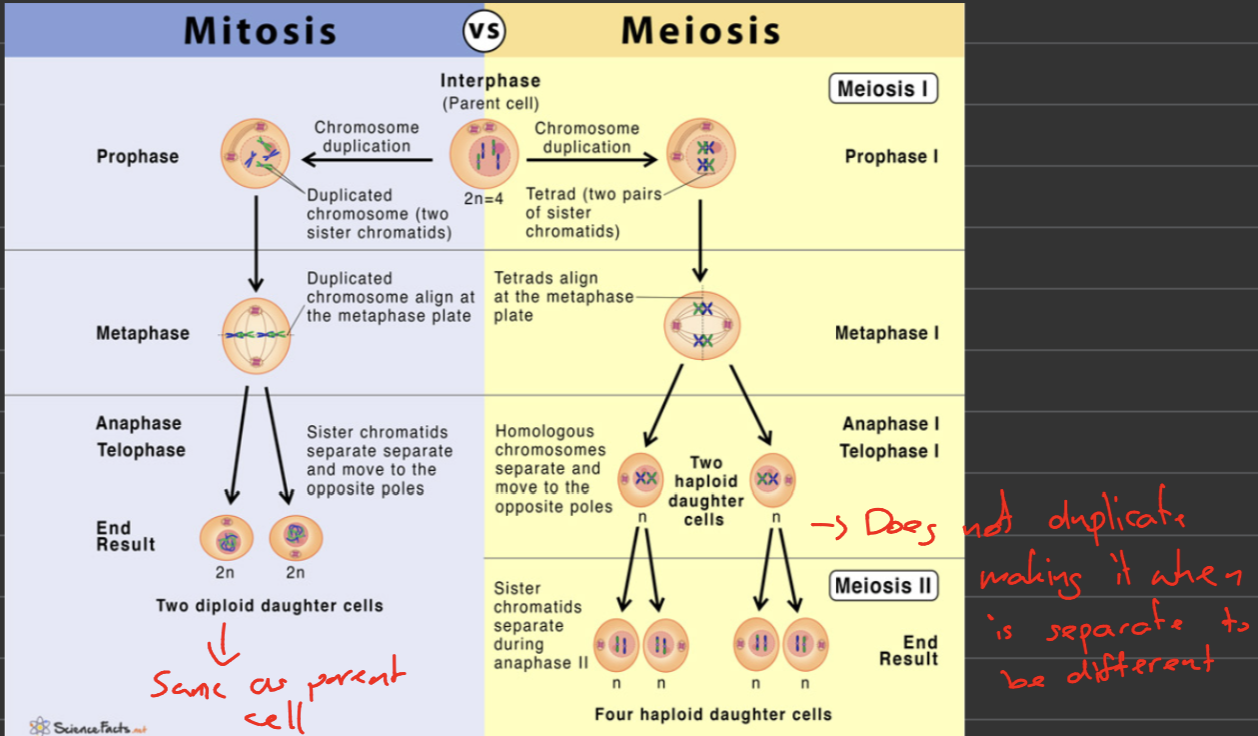
Mitosis vs Meiosis
Mitosis | Meiosis |
|---|---|
One cell division | Two cell divisions |
Produces 2 daughter cells | Produces 4 daughter cells |
Chromosome number maintained (diploid) | Chromosome number halved (haploid) |
Genetically identical cells | Genetically diverse cells |
Used for growth and repair | Used for gamete production |
Haploid and Diploid Cells
Diploid (2n): 46 chromosomes (23 pairs); found in most body cells.
Haploid (n): 23 chromosomes; found in each sperm and oocyte.
Chromosomal Composition
Humans have 46 chromosomes.
23 inherited from the mother.
23 inherited from the father.
Chromosome pair 23 determines biological sex.
XX = female, XY = male.
What are the three stages of spermatogenesis?
Mitotic proliferation (16–20 days)
Spermatogonia divide by mitosis (diploid).
Produces large numbers of cells.
Meiotic division (20–24 days)
Produces haploid cells via meiosis.
Creates genetic diversity.
Cytodifferentiation (~24 days)
Spermatids differentiate into sperm.
Chromosomes become tightly packaged (into a head and tail, effective for fertilization).
Total process ≈ 70–80 (on top of the ~10 days to mature) and occurs continuously throughout life.
Sperm Anatomy
Head
Nucleus (23 chromosomes)
Acrosome (enzymes for fertilization, allowing it to penetrate the egg)
Midpiece
Packed with mitochondria
Produces ATP for tail movement
Tail
Enables the cell to move
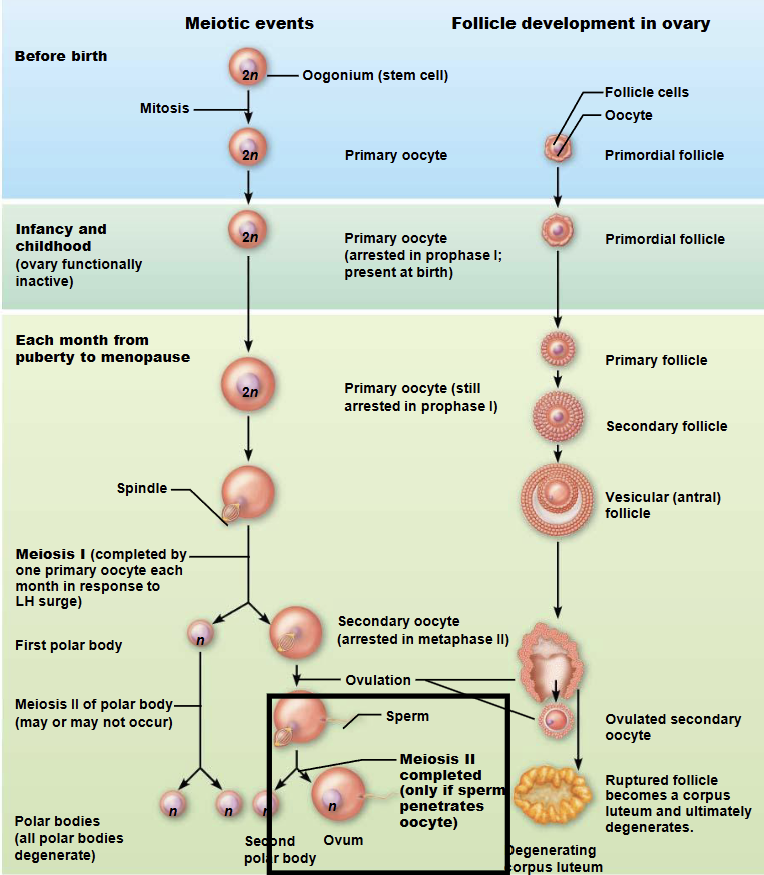
Describe oogenesis, including when the different stages occur during life.
Before Birth
Oogonia divide rapidly by mitosis during fetal life.
Of the many oogonia produced, only some develop into primary oocytes + follicle.
Primary oocytes begin meiosis I and then arrest in prophase I.
Females are born with all the primary oocytes they will ever have.
Puberty to Menopause
During each menstrual cycle, a small number of primary oocytes and their follicles become active.
Usually only one dominant primary oocyte + follicle is selected.
The dominant primary oocyte resumes and completes meiosis I.
This produces a secondary oocyte + follicle and the first polar body.
The secondary oocyte + follicle immediately begins meiosis II and arrests in metaphase II.
Ovulation
The mature follicle (Corona radiata) ruptures and releases the secondary oocyte from the ovary.
This release is called ovulation.
If Fertilization Occurs
Entry of a sperm triggers completion of meiosis II.
The secondary oocyte forms a mature ovum and a second polar body.
The male and female pronuclei then fuse to form a diploid zygote.
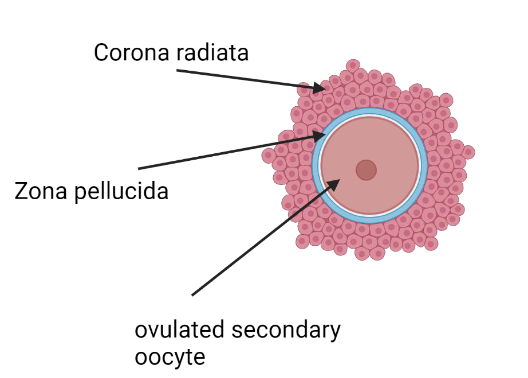
Ovulated Secondary Oocyte Anatomy
From inside to outside:
Secondary oocyte
Zona pellucida (follicle develops, forming into a thick protective barrier around the oocyte)
Corona radiata (carries the left over follicular cells protecting/nourishing the oocyte)
These layers must be penetrated by sperm for fertilization.
What is capacitation?
Capacitation is the process that sperm undergo within the female reproductive tract to be capable of penetrating/fertilizing the oocyte.
Effects:
Increases sperm’s ability to move.
Makes sperm capable of undergoing the acrosome reaction.
Enables fertilization.
What is the acrosome reaction?
Approach – Sperm moves through the corona radiata, using enzymes to separate the cells.
Acrosomal Reaction – Sperm binds to the zona pellucida and releases enzymes that help digest a pathway.
Multiple sperm releases its enzymes not to become fertile but to clear a path
Binding – One sperm reaches and binds to the oocyte membrane.
Fusion – Sperm and oocyte membranes fuse, allowing the sperm nucleus to enter the oocyte.
Tail and mitochondria left out
What prevents polyspermy?
Polyspermy = fertilization by more than one sperm.
The oocyte prevents this by:
Oocyte membrane block (fast block).
First sperm enters.
Oocyte membrane depolarizes.
Temporarily blocks other sperm.
Cortical reaction (slow block).
Calcium rises in the oocyte as the first sperm enters.
Cortical granules release enzymes.
Zona pellucida hardens and loses sperm-binding sites.
Prevents additional sperm from entering.
Explain the processes involved in fertilisation.
1. Sperm reaches the oocyte
Sperm travels through the female reproductive tract to the ampulla of the uterine tube.
Sperm must first undergo capacitation to become capable of fertilization.
2. Penetration of the oocyte
Sperm passes through the corona radiata.
Binding to the zona pellucida triggers the acrosomal reaction.
Acrosomal enzymes digest a pathway through the zona pellucida.
One sperm reaches and binds to the oocyte membrane.
3. Fusion
Sperm and oocyte membranes fuse.
The sperm nucleus enters the oocyte.
4. Block to polyspermy
Oocyte membrane block
Cortical reaction
Preventing additional sperm from entering.
5. Completion of meiosis II
The secondary oocyte completes meiosis II.
A mature ovum and second polar body are produced.
6. Formation of the zygote
Male and female pronuclei fuse.
Chromosome number is restored to 46 (diploid).
A zygote is formed, marking successful fertilization.
What are the major causes of infertility?
Male Factors
Low sperm count
Poor sperm motility
Abnormal sperm morphology
Erectile dysfunction
Blocked reproductive ducts
Female Factors
Failure to ovulate
Blocked uterine tubes
Endometriosis
Hormonal disorders
Reduced ovarian reserve with age
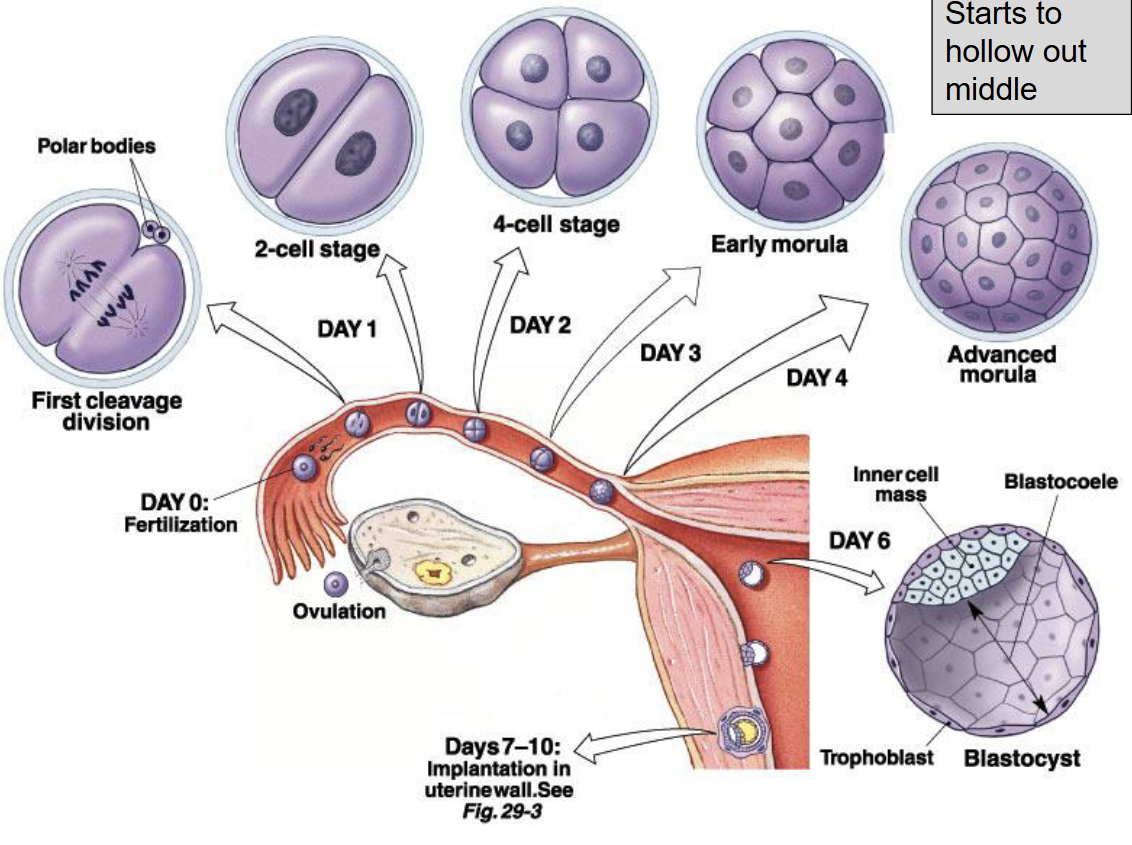
What are the key events of Week 1 after fertilisation?
Cleavage
The fertilised egg is called a zygote.
The zygote is surrounded by the zona pellucida.
The zygote travels through the uterine tube while undergoing repeated mitotic divisions called cleavage event.
Each new cleaved cell is called a blastomere.
Morula
By day 3, the embryo forms a solid ball of blastomeres called the morula.
Blastocyst
By day 4–5, about 100 cells are present.
A fluid-filled cavity forms, creating the blastocyst.
Hatching
The zona pellucida breaks down with the blastocyst hatching, so it can implant.
Implantation Begins
Around day 7, trophoblast cells attach to the endometrium.
Sequence:
Zygote → Cleavage → Blastomeres → Morula → Blastocyst → Hatching → Implantation
What are the main cell types of the blastocyst and what do they become?
Trophoblast (Outer Layer)
Forms the placenta.
Begins implantation into the endometrium.
Inner Cell Mass (20–30 cells)
Forms the embryo (baby).
During Implantation the Trophoblast Splits Into:
Cytotrophoblast
Inner trophoblast layer.
Produces new trophoblast cells.
Syncytiotrophoblast
Outer trophoblast layer.
Invades the endometrium.
Helps establish the placenta.
Memory Tip:
Inner Cell Mass = Baby
Trophoblast = Placenta
What is implantation?
Begins around day 7 after fertilisation.
The blastocyst attaches to the endometrium.
Trophoblast cells stick to the uterine lining and initiate implantation.
The blastocyst triggers an inflammatory response in the endometrium.
This causes breakdown of endometrial tissue, allowing trophoblast cells to invade.
During implantation, trophoblast cells differentiate into:
Cytotrophoblast
Syncytiotrophoblast
Implantation is usually complete by day 12.
Bilaminar embryo formation (Week 2)
The inner cell mass differentiates into two layers:
Epiblast (upper layer)
Hypoblast (lower layer)
These two layers form the bilaminar (two-layered) embryonic disc.
Trilaminar embryo formation (Week 3)
The bilaminar embryonic disc undergoes gastrulation, forming the trilaminar (three-layered) embryo:
Ectoderm ("outer skin")
Forms the nervous system and epidermis (skin).
Mesoderm ("middle skin")
Forms muscles, bones, connective tissue, blood vessels, and most other body tissues.
Endoderm ("inner skin")
Forms the epithelial lining of the digestive, respiratory, and urogenital systems, as well as their associated glands.
Compare the embryonic and fetal periods, and explain why problems during the fetal period are important.
Embryonic Period (Fertilisation–Week 8)
Major organs form.
Most vulnerable period for birth defects and miscarriage.
Fetal Period (Week 9–Birth)
Growth and maturation of organs.
Organs become functional.
Problems during the fetal period:
Poor placental function.
Growth restriction.
Preterm birth.
Reduced oxygen or nutrient supply.
These problems may not be immediately fatal but can increase the risk of heart disease, diabetes, high blood pressure, and other health problems later in life.
Why is preterm birth harmful?
Preterm birth = birth before 37 weeks.
Risks:
Immature lungs
Brain injury
Feeding difficulties
Increased illness and mortality
The earlier the birth, the greater the risk.
Why is fetal growth restriction harmful?
Can cause:
Low birth weight
Organ dysfunction
Developmental delays
Increased risk of adult disease
Often caused by placental dysfunction.
What are the functions of the placenta?
Delivers oxygen, nutrients to the fetus.
Removes carbon dioxide and waste products.
Produces hormones that maintain pregnancy.
Protects the fetus from some harmful substances.
How do DNA and hormones determine biological sex?
Biological sex is determined by:
Genotype (XX or XY)
Hormone production
The SRY gene on the Y chromosome triggers testis development.
Testes produce testosterone, which drives male reproductive development.
In the absence of significant testosterone, female reproductive structures develop.
What structures are found in the spermatic cord?
Contains blood vessels, nerves, ductus deferens
Blood vessels
Testicular artery
Pampinaform plexus (Testicular vein)
Nerves
Testicular nerve
Ductus deferens
Transports sperm to ejaculatory duct
What is the inguinal canal?
Passage connecting the abdomen to the scrotum.
Testes develop in the abdomen, before traveling down the deep inguinal ring (entrance)
It then exits from the inguinal canal through the superficial inguinal ring (exit)
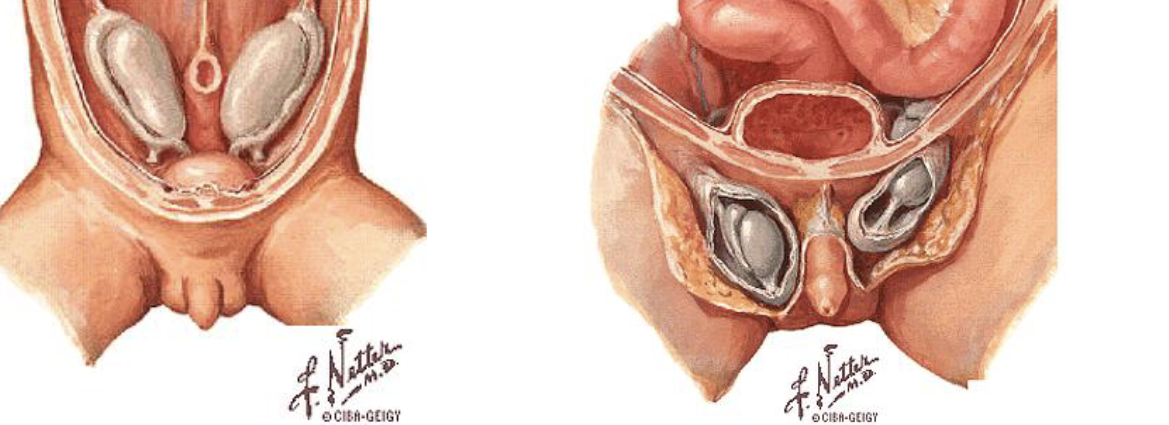
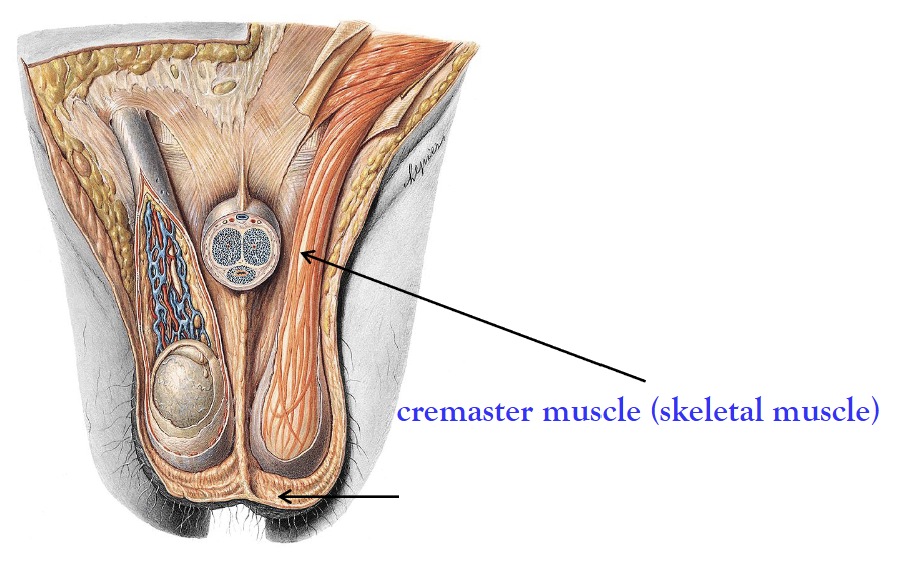
Describe the anatomy of the scrotum.
The scrotal septum divides the scrotum into two compartments.
Contains one testes each.
Wall consists of:
Skin (external)
Superficial fascia
Dartos muscle (smooth muscle)
Cremaster muscle (skeletal muscle) surrounds the testes and forms on the spermatic cord.
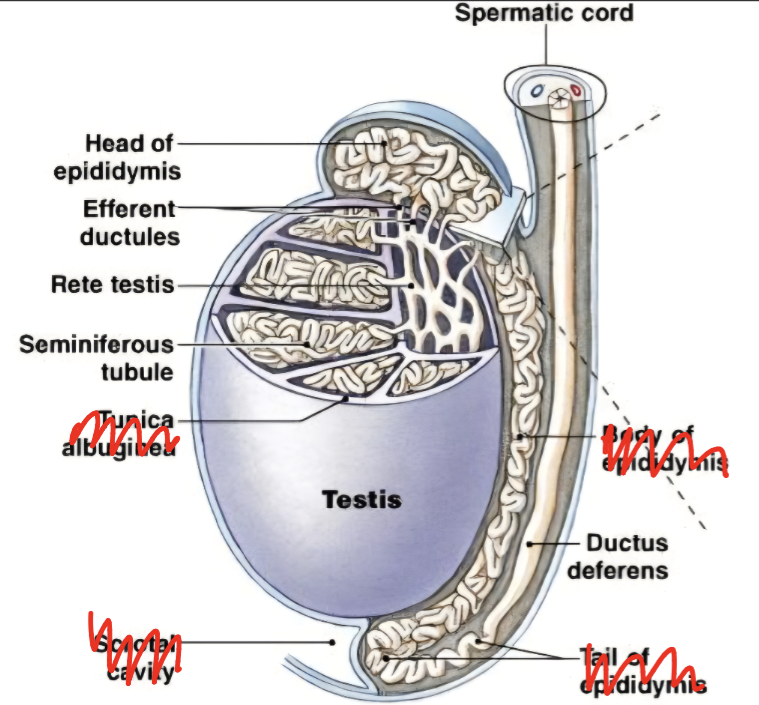
Describe the anatomy of the testes.
Paired male gonads located within the scrotum.
Divided into lobules and suspended in the scrotum by the spermatic cord.
Testes contain 2 main cells:
Sertoli cells (produce sperm)
Leydig cells (produce testosterone - required for sperm production)
Seminiferous tubules (produce sperm) → Straight tubules (channel sperm) → Rete testis (collects sperm) → Efferent ducts (transport sperm) → Epididymis (stores and matures sperm).
What are common disorders of the scrotum and inguinal canal?
Epididymitis - inflammation of epididymis
Varicocele – enlarged testicular veins
Cryptorchidism – one or both testes fail to descend or later retracts
Testicular torsion – twisting of the spermatic cord
Inguinal hernia – abdominal contents protrude through the inguinal canal
Where are sperm produced and what is their travel pathway?
Produced in:
Seminiferous tubules of the testes.
Supported by Sertoli cells and stimulated by testosterone.
Pathway:
Seminiferous tubules → Epididymis → Ductus deferens → Ejaculatory duct → Urethra → Penis
Key functions along the pathway:
Epididymis: sperm mature and gain motility.
Ductus deferens: transports sperm during ejaculation.
Ejaculatory duct: mixes sperm with seminal fluid.
Urethra: carries semen out of the body.
Memory Tip:
"Made, Matured, Moved, Mixed, Exit"
(Testes → Epididymis → Ductus deferens → Ejaculatory duct → Urethra)
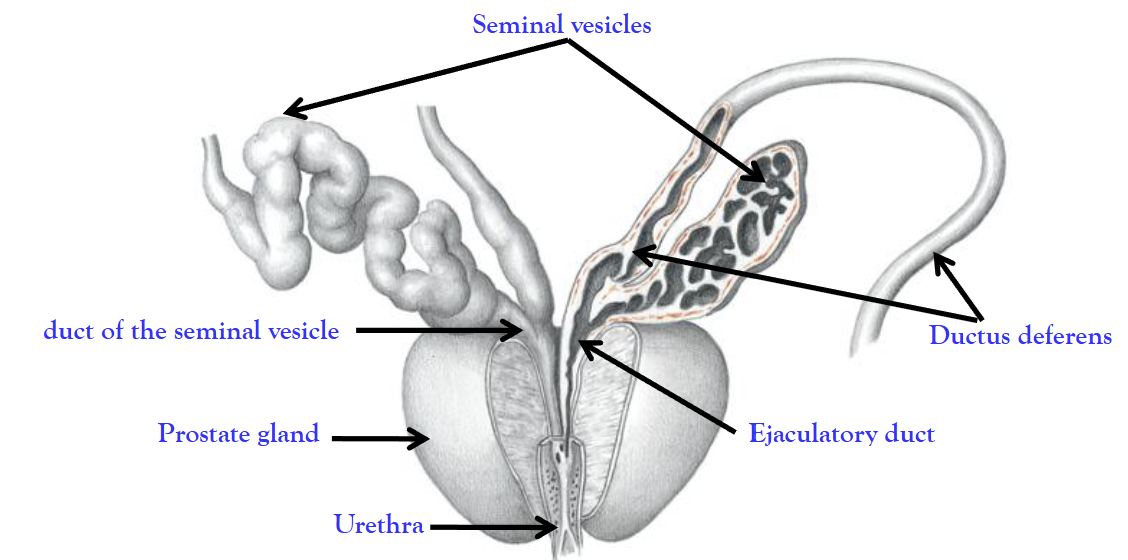
Describe the anatomy and physiology of the ejaculatory ducts and accessory glands.
Ejaculatory ducts
Formed by the ductus deferens + seminal vesicle duct.
Transport sperm and seminal fluid into the urethra during ejaculation.
Accessory glands
Seminal vesicles (on both ejaculatory ducts) → produce ~70% of total volume of semen.
Prostate gland (only one)→ adds slightly alkaline semen fluid (25%), to neutralizes the
acidity of the vagina.Bulbourethral glands (on both ejaculatory ducts) → secrete lubricating mucus.
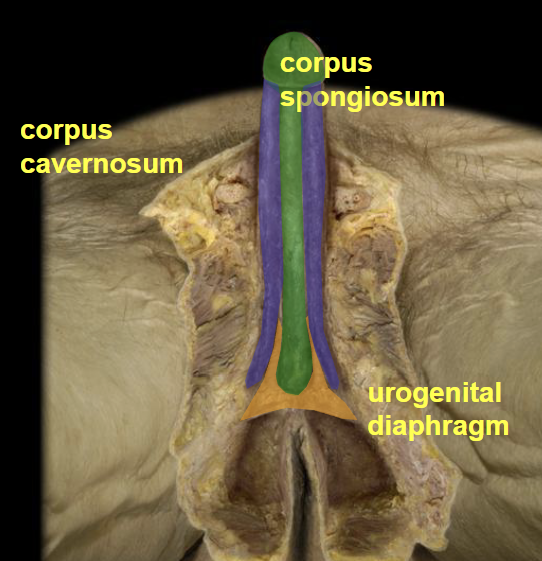
What are the main anatomical parts and erectile tissues of the penis?
Crura – proximal ends of the corpora cavernosa that anchor the penis to the pubic arch.
Body (shaft) – main part of the penis.
Glans penis – sensitive tip of the penis.
Prepuce (foreskin) – skin covering the glans, attached by the frenulum.
Corpus cavernosum (paired)
Main erectile tissue.
Contains deep arteries.
Engorges with blood during erection.
Corpus spongiosum (single)
Surrounds the urethra.
Keeps the urethra open during erection.
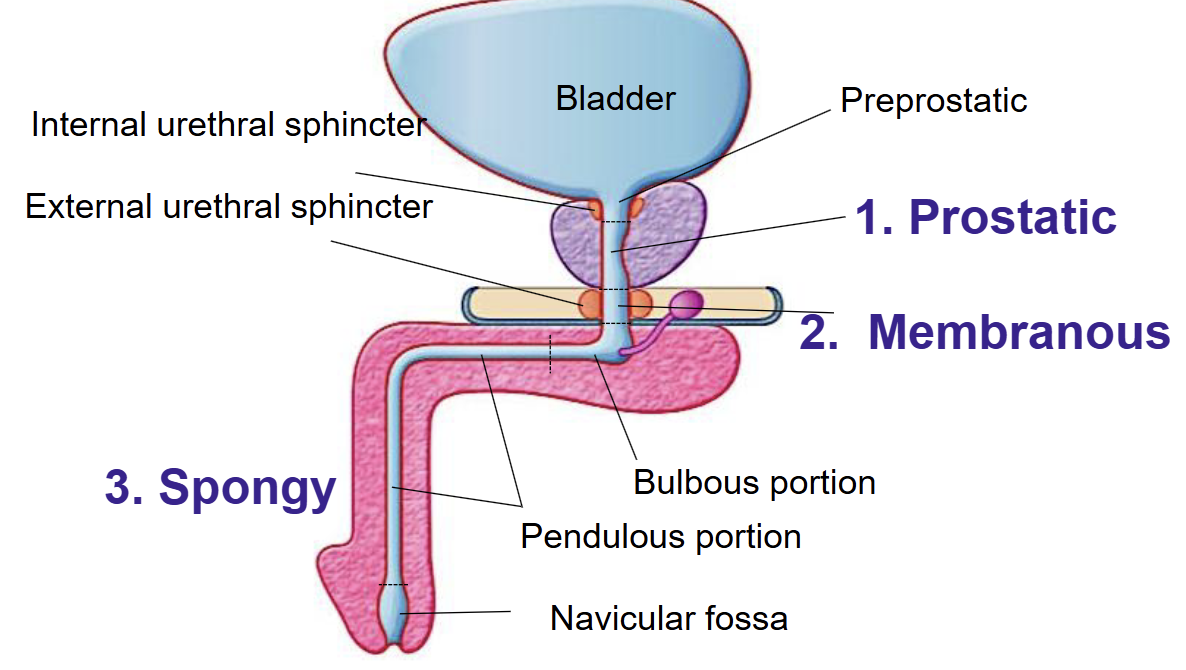
Describe the male urethra and erectile dysfunction (ED).
Male urethra:
Prostatic → Passes through the prostate gland
Membranous → Goes through the pelvic floor muscles
Spongy (penile) → Runs through the penis
Internal urethral sphincter
Prevents semen from flowing back into the bladder during ejaculation.
Erectile Dysfunction (ED):
Inability to achieve or maintain an erection.
Can be:
Psychogenic (stress, lack of arousal)
Organic (vascular, nerve, or hormonal problems)
What is the anatomy and function of the ovary?
Paired oval glands; site of oocyte development and female hormone production.
Has an outer cortex (contains follicles) and
Inner medulla (contains blood vessels).
Each cycle, a follicle matures and releases a secondary oocyte.
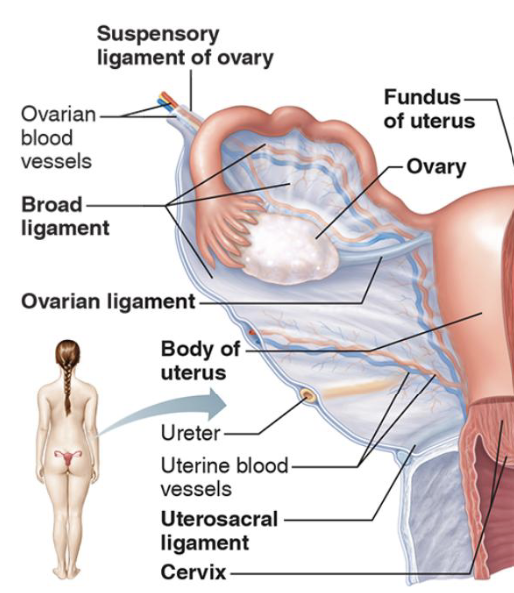
How are the ovaries attached within the pelvis?
The ovary is attached by:
Broad ligament → connects and holds the fallopian tubes, uterus, and ovaries (structural support).
Ovarian ligament → connects ovary to the uterus (help keep it in position).
Suspensory ligament → connects the ovary to the pelvic wall (contains blood vessels and nerves).
These ligaments help position the ovary during ovulation.
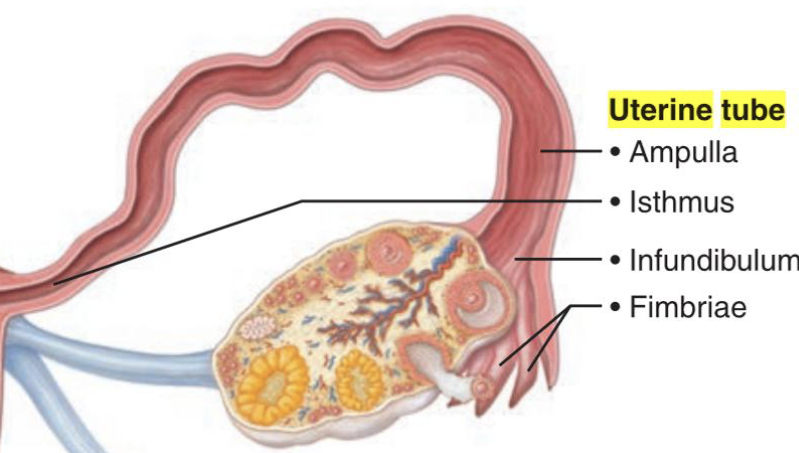
What are the parts and functions of the Fallopian tubes?
Fimbriae – finger-like projections collecting the ovulated oocyte from the pelvic cavity.
Infundibulum – funnel-shaped entrance.
Ampulla – widest section as well as the usual site of fertilisation.
Isthmus – transports embryo to uterus, narrow section.
How is the oocyte transported and what is an ectopic pregnancy?
Fimbriae catch the ovulated egg and move into the fallopian tube
Cilia and smooth muscle contractions move the oocyte through the uterine tube.
Fertilisation usually occurs in the ampulla.
Continues to travel through the isthmus and finally into the uterus
Ectopic pregnancy occurs when implantation happens outside the uterus, where it can get stuck in the fallopian tube
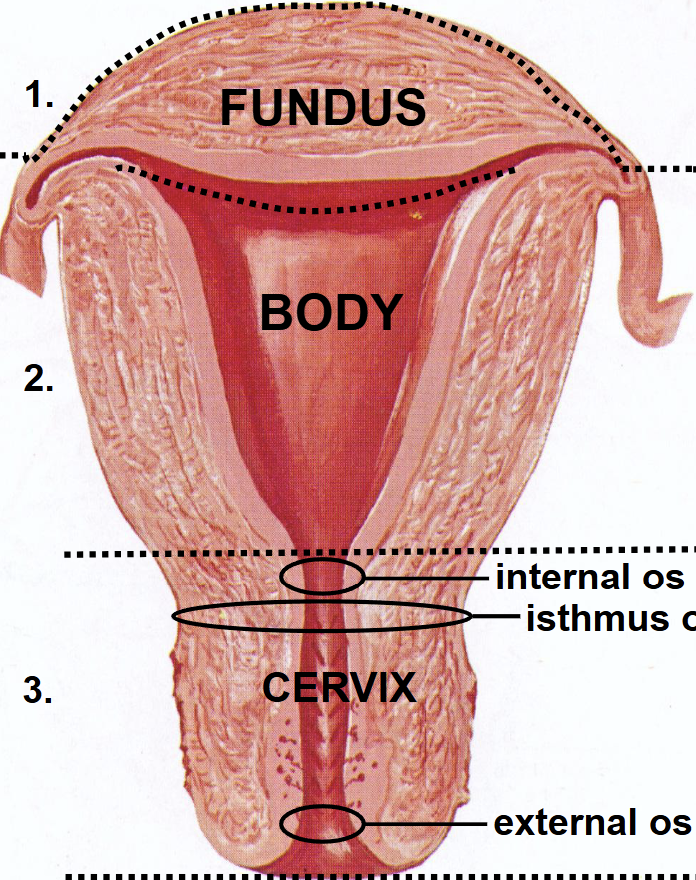
What are the regions of the uterus?
Fundus – upper portion.
Body – middle region where the fetus develops.
Cervix – lower portion projecting into the vagina.
Function: The uterus, hosts, nourishes, and protect a developing fetus, and to contract rhythmically during labor to expel the baby.
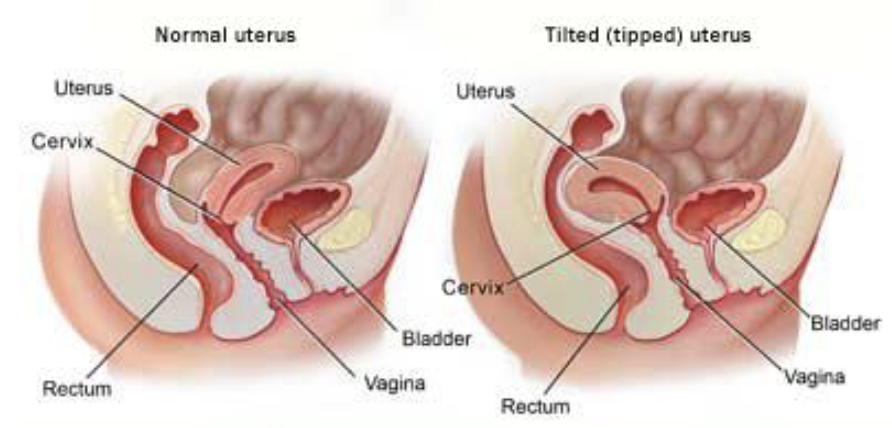
What is the normal position of the uterus?
Usually anteverted (tilted forward towards the bladder).
About 25% of women have a retroverted uterus (tilted backwards).
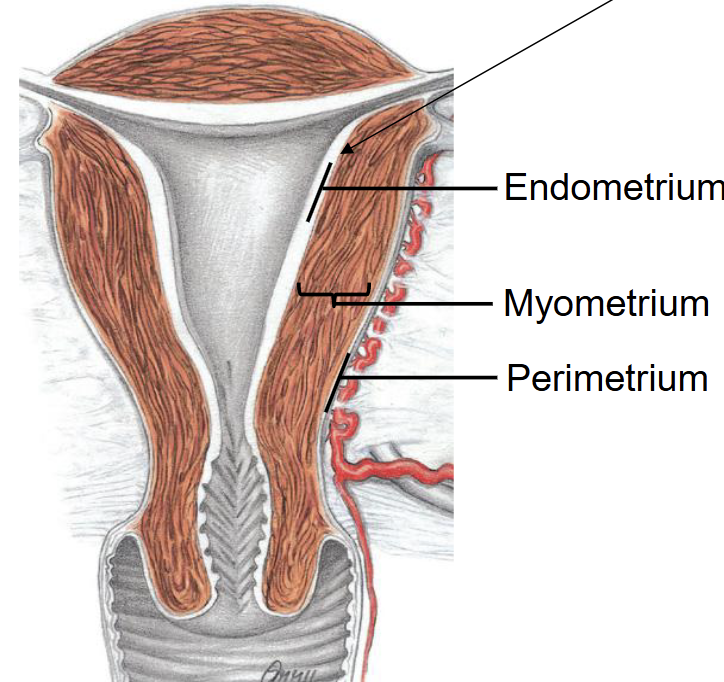
What are the layers of the uterine wall?
Endometrium – inner layer; shed during menstruation.
Myometrium – thick smooth muscle layer.
Perimetrium – outer thin layer.
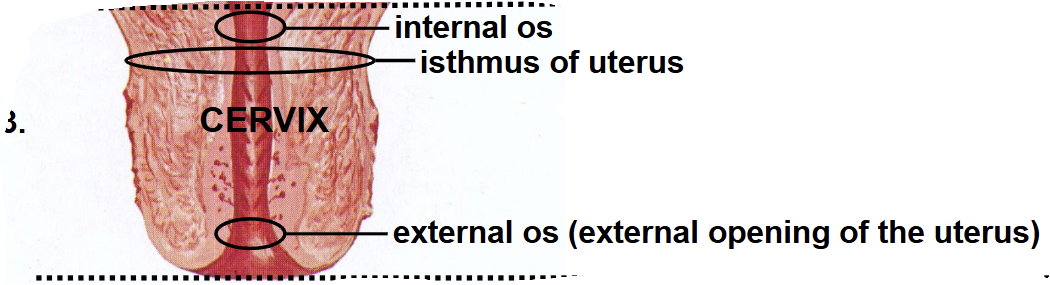
What is the cervix?
Lower one-third of the uterus.
Forms the passage between the uterus and vagina.
Contains the internal and external os.
It is the narrowest part of the cervix
Different invasive disorders or conditions with implantation over the cervix.
Placenta previa
Placenta implants low in the uterus.
Partially or completely covers the cervix.
Can cause serious bleeding during pregnancy and birth.
Placental accreta, increta and percreta
Conditions where the placenta grows too deeply into the uterus, with increasing severity from accreta to percreta.
What are the anatomy and functions of the vagina and its relationship to the cervix?
Muscular/elastic canal connecting the cervix to the exterior.
Receives penis during intercourse.
Passage for menstrual flow.
Birth canal during delivery.
Holds the sperm before passing into the uterus
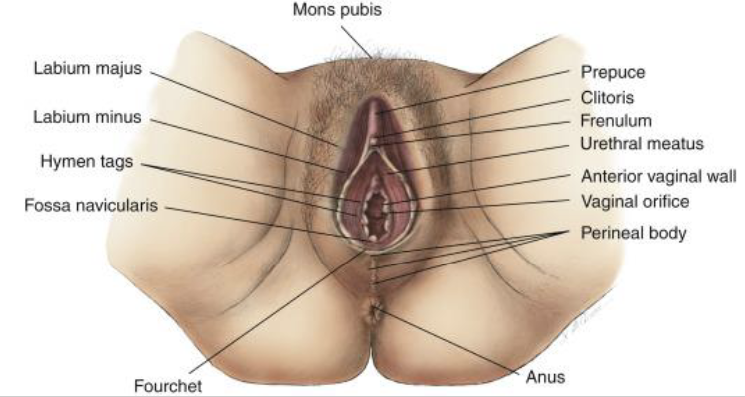
What structures form the vulva?
Mons pubis → provides protection from the pelvis
Labia majora → paired and thickened folds of skin
Labia minora → sits inside the majora, it also paired
Clitoris → small erectile body
Vestibule → space created by the minora
What are the accessory glands of the female reproductive system?
Greater vestibular (Bartholin's) glands.
Lesser vestibular (Skene's) glands.
Function: Produce mucus for lubrication.
What is the main erectile tissue in females?
Clitoris
Contains erectile tissue that becomes engorged during sexual arousal.
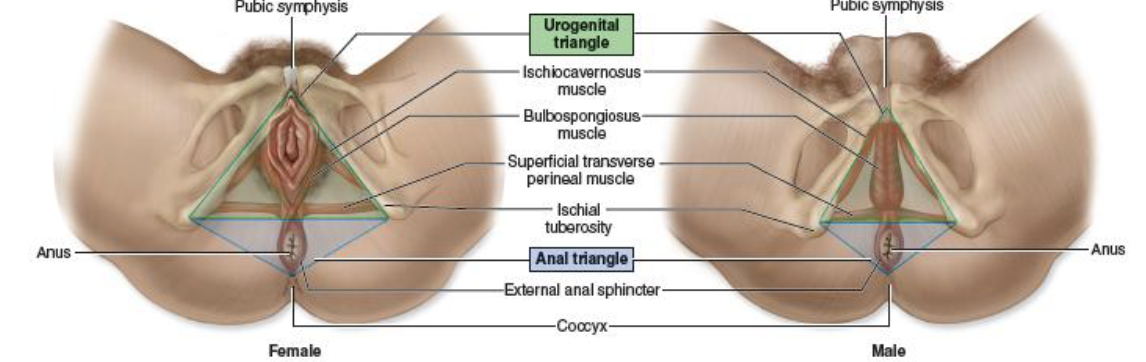
What is the perineum?
Area between the external genitalia and anus.
Contains muscles that support the pelvic organs.
What is the function of the mammary gland?
Produces and secretes milk after birth.
Contains lobes and lactiferous ducts that transport milk to the nipple.
Prolactin stimulates production of breast milk
Oxytocin is responsible for milk ejection
What is the composition of semen?
10% sperm - from the testies
70% seminal vesicle fluid
20% prostatic, bulbourethral fluids from respective glands
Summaries the male sexual response.
Erection → Emission → Ejaculation
Erection: sexual stimulation activated neural pathways, promoting nitric oxide (NO) to vasodilate and fill erectile tissue with blood.
Emission: Sperm from the epididymis → ductus deferens → gland secretions, moving into the urethra, with the urethral sphincter preventing backflow.
Ejaculation: Rhythmic muscle contractions to expel semen.
Name and explain the two female sex hormones
Estrogen
Promotes significant development of female reproductive organs.
breasts, thickening of uterine lining (endometrium)
Progesterone
Maintains the endometrium for implantation.
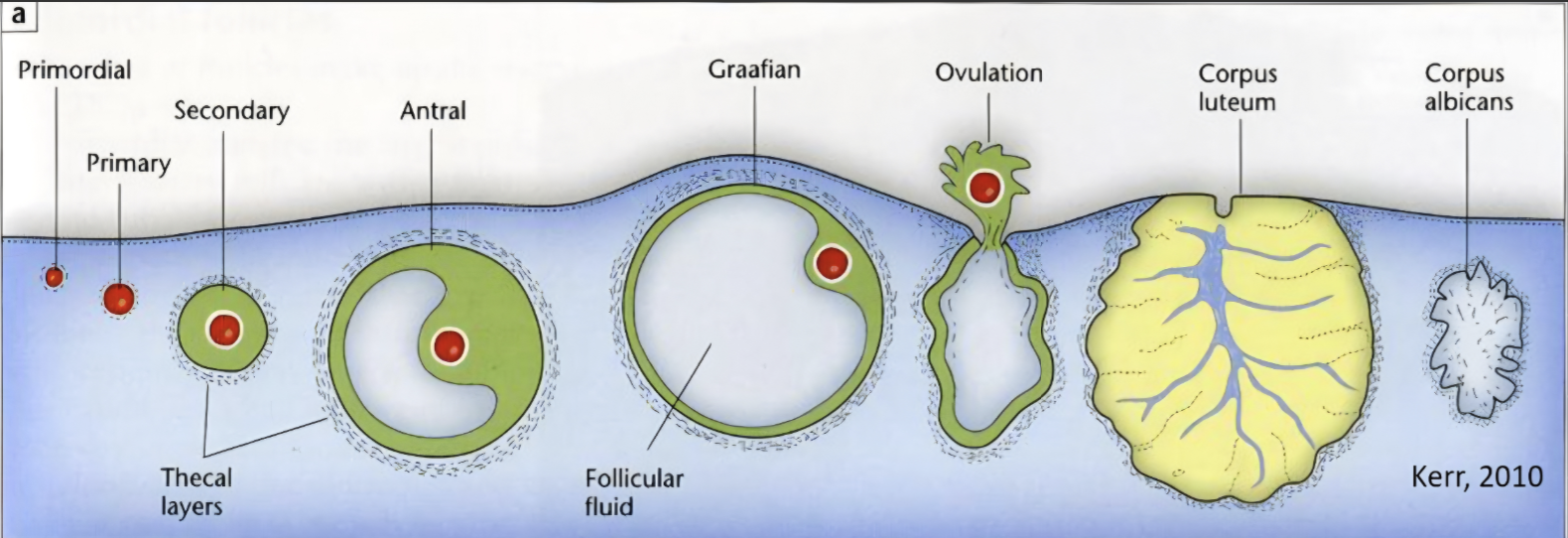
Describe the ovarian cycle.
1. Follicular Phase (Days 1–14)
Several follicles begin developing.
One dominant follicle is selected.
Follicle secretes increasing amounts of estrogen.
Ends with ovulation.
2. Ovulation (~Day 14)
Mature follicle ruptures.
Secondary oocyte is released into the uterine tube.
Oocyte remains viable for about 24 hours.
3. Luteal Phase (Days 15–28)
Ruptured follicle forms the corpus luteum.
Corpus luteum secretes progesterone.
If fertilisation does not occur, the corpus luteum degenerates and hormone levels fall.
Common pathologies related to reproductive system
Endometriosis:
Endometrial tissue grows outside the uterus.
Causes inflammation, pain and infertility.
Common sites include ovaries and pelvic cavity.
Polycystic Ovary Syndrome (PCOS):
Hormonal disorder causing irregular ovulation.
Can cause infertility and menstrual irregularities.
Explain the process of menstruation.
Occurs when fertilisation and implantation do not occur.
Corpus luteum degenerates.
Estrogen and progesterone levels fall.
Blood vessels in the functional layer of the endometrium constrict.
Endometrial tissue undergoes necrosis and is shed.
The functional layer is lost, but the basal layer remains to regenerate the endometrium.
Menstrual blood and tissue exit through the vagina.
How do ovulation and menstruation influence fertility?
Ovulation releases an oocyte, making fertilisation possible.
The ovum survives ~24 hours; sperm survive ~48 hours.
Fertile window: 48 hours before to 24 hours after ovulation.
Menstruation occurs when fertilisation and implantation do not occur.
Falling estrogen and progesterone cause shedding of the endometrium.
Indicates the previous cycle was not fertile/successful.
How is lactation regulated?
Prolactin
Stimulates milk production.
Oxytocin
Causes milk ejection.
Neurological stimulation when an infant suckling stimulates the release of both hormones.
What is breast milk composed of?
Water
Carbohydrates (lactose)
Fats
Proteins
Antibodies
Vitamins and minerals