6331- Psychopharmacology
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
What are the four parts of a neuron?
soma, dendrites, axon, terminal buttons
describe each of the four parts
soma is the cell body, dendrites are the branches that receive messages through multiple receptors, axon is a long tube that carries messages from the soma to the tb, terminal buttons are at the end of the axon and are small sacs or vesicles that hold NTs and transfers them through a synapse
two ways terminal buttons transfers neurotransmitters
between the terminal button of one neuron to the dendrite of another neuron OR between the terminal button of one neuron to the soma of another
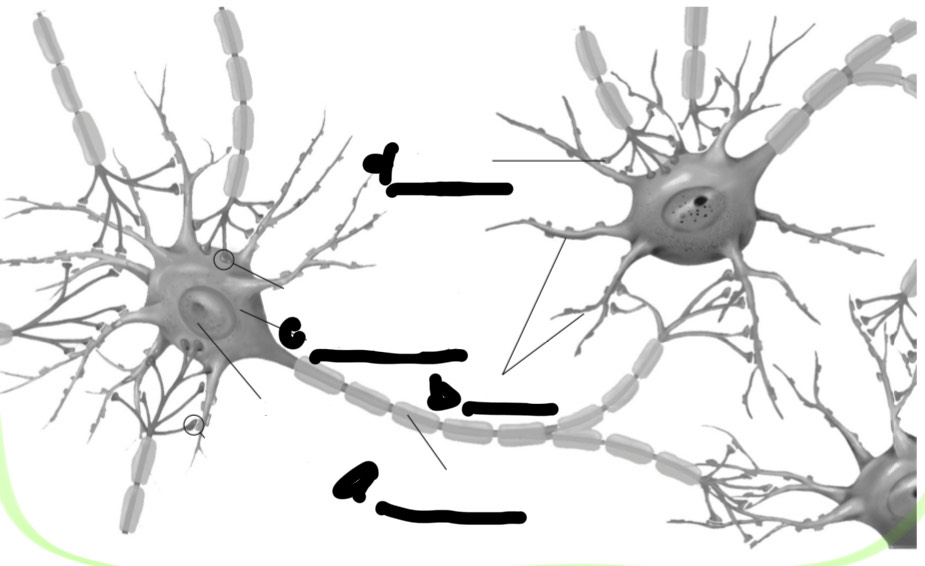
Label all the parts
a. axon
b. dendrites
c. soma
d. terminal buttons
in the grand scheme of things where does neural communication take place and what are the two ways that neurons communicate
in the central nervous system, neurons communicate chemically or electrically
what can activate neurons in the cns, in what two ways
all drugs and substances; endogenous is from within the body (endorphins, insulin, adrenaline) or exogenous which from outside the body and introduced to the body in the same way (caffeine, vitamins, herbs, medications)
Process of neural communication
receptors are stimulated by nt
action potential occurs if enough receptors are stimulated at once and this travels along axon to the tb
At the tb nt is released
travels across synapse from pre to postsynaptic membrane of dendrite where it might interact with receptors
receptors receive signal and activate postsynaptic cell, allowing for retransmission
another name for action potential
electrical impulse
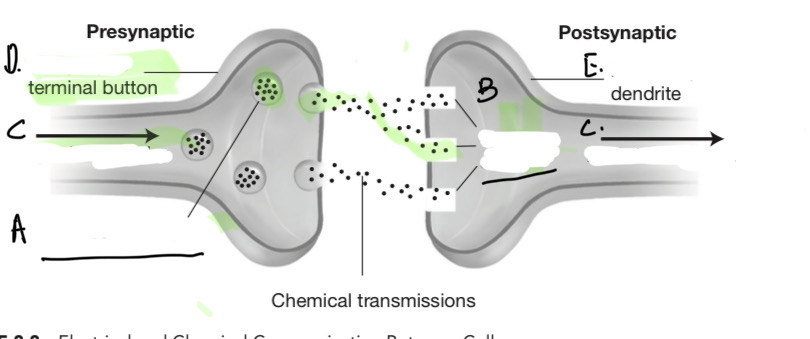
Label the parts
a. neurotransmitters
b. receptor sites
c. electrical impulse (action potential)
d. presynaptic
e. postsynaptic
ions
electrically charged particles that facilitate the electrical properties of neural transmission (most neurons are slightly electrically charged)
resting potential
the difference between intracellular and extracellular ion concentration, typically -70 mV (outside is more negative than inside)
threshold potential
-55 mV
TRUE OR FALSE: some drugs can affect various phases of action potential
true
extracellular space primarily contain
intracellular spaces primarily contain
sodium (Na+) and chloride (Cl-)
potassium (K+)
How many stages does action potential occur in
4 stages: stimulation, rising phase, peak and falling phase, undershoot and refractory period
membrane potential
the potential difference between inside and outside the cell
what is the stimulation phase'
how does this happen
action potential starts when the membrane potential is reduced to the threshold potential
this happens when a receptor is activated by a neurotransmitter which sends excitatory or inhibitory messages
what do excitatory messages do to a cell
depolarize- allows Na+ to flow in - reducing membrane potential and increasing chances of threshold potential
what do inhibitory messages do to a cell
hyperpolarize- allows Cl- to flow in- increasing membrane potential and decreasing the chances of threshold potential
Which actional potentials are expressed
how often do cell receive messages
what size are aps and what cause a stronger behavioral repsonse
the ones that outnumber the other; if there are more inhibitory messages than excitatory messages an ap will not be expressed
neurons receive inhibitory and excitatory messages constantly
all aps are the same size, however the number of aps express a stronger behavioral response
explain runaway and an example
voltage-gated sodium channels openings; tetrodotoxin in pufferfish can cause paralysis by blocking these channels
Rising phase
when ap is triggered and threshold potential is reached, runaway occurs which results in rapid depolarization until +40mV (peak) is reached
the cell tries to compensate for all of the sodium
by taking K+ out by opening channels by they open more slowly at first
peak and falling phase
example of this
K+ eventually catches up to peak and inactivates sodium from flowing in by a small protein blocking the voltage-gate sodium channel opening
potassium overpowers sodium and the voltage drops rapidly
ex: alpha toxins in a scorpion sting can block sodium inactivation this results in a prolong ap that doesn’t have a traditional falling phase and can lead to ataxia or muscle lock
undershoot and refractory period phase
After hyperpolarization the voltage is often lower than the resting potential this begins the refractory period
ion exchangers move Na+ back out and K+ in, this can last as long as an ap however reset is necessary before another ap can happen
when ap or electrical impulse reaches the nerve terminal, neurotransmitters are released by exocytosis
this is helped by calcium (Ca++) ions in the terminal buttons moving neurotransmitters inside of these vesicles to release to the synapse by binding to the cell wall
the nts diffuse across the synapse to the postsynaptic membrane where receptors are activated by ion channels and de or hyperpolarize that neuron
this signaling is over when there are no longer nts present in the synapse, reuptake can occur
Neurotransmitter and receptor sites analogy
are like a key and lock
receptors are specific proteins of amino acid made to be unique
signal transduction process occurs when a nt binds to a receptor…
through ligand-gated ion channel receptors
inducing chemical changes within the cell (many are G-protein-linked receptors because they bind guanine nucleotides these are dopamine, glutamate, gamma aminobutyric or GABA)
And changes it’s physical shape
some receptor sites are g-protein-linked receptors (bind guanine nucleotides these are dopamine, glutamate, gamma aminobutyric or GABA) and the bindings actuate the second messenger which is cyclic adenosine monophosphate or cyclic AMP
cyclic AMP actuate other molecules or enzymes that excite or inhibit other chemicals and it results in protein kinases
protein kinases changes the physical shape of the protein and that controls the opening of ligand-gated ion channel receptors
3 main nts of emotion and behaviors? what are the differences?
monoamines: two catecholamines (dopamine and norepinephrine) and one indolamine (serotonin); the difference between the two is based on the chemical structure
What are other nt that attribute to emotion and behavior
Amino acids: GABA, glycine, glutamine
Neuropeptides (chains of aa): substance P and endorphins
Dopamine and Norepinephrine are synthesized from what? how is it absorbed
Tyrosine
amino acid that comes from diet (meat, poultry, seafood, beans, tofu, lentils) and can be synthesized for purchase
enzyme DOPA decarboxylase converts tyrosine into L-DOPA and dopamine
dopamine from here can turn into norepinephrine by enzyme dopamine B-hydroxylase
Norepinephrine function
regulation of sleep-wake cycles, sustained attention, alertness, biological responses to new stimuli
noradrenaline function
mediate anxiety, fear, stress, and responses, thus plays role in mood and anxiety disorder with low levels
Serotonin aka… Comes from…
5-hydroxytryptamine (5-HTP) is synthesized from tryptophan by the enzyme tryptophan hydroxylase
comes from milk, sunflower seeds, bananas
serotonin function… low levels of this are asoociated with what?
brian functioning including mood, anxiety, arousal, irritability, tranquilitu, cognition, appetite, sleep-wake cycles, and obsessions
(low levels of serotonin are associated with anxiety, mood and psychotic disorders)
Agonists
increase the availability or action of nt by binding to receptors and acting
antagonists
decrease the availability of neural communication by binding to receptors and blocking
Acetylcholine: excitatory or inhibitory/ cns or pns
affects memory, learning, behavioral arousal, attention, mood, and REM sleep in CNS
found at synapses where nerve terminals meet the skeletal muscles causing excitation leading to muscle contractions in PNS
what is another name for epinephrine? explain where it is found and what it does
adrenaline
more active and is secreted by adrenal glands (small endocrine glands above the kidney) in PNS
regulates flight or fight responses
Norepinephrine: excitatory or inhibitory/ pns or cns
primarily an excitatory nt, has axons in the brainstem that project into the limbic system and frontal lobes in the CNS
regulates wakefulness and alertness
dopamine: excitatory or inhibitory
regulates behavior, movement, learning, mood and attention'; may have excitatory and inhibitory effects in the brain
overactivity or oversensitivity may play a role in schizophrenia
drugs of abuse directly activate dopamine receptors
serotonin: excitatory or inhibitory
key nt in homeostasis in the brain and involves inhibition of activity and behavior
regulates mood, appetite, sleep and arousal, pain
projects into almost the same areas as norepinephrine (limbic and frontal lobes)
Other neurotransmitters that affect mood and behavior and their functions ( 3 G’s excitatory or inhibitory)
GABA makes brain more stable by dec neural transmissions; benzodiazepines and barbiturates increase levels of GABA
glycine inhibits amino acids neurotransmissions mostly in the spinal cord; when glycine receptors are activated the cell becomes hyperpolarized and less likely to transmit signals; strychnine is a toxin that blocks receptors this leads to overexcitation and possibly death
glutamate is an aa nt that is excitatory and lowers the threshold; found Asian food in the form og monosodium glutamate (MSG) which excites the taste buds
Psychodynamics
study of how drugs affect receptor sites, send signals, and cause some neuro chemicals; at the synapse
Pharmacokinetics
administration, absorption, distribution, metabolism and elimination of a drug inside the body
Routes of administration (other names for them)
orally, subcutaneously (deep tissue injection), intramuscularly (IM or muscle injection); intradermally (dermal injection), intranasally; inhalational, sublingually, transdermally, (skin absorption), intravenously (IV)
Which route is most common? quickest? used in hospital or clinic settings to control behavior or in long-acting forms for more chronically ill patients?
oral; inhalation; intramuscular
What are soltabs? What are some examples
orally disolved tablets
olanzepine (Zyprexa Zydis)
mirtazapine (Rameron Soltabs)
risperidone (Risperdal M-tab)
Clonzepam (Klonopin Wafers)
Which routes are absorbed the fastest
intramuscular, intravenous, etc are absorbed faster than oral drugs and oral liquids are faster than capsules or tablets
What are the benefits of slower or extended release tablets
they allow for fewer doses and in turn cause fewer side effects because there is a slower rate of absorption
the process of how oral drugs are absorbed
starts in the stomach and duodenum (first segment of the small intestines), into the venous system, and delivered through the circulatory system
the liver is the first organ to receive oral drugs, it breaks it down into actives and non actives during first-pass metabolism and into the bloodstream
Can certain diseases and their treatment affect absorption
yes, gastrointestinal diseases and their treatment can affect absorption and example of this are antacids interfere with some antibiotics
After the liver breaks down the drug what do they turn into and where do they go? What is this process called
active metabolites that can be readily absorb are sent to their target organs via the bloodstream and non-active metabolites are expelled. This process is called first-pass metabolism
What is the target for psychotropic drugs after first pass metabolism
the central nervous system
What are some examples of intramuscular or IM drugs
haloperidol (Haldol Decanoate
fluphenazine (Prolixin Decanoate)
Risperidone (Risperdal Consta)
what factors affect absorption
protein binding, drug half-life, lipid solubility
what is protein binding? what is an example and purpose?
when a drug binds tightly to plasma protein
example is albumin in the bloodstream
this determines how much of the drug is available to act on the brain by hindering the drug’s metabolism and excretion causing it to remain in the circulatory system longer
what is drug half-life? what’s an example? how many half-lives are needed for a drug to completed be eliminated
the average amount of time required to eliminates one half of the drug’s concentration
Xanax has a half like of 11 hours, after 11 hours it’s concentration in the body is reduced to 50%, after 22 hours it’s concentration is reduced to 75%, after 33 hours it’s concentration is reduced to 87.5%, after 44 hours- 93.8%, after 55 hours- 96.9%
5 half-lives
what is lipid solubility? What are lipophilic drugs and what happens to drugs that arent lipophilic? what is it also called?
how easily a drug crosses a cell membrane
drugs that are more likely to cross over the blood-brain barrier and extert their effect, other drugs don’t cross the blood-brain barrier and do not get to exert their effect on the central nervous system
fat solubility
drugs are metabolized by what enzyme… what happens because of this
the 9450 enzyme family
drugs compete for the same pathways and drug interact because of this
regarding decreased liver enzymes what should you look out for… are all drugs metabolized by the liver
geriatric patients have dec liver enzumes, so their doses need to be reduced to avoid toxicity
medical conditions such as viral hepatitis and liver cirrhosis may also dec metabolism
some medication arent metabolized by the liver and are excreted unchanged by the kidneys in urine (ex: lithium or Lithobid)
What makes up the therapeutic index? explain
the ration of therapeutic dose and the toxic does makes up the therapeutic index
a toxic dose is when a drug concentration produces mild or severe side effects
a therapeutic dose is when a drug concentration gives a desired response
high versus low therapeutic index and example of low
high therapeutic index are desiriable drugs because the ratio is far from each other
low therapeutic index is risky because the margin is slim (lithium)
dose-response curve
considered when determining a therapeutic dose
when a drug is introduced, there is a slow titration upwards and that usually corresponds with an increasing response
at certain point the drugs levels off and increasing the dose at this point would only increase the risk of side effects and toxicity
loading doses
higher dose to obtain a certain response; seldom adjustments are needed
tolerance and tolerance with alcohol
needs greater amounts of drug over time to produce desired effect
this develops over time with alcohol
withdrawal and withdrawal with alcohol
set of characteristic symptoms that emerge when a drug is abruptly discontinued after heavy and prolonged use
if alcoholic suddenly stops drinking, it throws the body in a state of shoch which can cause tremors, agitation, insomnia, hallucination, and even seizures
discontinuation syndrome and example drugs
not medically dangerous like withdrawals
paroxetine (Paxil) or venlafaxine (Effexor XR) may cause malaise or flulike symptoms when patients missed a does or stops medication
potentiation
when one drug may enhance the effect of a second drug
synergism
when one drug may enhance the effec of a drug significantly more than expected
alcohol and benzodiazepines
placebo response and noceno
when the brain acts as if the drug was present even though it isent
when it causes negative effect
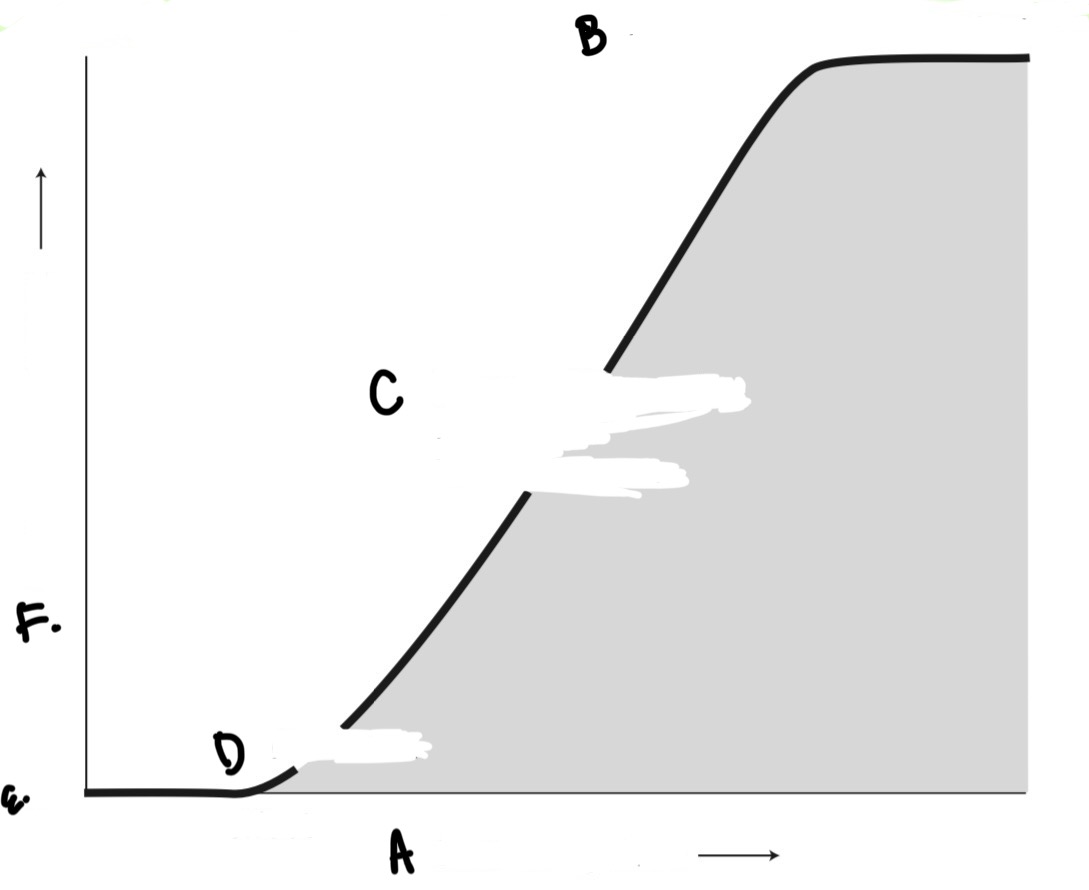
label all of the parts
a. increasing dose
b. range of maximum effect
c. range of increasing effect with increasing dose
d. threshold
e. range of no effect
f. increasing response
Latin Abbreviation and meanings
a.c.
b.i.d.
cap.
c with bar on top ( c )
h.
hs
p.c.
p.o.
p.r.n.
q4h
q6h
qd*
q.i.d.
q.o.d.*
Rx
stat.
tab.
t.i.d.
before food
twice a day
capsule
with
hour
at bedtime
after food
by mouth
as needed
every 4 hours
every 6 hours
every day
four times a day
every other day
prescription
immediately
tablet
three times a day
Latin Abbreviation and names
a.c.
b.i.d.
cap.
c with bar on top ( c )
h.
hs
p.c.
p.o.
p.r.
q4h
q6h
qd*
q.i.d.
q.o.d.*
Rx
stat.
tab.
t.i.d.
ante cibum
bis in die
capula
cum
hora
hora somni
post cibum
per os
pro re nata
quaque 4 hora
quaque 6 hora
quaque 1 die
quarter in die
quaque altera die
recipere
statim
tabella
ter in die