NMS I - Exam 1 (VBI, CB, DC, ect.)
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
If a pt has head and neck pain, what should be evaluated
think vascular = VBI (stenosis)
Cerebral vascular ischemia
heachaches, diplopia, drop attacks, dysarthria, dysphagia
Absolute contraindications
VBI
major artery aneurysm
acute arthropathies and acute freactures
malignancies
myelopathy or cauda equina symptoms
Relative contraindications
hypermobility
demineralization of bone
benign bone tumors
bleeding disorders
radiculopathy w/progressive neurological signs
Stethoscope for bruits
diaphragm = high sounds
bell = low sounds
Barre-Lieou
causes compression of vertebral arteries to try to elicit symptoms
If any of the VBI tests (VBA functional maneuver, Barre-Lieou, DeKleyn’s) are positive what three further imaging should be done
1) MR angiogram of head
2) MR angiogram of neck
3) MRI of head
The body will fall ____ the side of the cerebellar lesion
towards
Six cardinal fields of gaze revealed nystagmus in right eye when looking to the right
cerebellar lesion on right involving flocculonodular lobe
Cerebellar tracts are _________ and produce ipsilateral findings
double crossed
Where does cerebellar tracts cross
1st - superior cerebellar peduncle in midbrain
2nd - corticospinal and rubrospinal tracts (pyramidal decussation)
Cerebellar lobe functions - Hemispheres
appendicular coordination (UE + LE)
finger to finger, finger to nose, heel to shin
Cerebellar lobe functions - Vermis
gait and axial coordination (walking and trunk)
tandem gait, hopping on one leg, squatting on one leg
Cerebellar lobe functions - Flocculonodular/Vestibulocerebellum
connections with vestibular nuclei (eye and gross balance)
vestibular function and connections w/labyrinth
Pt falls with only eyes closed = DC deficit below lesion
sensory ataxia
classic findings of Tabes dorsalis or B12 deficiency (MC)
syringomyelia
What poisons vermis producing a widened gait
alcohol
Hypermetria vs Hypometria (finger to nose, finger to finger)
hypermetria = over shooting
hypometria = undershooting
What abnormality can be found in finger to nose to finger (eyes open ONLY)
dyssynergia (incoordinate movement)
What two things can be found in heel to shin
dyssynergia
dysmetria (inaccuracy in measuring distance)
Abnormality found in RAM (diadochonkinesia)
dysdiadochonkinesia = cerebellar dysfunction
Abnormality from Holmes Rebound test (eyes open and closed)
loss of check reflex
What part of the cerebellum is being evaluated during tandem gait
vermis
Posterior cord syndrome (infarction of posterior spinal artery)
loss of vibration, proprioception, reflexes below level of lesion
**Note: pain, temperature, muscle strength are spared
Anterior spinothalamic tract carries what sensation
light touch
Lateral spinothalamic tract carries what sensation
sharp pain and temperature
Cuneatus tract (UE) and Gracilis (LE) of dorsal columns carry what sensation
vibratory sensation, proprioceptive info, 2pt touch discrimination
Posterior cervical disc herniation affects _____ part of the spinal cord first
anterior
effects anterior and lateral spinothalamic tracts
Discriminating local touch name
topesthesia
Deep pain and topesthesia is initiated by
corpuscles of Meissner
Sensation is carried by primary large diameter heavily myelinated fibers through
posterior/dorsal spinal cord district
Your static and motion palpation exam findings reveal that your pt experiences pain BEFORE end range with your passive ROM
pt has an acute condition
Your static and motion palpation exam findings reveal that your pt experiences pain AS end range is reached with your passive ROM
pt has a subacute condition
Your static and motion palpation exam findings reveal that your pt experiences pain AFTER end range with your passive ROM
pt has a chronic condition
Resisted muscle testing of right triceps muscle reveals that is painful and strong
pt has a minor sTrain (Tendon)
2pt touch discrimination normal values
Finger tips = 2-4mm
Dorsum of fingers = 4-6mm
Palm = 8-12mm
Dorsum of hand = 20-30mm
Nosognosis
ability for pt to know that they are ill (pt will deny there is a problem)
Medial side of ring finger is innervated by
ulnar C8
Lateral side of ring finger is innervated by
median C8
Nerve root Irritation (NRI)
hyper’s (inc sympathetics)
instrumentation break AWAY from involved side (vasoconstriction/hypothermia)
Nerve root compression (NRC)
hypo’s (dec sympathetics)
instrumentation break TOWARDS involved side (vasodilation/hyperthermia)
NRC means the nerve is
dying
Sensory/Motor/DTRs exams exhibit abnormal or decreased findings with NRC, what sensations are lost 1st
1) autonomics
2) light touch
3) sharp pain and temp
4) vibratory sensation
Sensory/Motor/DTRs exams exhibit abnormal or decreased findings with NRC, what sensations are regained 1st
1) vibratory sensation
2) proprioception
3) pain and temp
4) light touch
Paresthesia (abnormal sensation like tingling/burning) + instrumentation break AWAY from involved side
NR irritation
Anesthesia (absent sensation) + instrumentation break TOWARDS involved side
NR compression
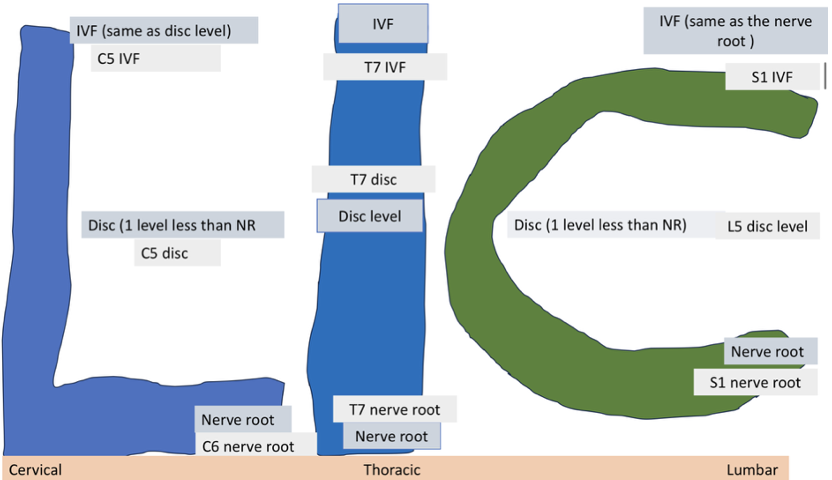
SOL in Cervicals (L)
IVF = same as disc level (C5 IVF)
Disc = below NR level (C5 disc)
NR = C6
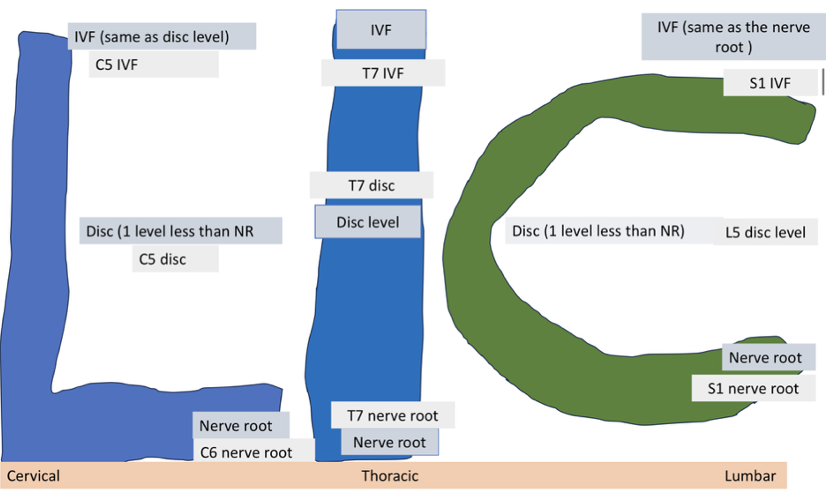
SOL in Thoracics (I)
IVF = same as disc level (T7 IVF)
Disc = same as NR level (T7 disc)
NR = T7
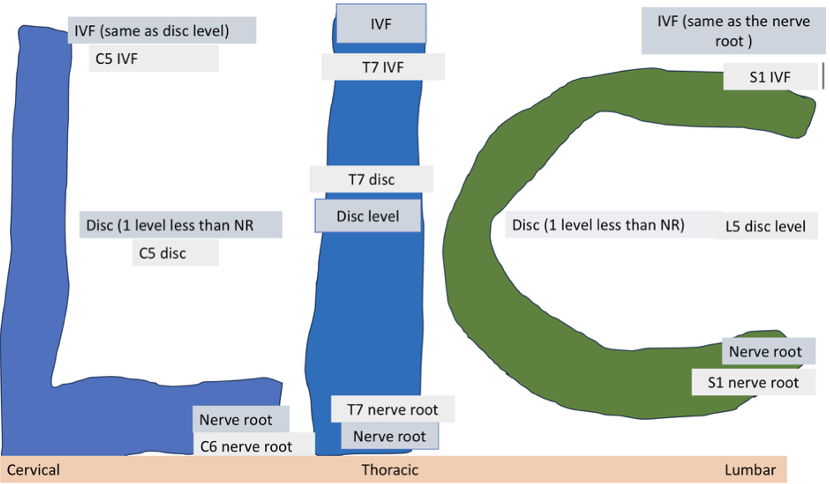
SOL in Lumbar (C)
IVF = same as NR level (S1 IVF)
Disc = below NR level (L5 disc)
NR = S1
What is the easiest and best way to check motor nerve function
strength tests
In a motor exam, the voluntary motor impulses are initiated in the
primary motor cortex of frontal lobe in pre-central gyrus
Muscle exams assess
strength, tone, and volume
UMNL symptoms
spacticity, hypertonia, hyperreflexia
Spasticity
increased muscular resistance felt by examiner during quick joint movement that quickly fades away
Clasped knife (tension at first followed by decreased tension as joint is opened)
Cogwheel rigidity
joint give way with passive motion (seen in Parkinson’s)
Hypertonia (Gooseneck rigidity)
resistance felt through its entire ROM
lesions of extrapyramidal tract
Release phenomena
exaggerations of normal neurological function due to loss of cortical inhibition
LMNL (NRC) symptoms
flaccidity, hypotonia, hyporeflexia
Hypotonia
neurological damage at the level of the reflex arc
example: cerebellar disease (intention tremor)
Deficit phenomena
reductions in muscle tone, DTRs, muscle strength, muscle volume
Neural shock that caused injury first cause ONLY
peripheral type neurological findings (3-4wks before becoming hyperactive)
Antigravity muscles are _____ than their antagonists
stronger
Kinetic power
force exerted on a changing position (lifting barbell off rack in bench press)
Static power (-)
exerted in resisting movement (lowering barbell to chest in bench press)
Extrapyramidal syndrome ______ kinetic power while static remain normal
DECREASE
Muscle grading
0/5 - no evidence of contraction
1/5 - evidence of slight contraction but no joint motion
2/5 - complete ROM gravity eliminated
3/5 - complete ROM enough strength to put joint through normal ROM
4/5 - complete ROM against gravity with some resistance
5/5 - complete ROM against gravity with full resistance
Muscle strength - Supraspinatus
C4, 5, 6
Suprascapular N
Muscle strength - Deltoid
C5 + 6
Axillary N
Muscle strength - Biceps
C5 + 6
Musculocutaneous N
Muscle strength - Brachioradialis
C5 + 6
Radial N
Muscle strength - Wrist extension
C6, 7, 8
Radial N
Muscle Strength - Triceps
C6, 7, 8
Radial N
Muscle strength - Wrist flexion
C6, 7, 8
Median/Ulnar N
Muscle strength - Finger extension
C6, 7, 8
Radial N
Muscle strength - Finger flexion
C7, 8, T1
Median/Ulnar N
Muscle strength - Finger abduction
C8 + T1
Ulnar N
Muscle strength - Finger adduction
C8 + T1
Ulnar N
DTRs
Biceps = C5
Brachioradialis = C6
Triceps = C7
Finger flexion = C8
Grading DTRs
0 - areflexia
+1 - sluggish or diminshed
+2 - normal
+3 - slightly hyperactive
+4 - hyperactive w/transient or sustained clonus
Jandrassik’s maneuver (reinforcement)
pt squeezes their glutes, knees, bites down, hand in hand pull apart
**Can’t say diminished unless tried reinforcement first
Cervical spine - midline disc herniations create
myelopathies (cord lesion)
Cervical spine - lateral disc herniations compresses
NR below
Cervical spine - hypertrophic changes of C5 uncinate will compress
C5 NR (SAME LEVEL)
Lumbar spine - midline disc herniations compresses
NR below
Lumbar spine - Foraminal (far lateral) disc herniation compresses
NR at same level
If lesion is in brain, clonus will be on
contralateral side
If lesion is in spinal cord, clonus will be on
ipsilateral side