Fetal Physiology
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
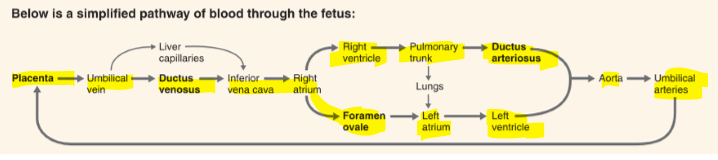
fetal circulation
Fetal heart
Pumps blood through both the fetal circulation and the placenta
Youd think increased pressure load of the heart but Placenta acts as a large, low resistance vascular bed - allows blood to flow easily through circuit
Increased CO but not pressure load
Low stroke volume so required high heart rate 110-160
How does fetal blood flow change as it grows and demand increase?
Placenta becomes more vascularised increasing its capacity to exchange nutrients
Increase in FCO so that more blood is directed to the placenta over time
Cardiac growth and development
Initially Hyperplasia (increase in cell number)
32 weeks onwards - heart cells start to from 2 nuclei
after birth cells only get bigger not more (hypertrophy)
Pronephros
First Kidneys
Day 22
6-10 pair of tubules connected to the wolffian duct
non-function in humans
Mesonephros
5th- 11th week
Small amounts of urine produced
Humans develop about 40 mesonephric nephrons
Metanephros
Permanent kidney
starts week 5 - overlaps
Adult like nephrons which continue to branch until 36 weeks
urine produced from the 16th week - amniotic fluid
Amniotic fluid improtance
Breathed in by the fetal lung and helps with lung development
fetal kidney overall
born with all the nephrons we are ever going to have
nephrogenesis involved repeated branching events
disruption of these may theoretically halve nephron number
Affected by chemicals, stress and drugs
Fetal lung development timing
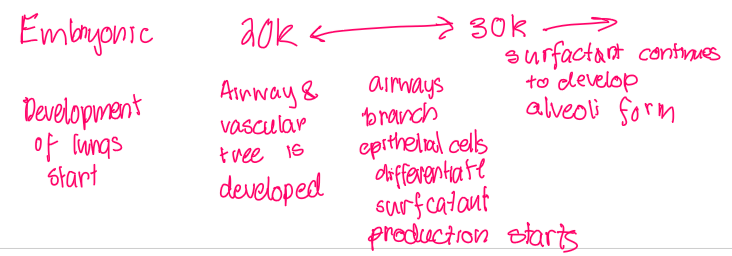
Surfactant
prevents the collaps eof alveoli during breathing
If not well enough developed causes - RDS in newborn
Fetal gastrointestinal system
Feces accumulated in the intestines from week 13
Liver makes RBC peaking at 16 weeks and continuing till term. many liver functions ae performed by placenta
Meconium
meconium consists of amniotic fluid, cellular debris, musus and bile
Fetal skin in embryonic period
Two layers
1. periderm - sloughs off to form vernix
2. inner basal layer - epidurmis and glands
Fetal skin
All layers of epidermis are present by week 20
preterm babies dont have vernix
causes water loss and poor temp control
Fetal brain
12-20 weeks form neurons that become nuclei
migrate to developing cortex and deep nuclei where they will reside for life
massive proliferation, differentiation of neurons and glia and organisation of brain regions
Biggest neural proliferation 8-15 weeks
Process in fetal brain formation
Synaptogenesis - connections between neurons
Apoptosis - selective neuronal loss
synaptic pruning - removing of connections
Neonatal period
moment of birth to day 28
Transitional events at birth
Baby need to start using its own lungs for gas exchange and the circulatory system has to start functioning as an adults
Factors that trigger transitional events
Blood flow from the umbilical cord stops - reducing pressure in heart
The lungs expand - blood flows to lungs
Cardiovascular transitional changes
Change in pressure in teh atriium and lung results in the flowing changes
Closing of ductus venous, foramen ovale and ductus aterious
Blood flow sthrough lungs and fills left atrium
left venticle has to work harder
respiratory transition chnages
Fluid clearance, changes to vascular flow, surfactant secretion, alveolar distention and establishment of breathing is needed
How does baby take first breath
Normal labour compresses the cord and lead to increased fetal CO2 and reduced oxygen - exaggerated once cord is cut
Shift stimulating change in teh respiratory centres of the brain to cause the first breath
Fluid drainage from lungs
ENAC - helps reabsorb lots of fluid from the lungs, starting a few days before natural delivery
During birth - chest wall of baby is compressed which helps clear remaining fluid
After birth - lymphatics and vacsular drainage, breathing removes some
Delayed cord clampung
More gas exchange
more iron and more fRBC
Respiratory distress syndrome
caused by insufficent surfactant in lungs - causing alveoli to collapse
Treatment involved Respiratory report, maybe survanta
If babies need respiratory support by 36 weeks gestational equivalent - termed chronic lung disease or bronchopulmonary dysplasia
Hemogobin Fetal vs adult
Fetal hb - 2 alpha and 2 gamma chains
making it better at takeing up oxygen not giving up
Adult hb - 2 alpha and 2 beta chains
Easier fro fetal blood chells to take oxygen from adult blood cells
Transition from fetal to adult Hb and RBC
Lowered RBC formation until about 6 weeks after birth due to ris ein oxygen that decreased EPO
Slowly fetal hb is replaced - until about 3 months
Bilirubin formed
Jaundice
A condition characterized by yellowing of the skin and eyes due to high levels of bilirubin, often more common in preterm infants.
Immature liver - lower bilirubin clearance
the faster RBC turnover - more bilirubin builds up
Can cause brain damage
Vitamin K and the newboen
Newborn cannot make vitamin K, not passed through placenta
at risk of hemorrage
Digestive system changes
Baby not used to having food move through intestine and needs to adapt
Probiotics for GUT reduces risk
APGAR
Universally scored system for assessing a baby’s health right after birth
1 and 5 mins
7 or more is normal

Pulse oximetry screening
Pulse oximetry looks for hypoxemia - sign of Critical Congenital heart disease
In term babies
O2 sats >95% - discharge
O2 sats <90% - admit to neonatal unit
Guthrie screening test
NNST
blood obtained from a heel prick and applied to a paper card
DNA obtained from the white blood cells for assessment of serious genetic diseases
Cystic fibrosis, phenylketonuria, congenital hypothyroidism, galactosaemic, spinal muscular atrophy
Postnatal hypoglycemia
Too low blood sugar of baby
Fetus builds up glycogen stores close to term but can only last so long. when runout, baby may start ketogenesis and lactate formation until milk can provide energy
Neonatal Hypoglycemia risk factors
Most common reasons for babies to spend a short amount of time in the special care nursery
IUGR babies - little fat to form ketones
Babies of diabetic women - adapted to higher glucose needs
Traumatic births/ long labour/fetal distress
Early growth in first few weeks
may loose up to 10% of weight
Usually due to loss of extracellular fluid but also change in the way baby obtains nutrients
should regain birth weight by 2 weeks of age
Growth of baby on growth charts an dthe goal is not not deviate much from the birth weight
Failure to thrive
Weight below 3rd centile
or
Dropping two major percentile lines over time
Nutrients required for the newborn
6 week old baby weighing 40kg may require over 600mls of milk per day
size of stomach is small, feeding must be frequent
Reasons fro failure tothrive
Inadequate food intake
inability to properly utilise food - reduced digestion or aborption
accessible energy utilisation - hyperthyroidism, coming of oxygen
Loss of nutrients - reflux
Skeleton of the infant
Spinal colum contains 33 separate bones (9 fuse and form 2 bones - scrum/coccyx)
Two primary curvatures care C shape spine
Most bones are well ossified except for the epiphysis. long bone growth until puberty ends
Fonatenel may last up to 2 years
Cranium large compared to rest of the face
Lungs of infant
As skeletal growth the chest increases - lung growth occurs
alevolar growth
Brain of infant
Synapses forming with all new information exposed to all senses
most rapid synaptogensis happens aright around birth
every second hundreds of millions of synapse are formed
Brain development of infant
Newborn quickly learns to distinguish voices, sounds, people and facial expressions
prefer speech from the language of their parents
Risk factors for preterm birth
Age of mother
Ethnicity
Smoking
Stress
Late or no antental care
low socio-economic status
High or low BMI
previous PTB
genital tract infections
IVF - assisted reproduction
Multiple gestation
Chronic or acute medical donsitions
Most common cause of neonatal death
preterm birth
Corticosteroids for PTB
Risk of PTB 24-34 weeks
betamethasone injections x 2
ensure Fetal lung is more fully developed
Tocolytic drugs for PTB
Anti contraction medication - can delay preterm labour longe enough to provide corticosteriods
Neuroprotectant for PTB
Magnesium sulfate
reduces cerebral pulsy
less than 30 weeks
Consider if between 30-33+6 weeks - preelcmpsia
Loading dose 4g over 2-, 1g maintence
Acute complications of PTB
Respiratory distress syndrome - resp support, low surfactant
Gastrointestinal complications - cannot coordinate breathing, sucking and swallowing - tube feeding
Jaundice - immature liver
skin not developed - dehydration and temp loss
Cardiovascular - patent arteriosus, brady, hypotension, iron deficnecy
Chronic complications of preterm birth
25% of preterm babies are visually impaired
10% are hearing impaired
40% chronic lung disease
Unquantified riks of heart disease and diabetes
LBW
Less than 2500g
FGR or IUGR
clinical features of in utero growth retardation
because of a pathology
higher stillbirth risk
sevre - less than 3rd centile
Early less than 32 weeks
late - after 32 weeks
SGA
(below 10th centile)
could be constitutively small or growth restricted
How is fetal growth restriction monitored
Fundal height
USS should be considered if reason to suspect slowing growth need over 3 consecutive though
Still birth
Usually due to congenital defects, suboptimal care contributes, placental insufficiency, maternal illness, fetal hypoxia, oxidative stress
Miscarriage
fetal loss before the time it could survie outside th womb
before 20 weeks QLD
75% before 12 weeks
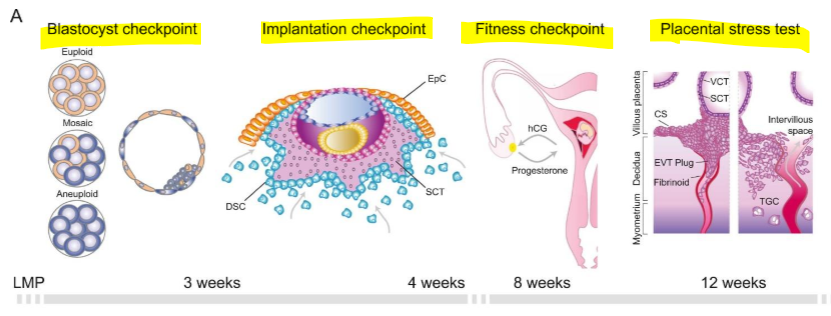
Checkpoints for continuing pregnancy
Embryo/fetus may be lost at such checkpoints
Types of miscarriage
Threatened - Bleeding occurs before 20 weeks, no pain, cervix closed, pregnancy continues
Inevitable - Cervix open, bleeding and pain
complete - pregnancy ended and both fetus and pregnancy tissue have been passed
incomplete- some but not all of preganancy tissue hase been passed - bleeidng or infection
Blighted ovum - embryo has not devloped, placenta and empty sac
Recurrent miscarriage
2-5% of women
2-3 ina row
Cause, genetic, hormonal, immunological incompatibility, environment
recurrent miscarriage and the immune system
HLA proteins regulate tolerance of the baby
HLA in the mother and father must be similar enough but not the same
can lead to Immune rejection of babay
Transient Tachypnea of Newborn (TTN)
A respiratory condition that can occur if fluid does not clear from the lungs after birth, potentially requiring respiratory support.
Congenital disorder
Birth defects - structural or functional anomalies that occur due to abnormal developmental processes
What causes a congenital disorder
Environmental factors - drugs, alcohol, infection, medications
Parental factors - age, blood pressure, glucose, hormone concentrations
Genetic factors - single gene defect, chromosomal abnormalities
Genetics
Many babies are exposed before a women realises she is pregnant or changes in behaviour
It atkes around6 weeks for women to recognise they are pregnant and the most sensitive period to teratogen are between weeks 3-8
Fetal alcohol syndrome
Caused by alcohol exposure
Includes facial anomalies, growth deficiency, cognitive an behavioural issues
FASD vs FAS
FAS is a specific condition wherase, FASD is a spectrum of disorders
Poor learning/concentration
soical and commuincation problems
anxiety and mood dysregulation
facial features
lwo birth weight
heart, kidney, metabolic consequences
Micronutrient deficences
Folate, iodine and selenium
Genetic causes of embryonic defects
Advanced maternal age increases the risk of genetic defects
Consanguinity - related parents
Single gene defects
chromosomal abnormalities
Aneupoldiey - disruption of normal chromosme number Trisomy extra, monsomy missing
Trisomy 21- down syndrome
13 and 18 make it to term but survive days -months
Turner syndrime-45 X
Klinefelter’s syndrome XXY
Hypospadias
Displaced urethral meatus opening in males
Congenital uterine anomaly
4% of population
Most comoal is septal uterus
Ventricular septal defect
Hole in thE heart
Oxygen rich and oxygen poor blood mix
Renal agenesis
When one or both kidneys fail to develop
reduced anmiotic fluid
lungs dont dvelop properly
UNilateral can live with
cleft lip and palate
Can sometimes be picked up prenatally
Many differnt variations - unilateral vs bilateral, complete vs incomplete, lip and cleft or just one
Specal bottles needed to feed until surgery
neural tube defects
Failure of normal neural tube closure
Spina bifida - incomplete closing of the caudal neural tube - incomplete lumbar spinal column
NIPT
DNA of fetal origina can be detected in the maternal blood
10 weeks
not medicare
First trimester screen
11-13
assess anatomical features of the fetus
Nuchal transcalency thickness
Papp-a decreased in trisomy preg
B-HCG
increasing in Trisomy 21, decreased in others
blood test
second trimester screen
18-20 weeks
picking u major phsyical abnormalities in the baby
Diagnostic
Amniocentesis after 15 weeks
chronic villi sampling before 14 weeks