Substance-related and addictive disorders
1/12
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
13 Terms
How psychologists conceptualise and diagnose addiction to substances
-drug/substance? → any substance that exerts an effect on body or mind (prescription,
legal and illicit)
-effect may be neurophysiological (respiratory, tachycardia, dilatation), behavioural
(sedated, aggressive), emotional (excitement, confidence), cognitive (impaired
judgment and memory)
-drugs classified by induced effects
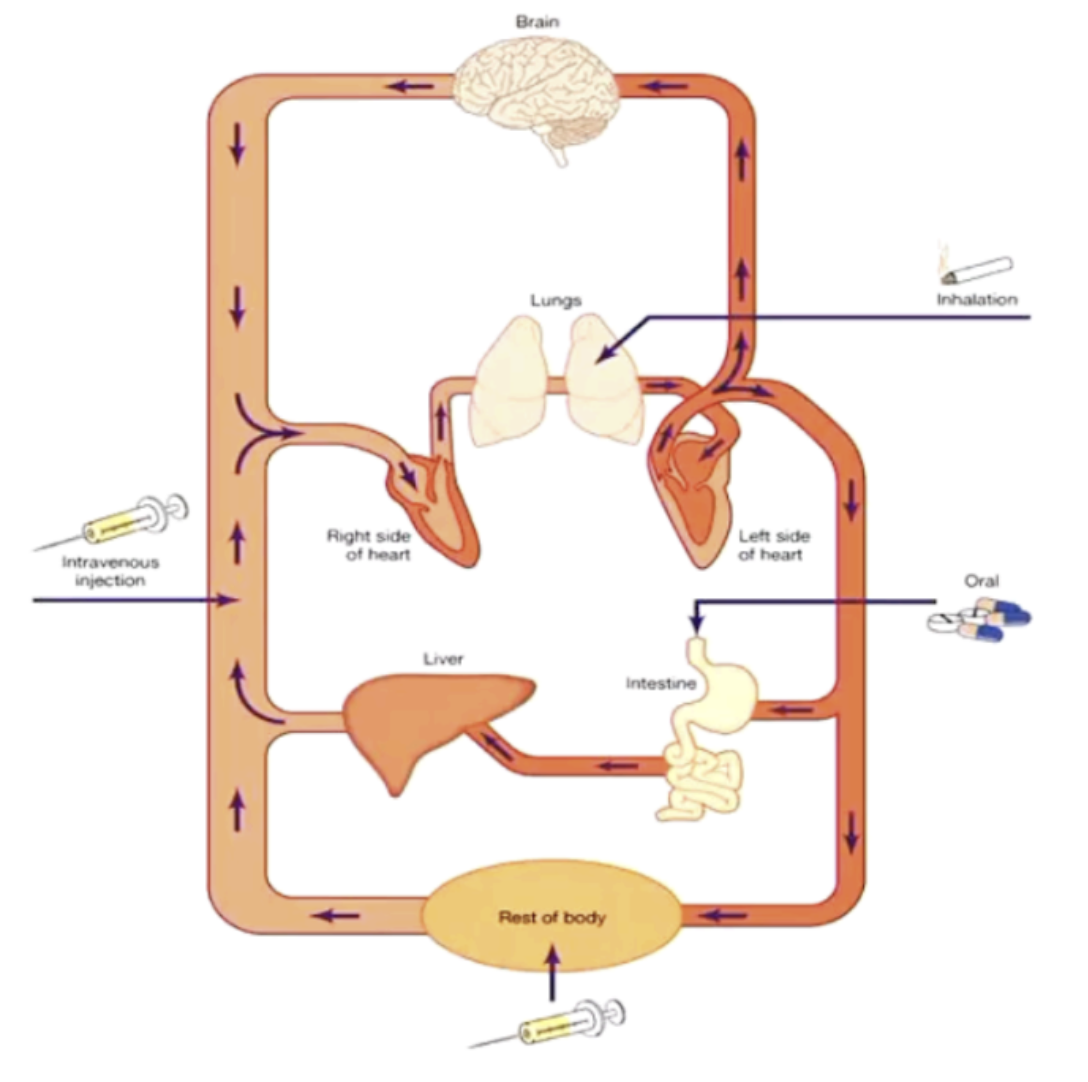
Roles of drug administration (intravenous, inhalation, oral)
Diagnosis of substance use disorders
changes over time (DSM IV : substance dependence and substance abuse)
● DSM-5 (substance related and addictive disorder) → substance use disorders
and substance induced disorders [non substance related behavioural addictions
→ gambling]
● DSM-5 : substance related and addictive disorders → covers diagnostic criteria
for 9 separate classes of drugs : alcohol, caffeine, cannabis, hallucinogens,
inhalants, opioids (heroin), sedatives, hypnotics OR anxiolytics (valium),
stimulants (cocaine, methamphetamines), tobacco
*substance use disorder does not apply to caffeine (ONLY caffeine withdrawal disorder)
DSM-5: Substance-related disorders
● Criterion A
1) impaired control →
- use of amounts or for longer periods than intended
- repeated unsuccessful attempts to cut back/cease
- excessive time obtaining substance or recovery from use
- craving
2) social impairment →
- failure to meet obligations : home, work, school
- social & interpersonal problems, social, occupational or recreational activities reduced
3) risky use →
- use in physically hazardous situation
- persistence despite awareness of physical or psychological problems exacerbated by
use
4) pharmacological indicators (indicative of neuro-adaptation) → tolerance, withdrawal
● Severity of substance use disorder → substance use disorders occur in broad
range of severity from mild to severe with severity based on the number of symptom criteria endorsed (at risk, mild : 2-3 symptoms, moderate : 4-5 symptoms, severe = addiction : 6+ symptoms)
● Comorbidities of substance use : 60% substance users have a comorbid psychiatric disorder → compared to general population : patients w mood/anxiety disorders twice as likely to suffer substance disorder AND patients with substance disorders twice as likely to suffer a mood/anxiety WHY?? → overlapping genetic vulnerabilities, overlapping env triggers, involvement of similar brain regions, interactive effect → drug/other disorders can increase vulnerability to the other
What are the core clinical components and issues for intervention
-Principles of effective treatment
● No single treatment is appropriate
● Treatment needs to be readily available and accessible
● Effective treatment involves and attends to multiple psychological, medical and social interventions and needs (CBT, naloxone, antabuse, methadone, peer support)
● Dual diagnosed clients should have both disorders treated in an integrated fashion
● Treatment does not need to be voluntary to effect change
● Recovery from drug addiction can be a long term process and frequently requires multiple episodes of treatment
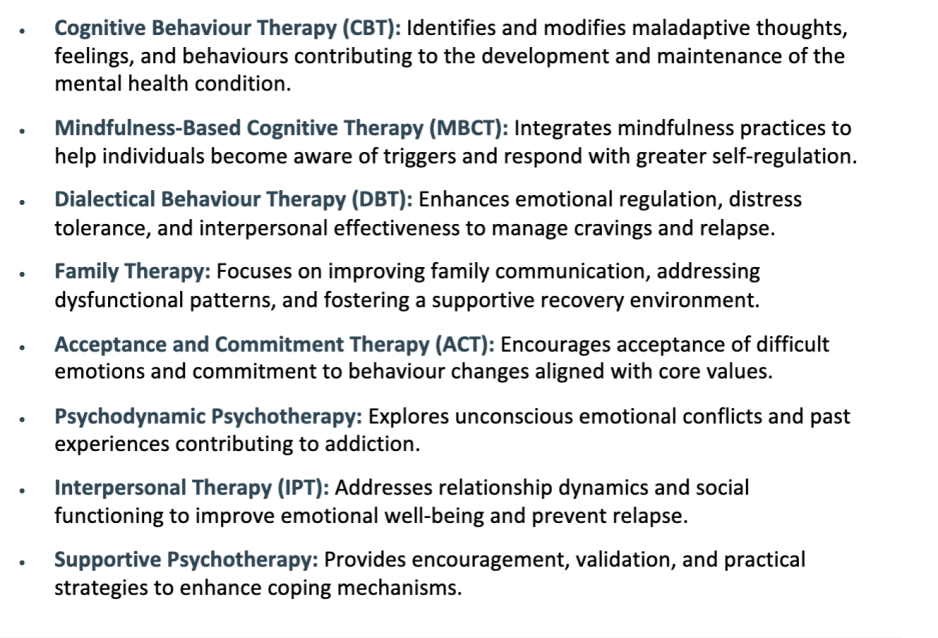
Main types of psychotherapy
The Second Wave of CBT
The Second Wave represents the dominant model in clinical psychology. It focuses on how our thoughts influence our emotions and actions.
Aaron Beck’s Cognitive Model
Core Beliefs: Deeply held, latent negative views about yourself, others, and the future, such as "I am a failure."
Intermediate Beliefs: Negative assumptions formatted as "If... then" statements.
Automatic Thoughts: Immediate, biased cognitive responses like catastrophizing or black-and-white thinking.
Outcome: These cognitive layers lead directly to maladaptive or unhelpful behaviors.
Clinical Application of Second Wave CBT
CBT is a short-term, goal-oriented treatment. It typically lasts between three and six months.
Treatment Focus
Mechanisms: Changing unhelpful thinking and behavioral patterns.
Cognitive Techniques: Cognitive restructuring to challenge biases.
Behavioral Techniques: Exposure therapy and behavioral experiments.
Model: A disease-centered approach focused on reducing specific symptoms and pathology.
The Third Wave Transition
The Third Wave marks a shift from what people think to how they think. This process-based approach integrates humanistic, existential, and spiritual traditions.
Core Philosophy
Holistic View: Moves away from the deficit model toward promoting personal values and wellbeing.
Key Pillars: Mindfulness, metacognition, and personal goals.
Symptom Reduction: Viewed as a secondary benefit rather than the primary goal.
Acceptance and Commitment Therapy (ACT)
The goal of ACT is to maximize your potential for a rich and meaningful life through psychological flexibility.
Key Strategies
Mindfulness: Teaching skills to stay present and detached from unhelpful thoughts.
Value Clarification: Identifying what truly matters to you.
Committed Action: Using your values to motivate and guide behavioral change for the better.
Dialectical Behavior Therapy (DBT)
DBT centers on the dialectic, which is the synthesis of two opposing forces: acceptance and change.
DBT Objectives
The Balance: Accepting your current life and self while simultaneously working to change behaviors that cause suffering.
Enhancement: Improving emotional, cognitive, and interpersonal responses.
DBT Core Skills
DBT utilizes four specific behavioral skills modules divided into two categories.
Acceptance Skills
Mindfulness: Being present in the moment.
Distress Tolerance: Coping with crises without making them worse.
Change Skills
Emotion Regulation: Managing and shifting intense feelings.
Interpersonal Effectiveness: Navigating relationships and communicating needs clearly.
Psychotherapy Delivery and Ethics
Effective therapy requires tailoring components to the individual. Applying the same treatment to every patient is considered inappropriate and potentially unethical.
Professional Standards
Customization: Different clients require different relationship styles and treatment plans.
Accreditation: Clinical training programs must include evidence-based therapies to maintain their certified status.