Unit 6: Hematolgical Disorders; DIC & HIT
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
hematopoiesis
blood cell formation
stem cell differentiate
erythrocytes
leukocytes
thrombocytes
blood contains
plasma (clotting factors floating, liver producers)
solutes
serum proteins
coags
healing transport
osmotic pressure
blood cells
where are globulins made
liver
what’s the main protein in blood
albumin, made in liver
what can happen with decreased proteins
third spacing
erythrocytes/RBC’s
purpose: O2 transport
production stimulated by: EPO
maturation: 4-5 days
lifespan: 120 days
normal: 4.2-5.15
decreases with: renal disease
thrombocytes/platelets
purpose:clotting
production stimulated by: thrombopoietin
maturation: 2/3 circulate in blood, 1/3 in spleen
lifespan: 8-12 days
normal: 150-400k
decreased with: used more rapidly if multiple vascular injuries or clotting stimuli
leukocytes/WBC
purpose: fight infection and antigens
production stimulated by: triggering mechanism within the immune response
maturation: varies
lifespan: varies
normal: 4500-11,000
decreased with: malnutrition, immune disorders, advanced age
CBC with diff includes
basophils
eosinophils
neutrophils
monocytes
B and T lymphocytes
hemostasis
platelets
blood proteins
vasculature
balance between clotting system and fibrinolytic system
clotting cascade steps
vasoconstriction
plts get sticky —> activation —> platelet plug
2A. fibrin = cement, intrinsic & extrinsic meet at the common pathway (Factor X) —> thrombin —> fibrin
what needs to work in order for clotting factors to work
liver
calcium
what is Factor X
the common pathway
can get anti factor XA lab test
where the intrinsic and extrinsic pathway meeet
all other anticoagulants work here !!!! besides the heparin and warfarin
anti platelets do what
makes plts less sticky
antiplt meds
pt plug inhibitors
ASA
clopidogrel
ticagrelor
antiplatelet meds MOA
block plt aggregation —> prevents CLOT FORMATION
works on the plt phase —> primary hemostasis
anticoagulants do what
work on the production of fibrin
clotting cascade inhibitor
anticoagulant meds
heparin
warfarin
heparin works on the
intrinsic pathway
injury’s INSIDE the vessel/ to the blood
heparin antidote
protamine sulfate
heparin lab to monitor
aPTT
aPTT normal range and therapeutic range
normal: 25-3 seconds
therapeutic: 1.5-2.5 the normal, so 60-80 seconds
warfarin works on the
extrinsic pathway
tissue injury OUTSIDE the vessel
needs Vitamin K dependent factors
warfarin antidote
vitamin K
warfarin labs to monitor
PT
INR
INR normals and therapeutic range
normal: 1
therapeutic: 2-3
hemostasis summary
activation of the coagulation cascade
formulation of a stable fibrin clot
activation of fibrinolytic system
blood clots
stop bleeding from injured vessel
3 physiologic mechanisms known to trigger clotting
tissue injury ‘
vessel injury
FBO in bloodstream
fibrinolysis
stimulated by clot formation & occurs 1-3 days after clot formation
plasmin- an enzyme that digests fibrinogen & fibrin
when plasmin digests fibrinogen—> fragments are produced that function as potent ANTICOAGULANTS
form FIBRIN DEGREDATION PRODUCTS (FDP’s)/ Fibrin split products (FSP’s) —> bleeding —> CAN LEAD TO DIC
coagulation pathway
cascade theory
initiating event
intrinsic pathway: injury to blood (factor XII (12)
extrinsic pathway: tissue injury (factor VII (7)
final common pathway
prothrombin —> thrombin
fibrinogen —> fibrin
CLOT
fibrinolysis continued
Stimulated by clot formation
Thrombin released
Stimulates conversion of plasminogen to plasmin
Breakdown yields fibrin degradation products
(FDPs), or fibrinogen split products (FSPs)
cues to heme and immune problems
altered O2
bleeding
infection
heme dx tests
CBC with diff
coagulation profile
based on these findings, further testing math be required
bleeding disorders
Abnormality in stages of clotting
Vasoconstriction
Creation of platelet plug
Development of clot
Fibrinolysis
Inherited or acquired
Common in renal, hepatic, and gastrointestinal
disorders; malnutrition
D dimer indicates what
clot breaking down
dx of bleeding
CBC
H&H
Fibrinogen
FSP/FDP
D Dimer
PT, aPTT
nursing managment of bleeding
Assess blood loss
Assess vital signs, hemodynamics, and
perfusion
Assess for signs and symptoms of hypovolemia
Administer blood products and fluids
Administer topical agents as needed
what can we given for prolonged clotting factors
FFP
medical management of bleeding
Whole blood
Packed RBCs
Leukocyte-poor RBCs
Platelets
Cryoprecipitate
• Albumin
• Granulocytes
• Plasma protein
• Fresh frozen plasma
whole blood
what is it: RBC’s, plasma, clotting factors
why do we give: restores O2 carrying capacity and intravascular volume
indications: SEVERE hemorrhage, symptomatic anemia with major circulating volume deficit
PRBC’s
what is it: RBC’s spun out from whole blood (leukoreduced)
give why: restores O2 carrying capacity and intravascular volume
indications: symptomatic anemia, acute hemorrhage
based of H&H <7 or active bleed
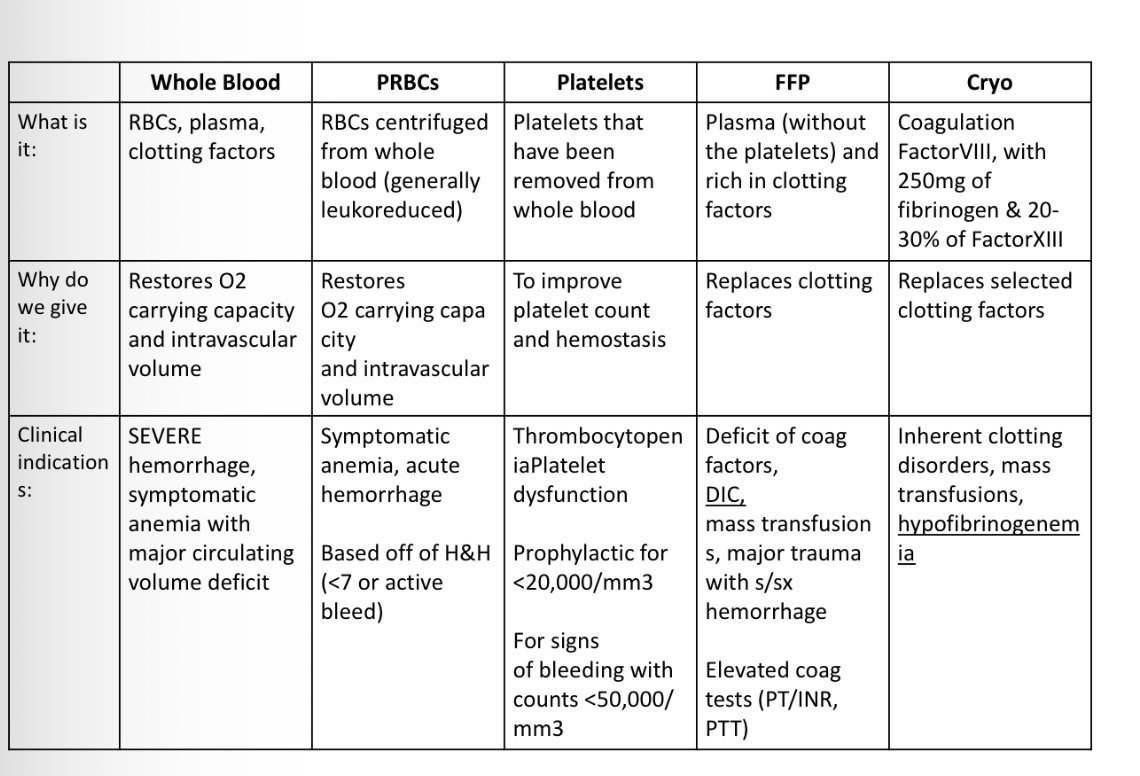
platelets
what is it: plts thatve been removed from blood
why we give: improve plt count and hemostasis
indications: prophylactic for <20K and for signs of bleeding with counts <50K
FFP
what is it: plasma w/o platelets and RICH IN CLOTTING FACTORS
why we give: replaces clotting factors
indications:
deficit of coag factors
mass transfuions
DIC
major trauma with s/s of hemorrhage
elevated/prolonged PT/INR/PTT
Cryo
what is it: coagulation factor VIII (8), with 250 mg fibrinogen and 20-30% of factor XIII (13)
why we give: replaced selected clotting factors i
indications:
inherent clotting disorders (hemophilia)
mass transfusions
hypofibrinogenemia
DIC
disseminated intravascular coagulation
Accelerated activation of clotting cascade
Depletion of clotting factors
Bleeding
Secondary problem
bleeding with no perfusion to kidneys and brain
what is DIC cont
hematological disorder that occurs because of an acceleration in the clotting cascade. A triggering event causes the release of procoagulant factors such as: sepsis , trauma, big hemorrhage
In other words -
It’s a coagulopathy in which you have both
intravascular clotting and bleeding
patho of DIC
Initiating event: procoagulants
Stimulation of intrinsic or extrinsic pathway
Clots in microvasculature
Consumption of clotting factors (eating up clotting factors —> microemboli = consumptive couagulopathy
Fibrinolysis
FDPs: potent anticoagulants
DOC etiology
Infection
Trauma (e.g., burns, crush)
Obstetric conditions (e.g., abruptio placentae,
amniotic fluid embolus, retained dead fetus, PPH)
Hematological disorders
Oncological disorders
Other: shock or sepsis, acute respiratory
distress syndrome
blood is an organ —> DIC = failure of organ
1st phase of DIC
thrombotic
last hours to days
large amounts of thrombin are produced and clots are lodged in the micro vasculature
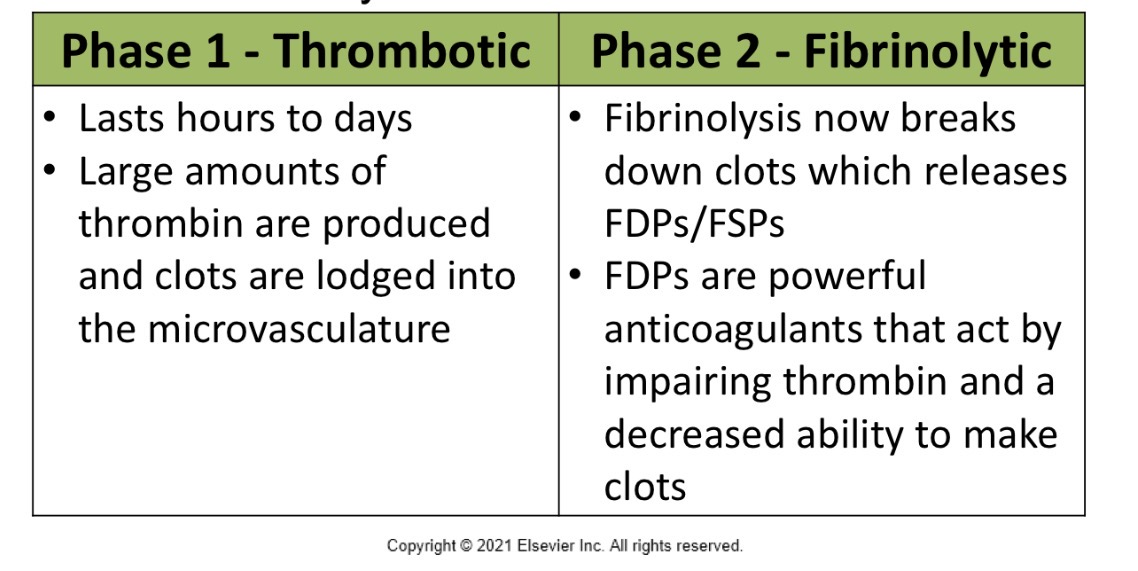
2nd phase of DIC
fibrinolytic
fibrinolysis now breaks down clots which releases FDP’s/FSP’s
FDP’s are potent anticoagulants that act by impairing thrombin and decreased ability to make clots
DIC summary
Triggering event (endothelial damage or direct tissue damage)
Activation of clotting cascade
Excessive thrombin production leads to fibrin
deposits in the microvasculature (leads to death to
whichever organ is occluded)
Available clotting factors are spent/consumed
Fibrinolysis occurs, leading to FDPs (anticoagulants)
RBCs are damaged as they try to pass blocked capillary beds (more hemolysis)
why is bleeding such a big thing in DIC
anticoagulants are floating around and there are NO CLOTTING FACTORS LEFT= bleeding !!!!
DIC assessment
Overt bleeding or oozing
Occult bleeding
Signs of platelet deficiency
Petechiae
ecchymosis
Decreased perfusion to organs
Changes in mental status
Infarction of tissue in digits and nose (necrosis)
what labs will be decreased with DIC
platelets
fibrinogen
coagulation factors
H&H
labs that will elevated or HIGH with DIC
FSP/FSP
D dimer
labs that will be PROLONGED (elevated/high) with DIC
PTT
PT/INR
normal INR is 1
thrombin
DIC tx
CORRECT THE UNDERLYING CAUSE
Administer blood and components
Platelets
Fresh frozen plasma
Cryoprecipitate
Packed RBCs
Stop abnormal coagulation
Heparin: controversial when experiencing more hemorrhage than thrombosis
why may we give heparin in DIC
prevents thrombin and fibrin formation —> stops it from getting broken down in the first place
don’t give to active bleeding
overall prevents new from forming, overall less clot breakdown happens overall
stopping the unwanted clotting and control bleeding
Platelets
Highest priority
Fresh Frozen Plasma (FFP)
For Fibrinogen replacement
Contains all clotting factors and antithrombin III
Cryoprecipitate
When plasma is frozen, Factor VIII is inactivated so you'll need to replace through cryoprecipitate
PRBCs
To replace losses
FFP + Cryo for DIC
other tx for DIC
Tranexamic acid TXA, (anti-fibrinolytic)-for extreme hemorrhage, but causes thrombotic events (MI and renal artery occlusion)-should be used with Heparin —> prevents plasmin from breaking down fibrin
Antithrombin III (inhibits thrombin, factor Xa, common pathway)-
prevents development of fibrin clot.
prevents more fibrin production in the 1st place
heparin
a Thrombin Inhibitor
• Thought is to block the clotting process
• Controversial (might work or make bleeding
worse)
antithrombin III
Synthetic Antithrombin III inhibits thrombin
• May shorten course of DIC and improve survival
rates
transexamic acid
• Inhibits fibrinolysis by interfering with plasmin activity
• For severe hemorrhage with DIC
• Risk thrombotic events-MI and renal
artery occlusion
nursing managment of DIC
Assess and prevent
Conduct frequent laboratory analysis
Administer blood products
Assess circulation
Oral care and skin care
Relieve pain
Assess for complications: shock, multisystem
organ failure, impaired circulation
prevent and treat hypothermia
Keep pt covered during transfusion
Warmed blankets and/or Bair Hugger as needed
Utilization of fluid warmers or a rapid transfuser that provides warming
ionized calcium
Blood transfusions include citrate. It binds to calcium in the patient’s blood causing hypocalcemia (tetany, laryngospasm)
Chvosteks & Trousseaus
Follow up CBC and DIC panel
multiple blood transfusions can cause low Ca+
citrate builds up with multiple transfusions and lowers Ca+, checking the ionized shows the free floating ca in blood and gives more accurate levels
thrombocytopenia
Decreased platelets
Less than 100,000/microliter
Risk for bleeding
Treated with platelet transfusions
HIT
heparin induced thrombocytopenia
side effect
what is HIT
Can occur (as a delayed onset) even after
heparin discontinuation
HIT type 1
Type 1-non-immune, direct effect of Heparin on platelets-DC the Heparin immediately
pH will increase when Heparin is stopped
directly damages the platelets
HIT type 2
immune mediated and has life and limb
threatening thrombotic complications
platelets start clumping together
plts attacked, stopping the Heparin doesn’t help
HIT type 2 continued
HIT is an immune response to Heparin
Usually occurs 5-10 days after receiving heparin therapy
The immune response causes a >50% decrease of the highest platelet count after
heparin started.
examples: platelets before starting Heparin 300,000. five days later after therpay was started plts count now at 140,000.
just find half of the OG lab level, if less than or equal to that it’s HIT type2
HIT etiology
Heparin binds to platelets, specifically Platelet
Factor 4 (PF4)
This forms an antigenic complex on the surface of the platelets
Some people develop an antibody to this
If your body develops an antibody, it means
your body sees your platelets as foreign (seen more with Enoxaparin)
Macrophages begin to eat platelets
risk factors for HIT
10-fold higher with unfractionated heparin v.
LMWH (Lovenox)
Major Surgery
HIT complications
HYPERCOAGULABILITY (more with Type 2 HIT) & THROMBOSIS as opposed to bleeding, even though platelet count is low
WILL ACTUALLY CLOT MORE even though plts are low, not a bleeding risk
start clumping like crazy together, so count drops overall becuase they’re being used up in clots and consumed not becuase of BLEEDING!!!
thromboembolic complications of HIT
DVT
PE
MI
CVS (stroke)
arterial occlusion
DIC maybe
HIT Dx
A 50% decrease ( 300,000 —> 150, 000) from the highest level after heparin is started AND –a new thrombus OR – an anaphylactoid reaction after a heparin bolus
withdraw heparin
HIT treatment
Discontinue ALL Heparin
Administer meds that inhibit thrombin formation or cause direct thrombin inhibition
Argatroban (Novastan)
Bivalirudin (Angiomax)
Warfarin, LMWH, Aminocaproic acid, and
platelets are AVOIDED
Can exacerbate thrombosis
blood product administration
As needed
PRBCs
Symptomatic anemia
Platelets
Thrombocytopenia
• With signs of bleeding or counts low enough for spontaneous bleed with a sneeze
meds that are thrombolytics/fibrinolytics (plasminogen activators)
known as clot busters “-ase”
atleplase
stretokinase
meds that work on the common pathway
rivroxaban
dabigatran
apixaban
enoxaparin
endoxaban
fondaparinux
when do you when to make the switch from Heparin to Warfarin
pt will be on a heparin drip
will start Warfarin PO at the same time
wont d/c the Heparin drip til Warfarin reaches therapeutic level INR of 2-3
what do you for all types of blood transfusion reactions
STOP THE INFUSION
aspirate any blood left in the line, dont want any more going into the patient and then flush with NS
send back to blood bank
get VS
notify the MD
get and type and screen
and tx the type of transfusion reaction (ex: febrile give antipyretics, support the s/s)
acute hemolytic reaction
most dangerous
cause: ABO incompatibility —> wrong blood
onset is immediate
can lead to shock, DIC, KF
acute hemolytic reaction s/s
fever and chills
LOWER BACK PAIN/FLANK PAIN
chest tightness
hypotension
tachy
dark urine
impending doom feeling
febrile nonhemolytic reaction
most common
cause: WBC in donor blood → immune response
onset: within a few hours
febrile non hemolytic reaction s/s
FEVER
chills
headache
malaise
no hemolysis→ not life threatening
allergic reaction blood transfusion
sensitivity to donor plasma proteins
onset: during transfusion
allergic reaction transfusion s/s
ITCHING
hives
flushing
anaphylactic reaction
severe allergy from hypersensitive often IgA
onset is immediate
will see airway swelling
wheezing
dyspnea
hypotension
shock
life threatening
circulatory overload reaction
too much volume too fast
occurs during or shortly after
s/s include→ HTN, JVD, crackles, dyspnea, pulmonary edema
with what blood product do you see more reactions with
FFP