CC3 - Types and Degrees of Hearing Loss
1/92
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
93 Terms
Type of Hearing Loss
Determined by comparing air conduction thresholds to bone conduction thresholds for each ear independently
Four types of hearing loss
Conductive
Sensorineural
Mixed
Auditory processing disorders
Sudden HL
Rapid onset
Gradual HL
Hearing loss occurs in small degrees
Temporary HL
Short duration/reversible
Permanent HL
Not reversible
Progressive HL
Hearing loss will advance in degrees
AU
Both ears
AS
Left ear
AD
Right ear
Monaurally
1 ear
Binaural
Both ears
Flat
Less than a 5dB rise/fall per octave
Gradually sloping
5-12 dB decrease per octave
Sharply sloping
13 or more dB decrease per octave
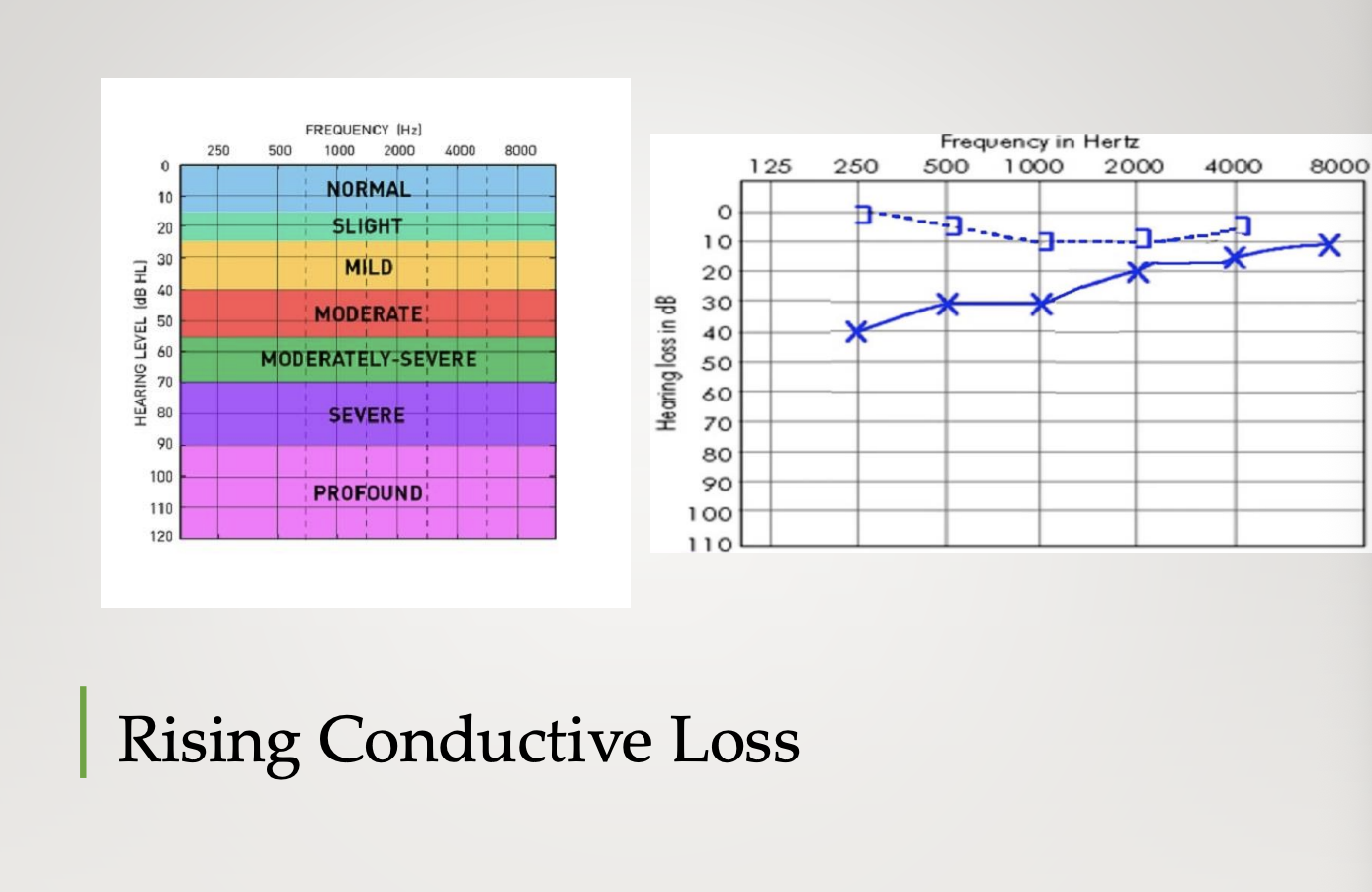
Rising
Low frequency are poorer than high frequency
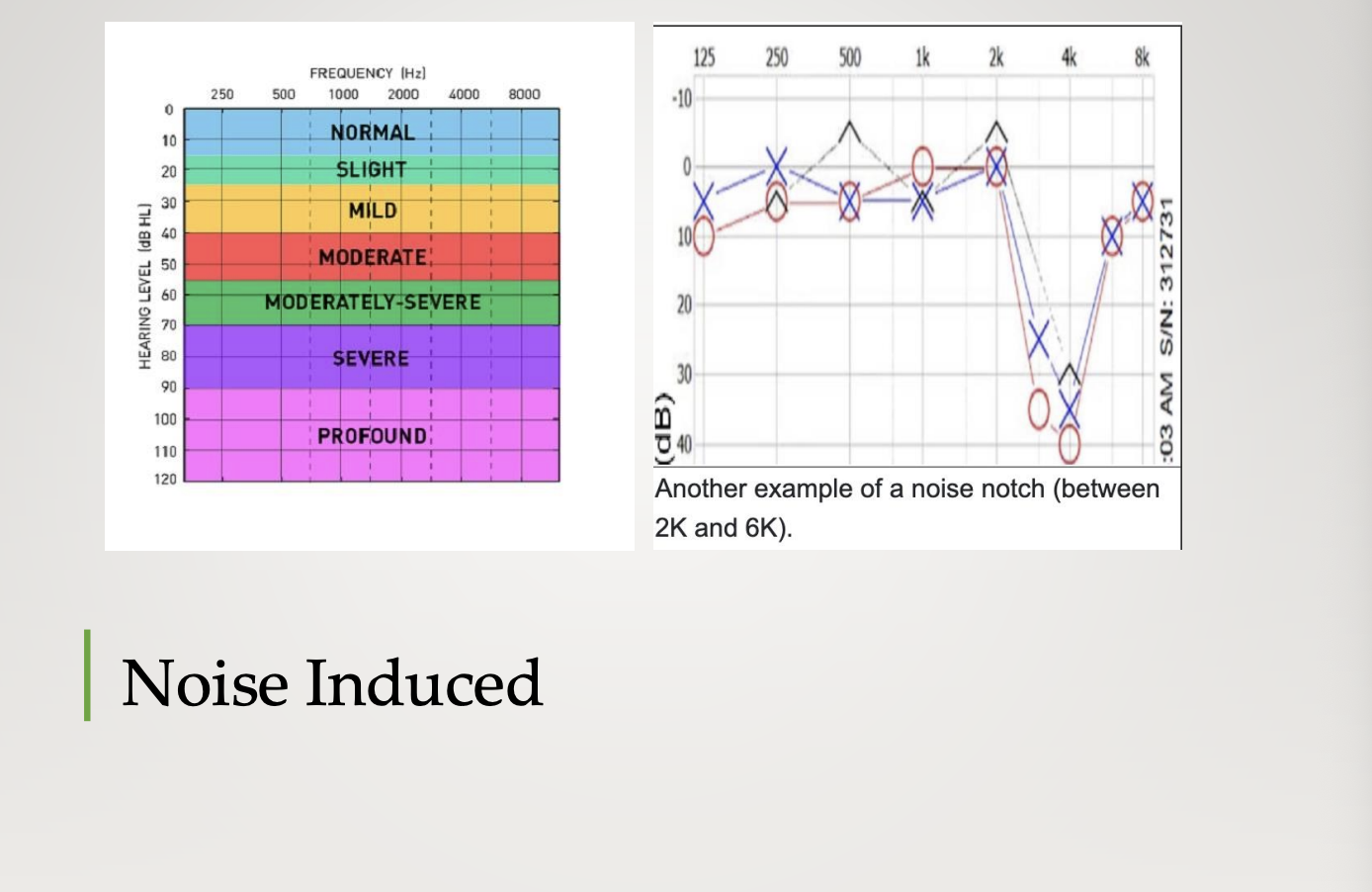
Noice notch
normal haring until 4000 Hz then a decrease
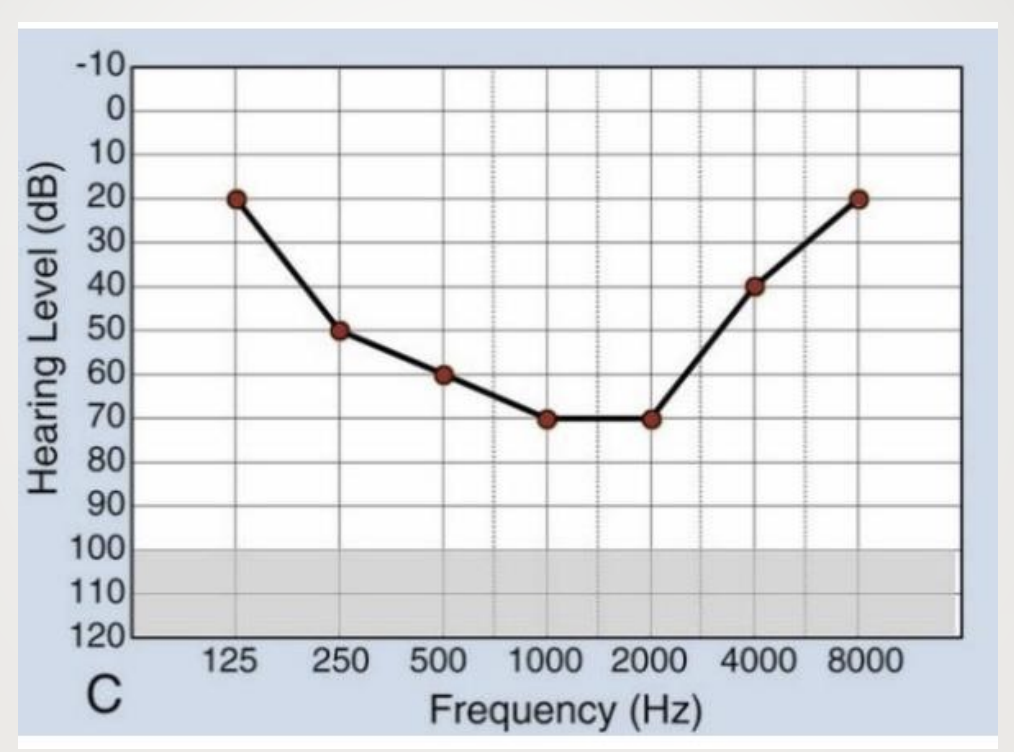
Cookie Bite Audiogram
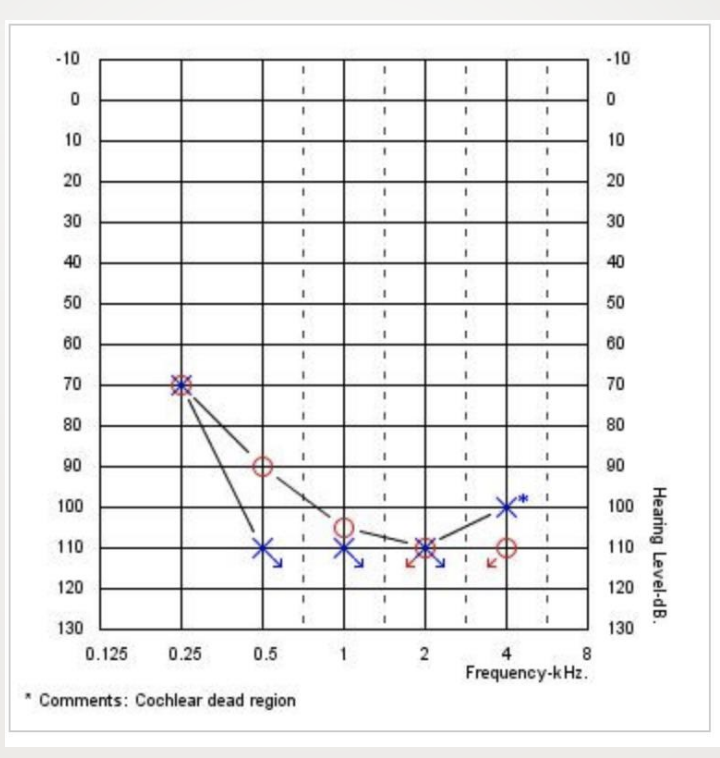
L Corner Audiogram
Hearing loss is described in terms of
type
degree
symmetry
configuration
time of onset (time course)
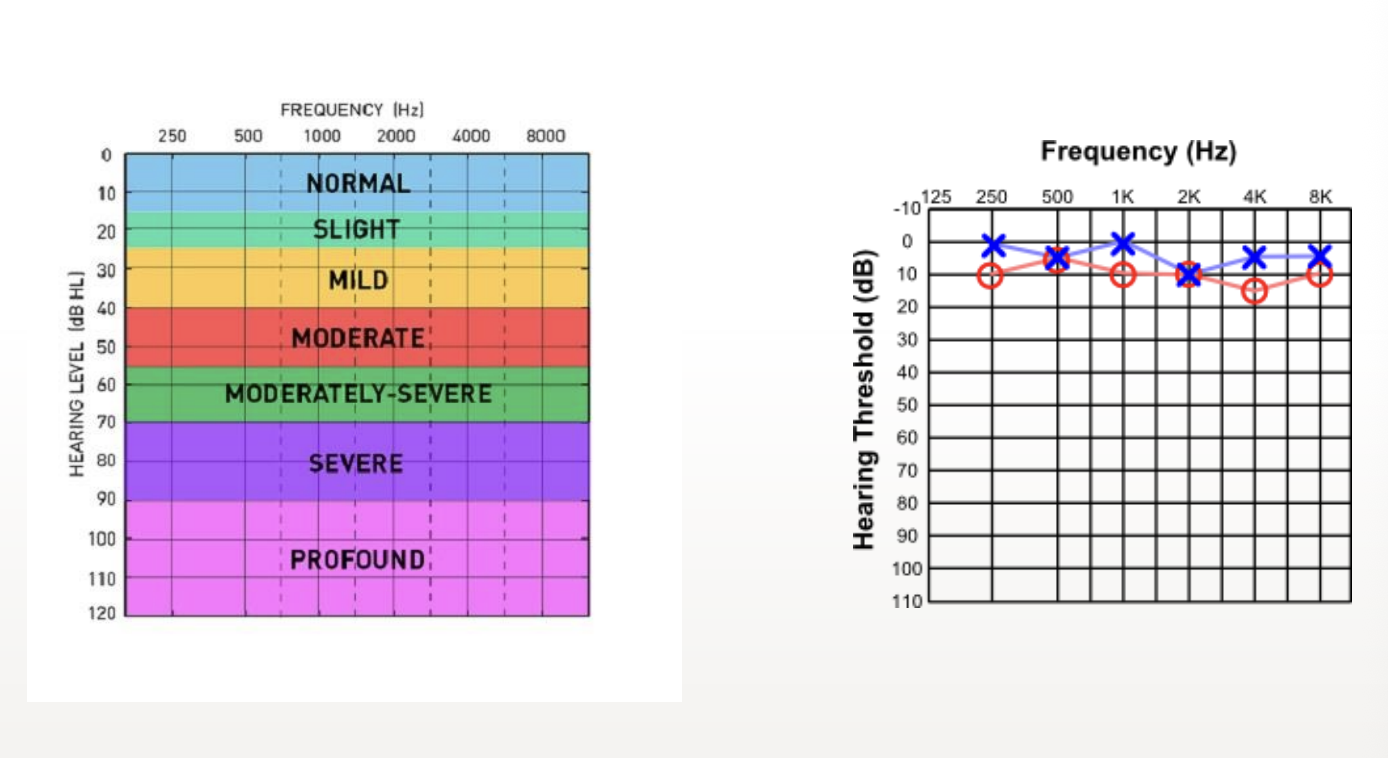
Normal Audiogram
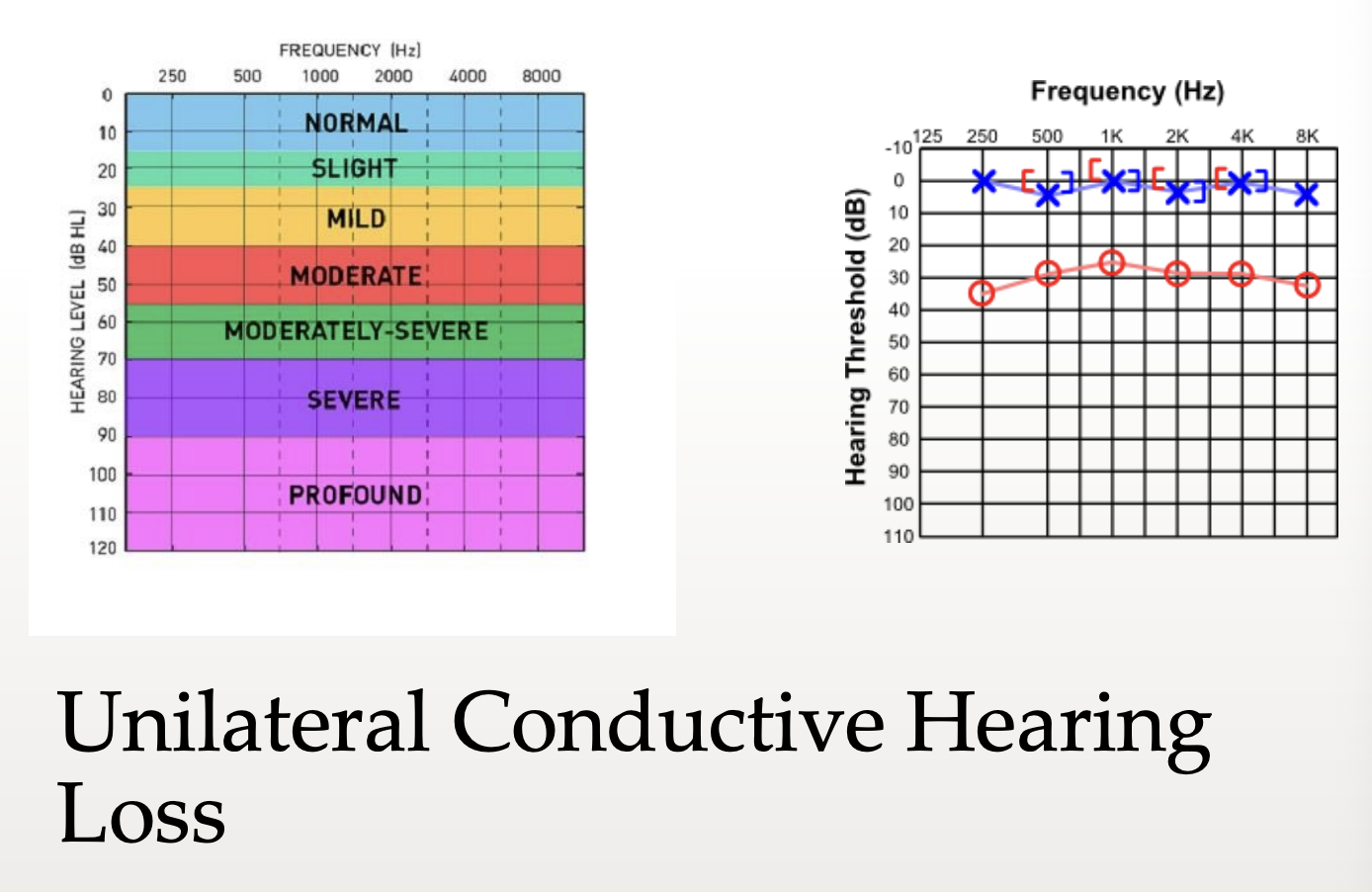
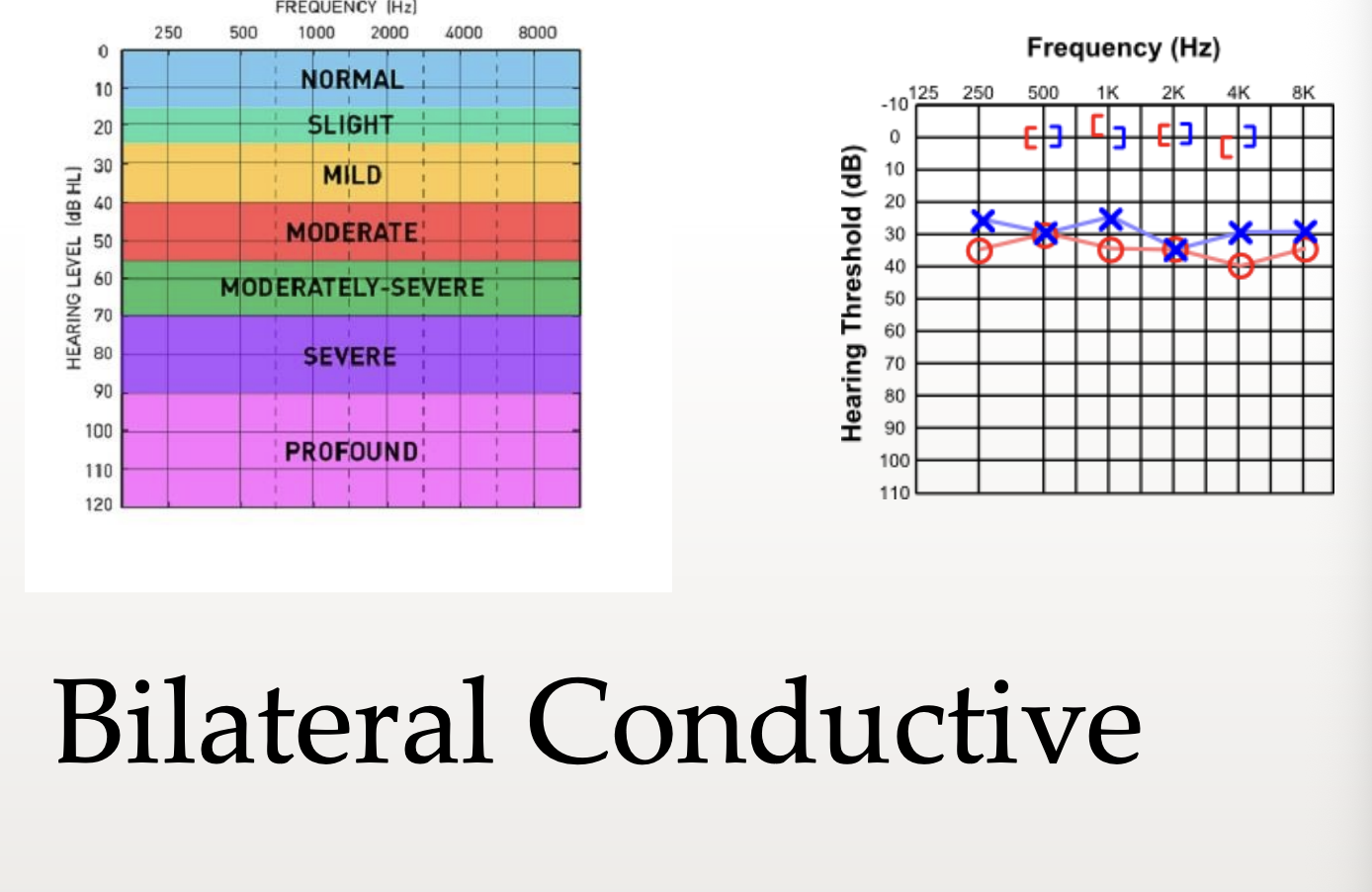
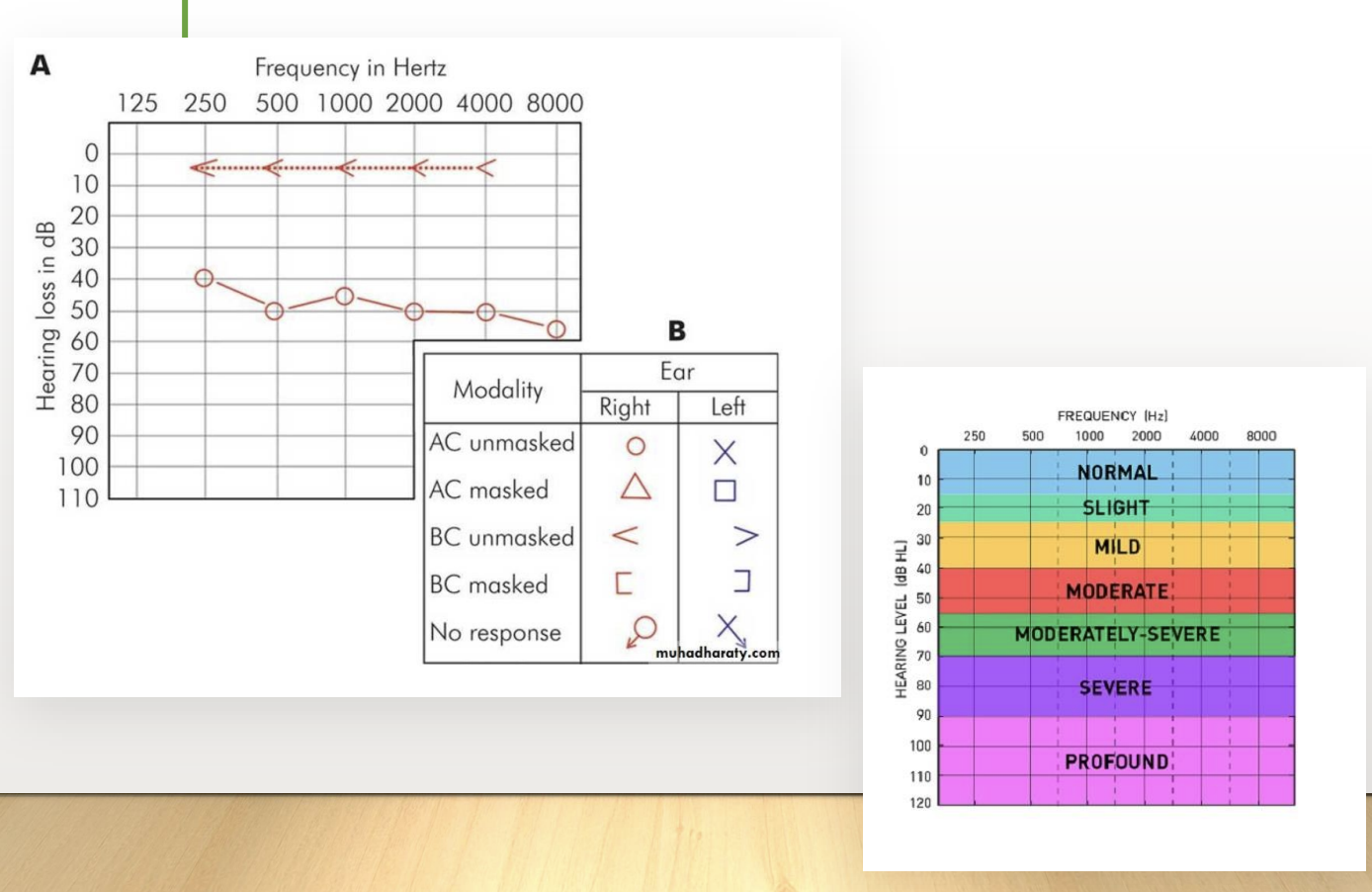
Conductive hearing loss (CHL)
Involves obstruction of outer and middle ear mechanisms
Characterized by bone conduction thresholds within normal range (0-20 dB HL) with higher air conduction thresholds (greater than 20 dB HL)
Can cause occlusion effect = person usually speaks in a quieter voice than normal because they perceive it louder than what it actually is
Opposite of Lombard effect
Audiogram is characterized by flat configuration of low frequency loss and patient may have occasional tinnitus
CHL
Loss can be overcome if the signal is loud enough because there is no problem with the cochlea
If amplified = speech discrimination is not impaired
Paracusis Willisii
Ability to hear better in noisy environments
Unilateral Conductive Hearing Loss
Bilateral Conductive
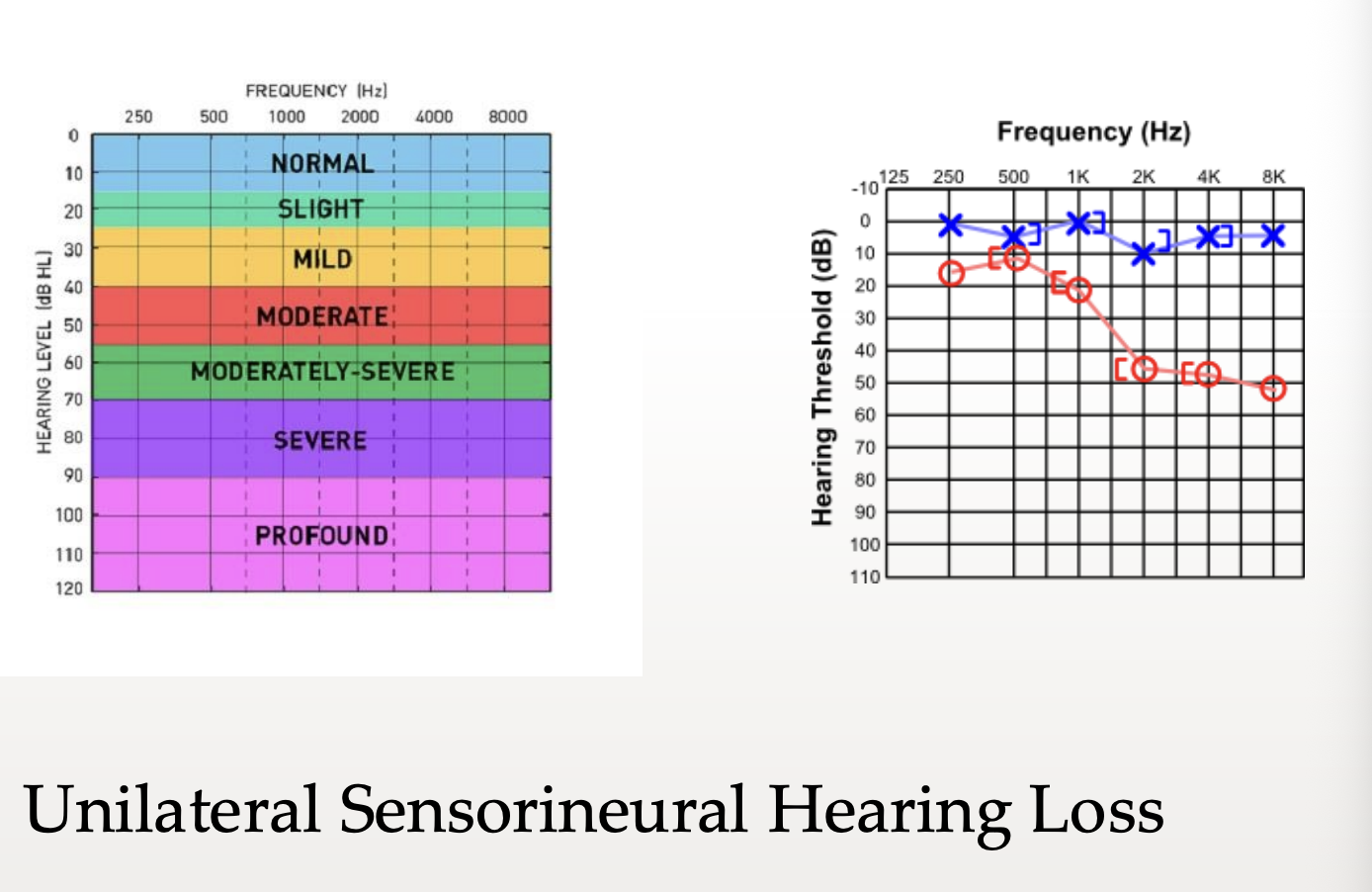
Sensorineural Hearing Loss (SNHL)
Involves the pathology of the inner ear
Two types
Sensory hearing loss = result of damage to the cochlea
Neural loss = damage to 8th nerve
Audiogram = sloping air conduction and bone conduction thresholds are essentially equal (i.e., within 10 dB)
All thresholds outside the normal range
Continued reduction of speech recognition ability even with adequate amplification
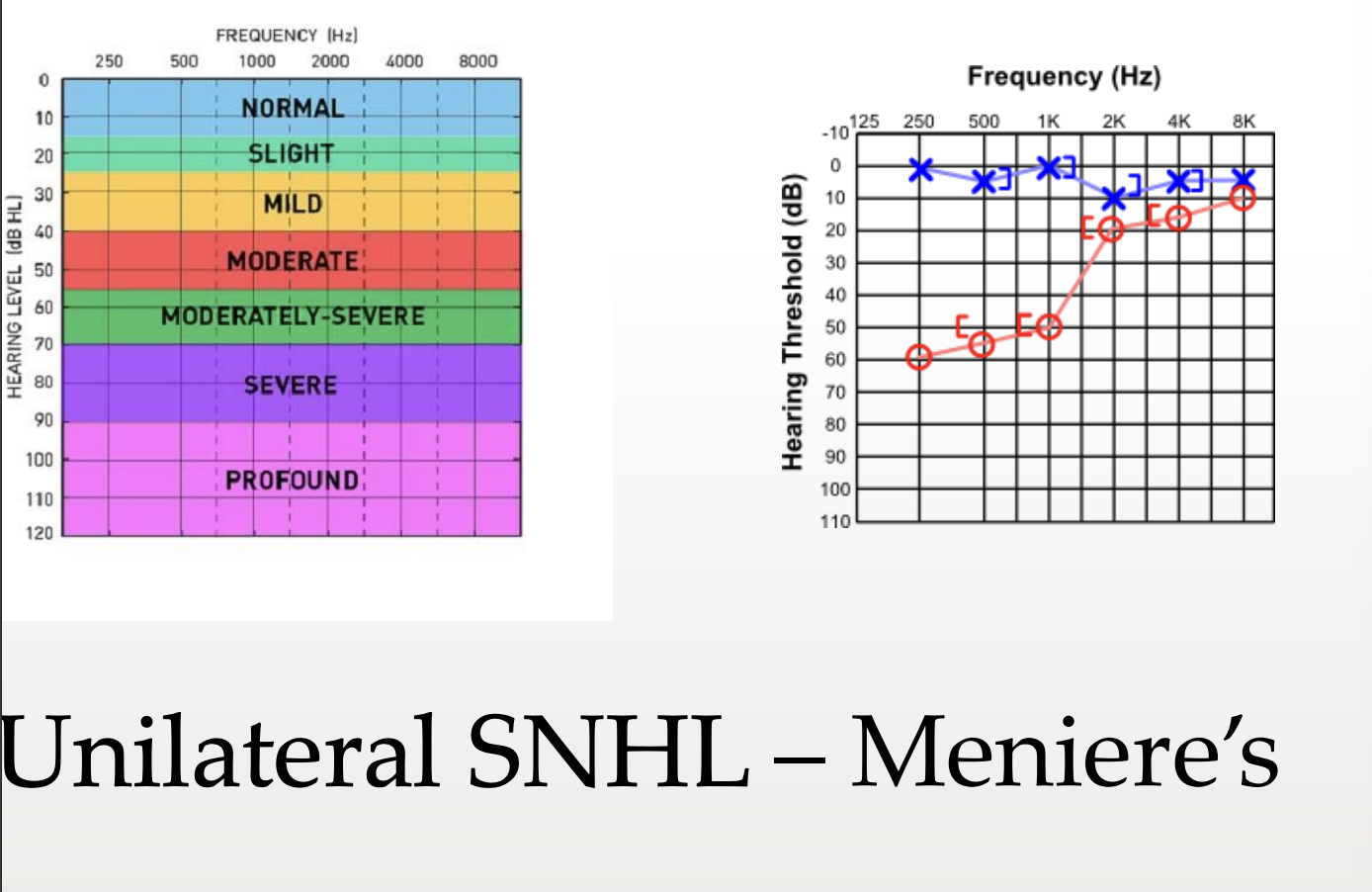
May have tinnitus, especially with Meniere’s
Recruitment = cochlear phenomenon where there is a nonlinear increase in loudness growth, wherein loudness grows rapidly at intensity levels just above thresholds but may grow normally at higher levels
Indication of retrocochlear pathology
May have diplacusis = where one tone sounds like 2 different pitches in two ears, and is an indication of retrocochlear disease
Patient will speak excessively loudly since the patient can’t monitor himself
Sensory Hearing Loss
Damage of cochlea
Someone who has sensory hearing loss (SNHL) presents with
Recruitment
Reduction in frequency resolution (impacts speech understanding)
Reduced dynamic range
Word recognition ability is reduced
Neural Hearing Loss
Damage of VN 8 (vestibulocochlear)
Someone who has neural hearing loss (SNHL) presents with
Word recognition ability is poorer than expected based on hearing loss severity
Speech recognition declines with increases in intensity (rollover phenomenon)
Auditory adaptation occurs
Unilateral Sensorineural Hearing Loss
Unilateral SNHL - Meniere’s
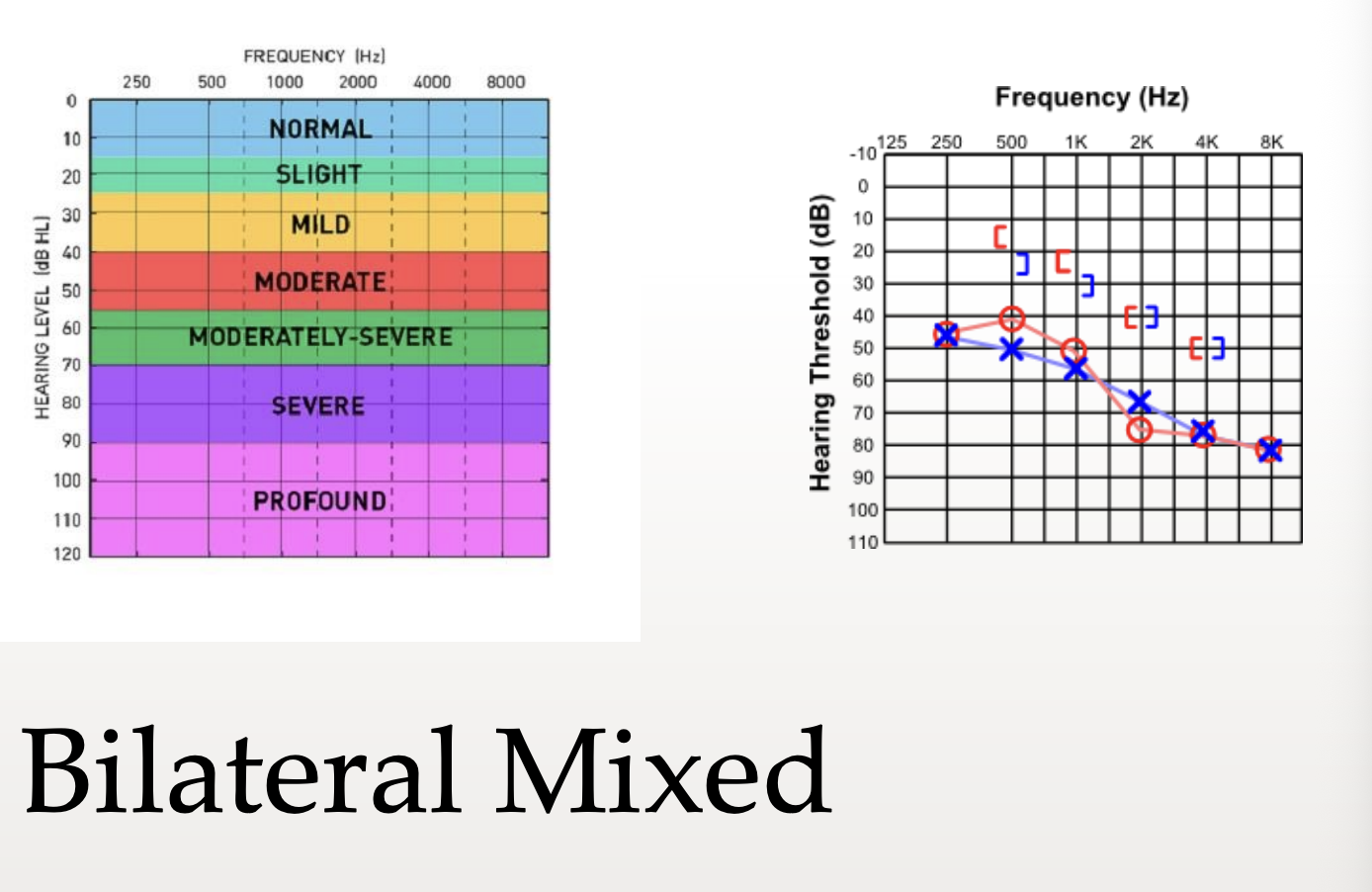
Mixed Hearing Loss
Result of both OE/ME and IE pathologies
Combination of both CHL and SNHL
Characterized by bone conduction thresholds outside normal hearing range, with air conduction thresholds poorer than bone conduction thresholds
The difference between air and bone conduction thresholds is known as the air-bone gap (ABG)
Reflects degree of conductive component contributing to overall hearing loss
Bilateral Mixed
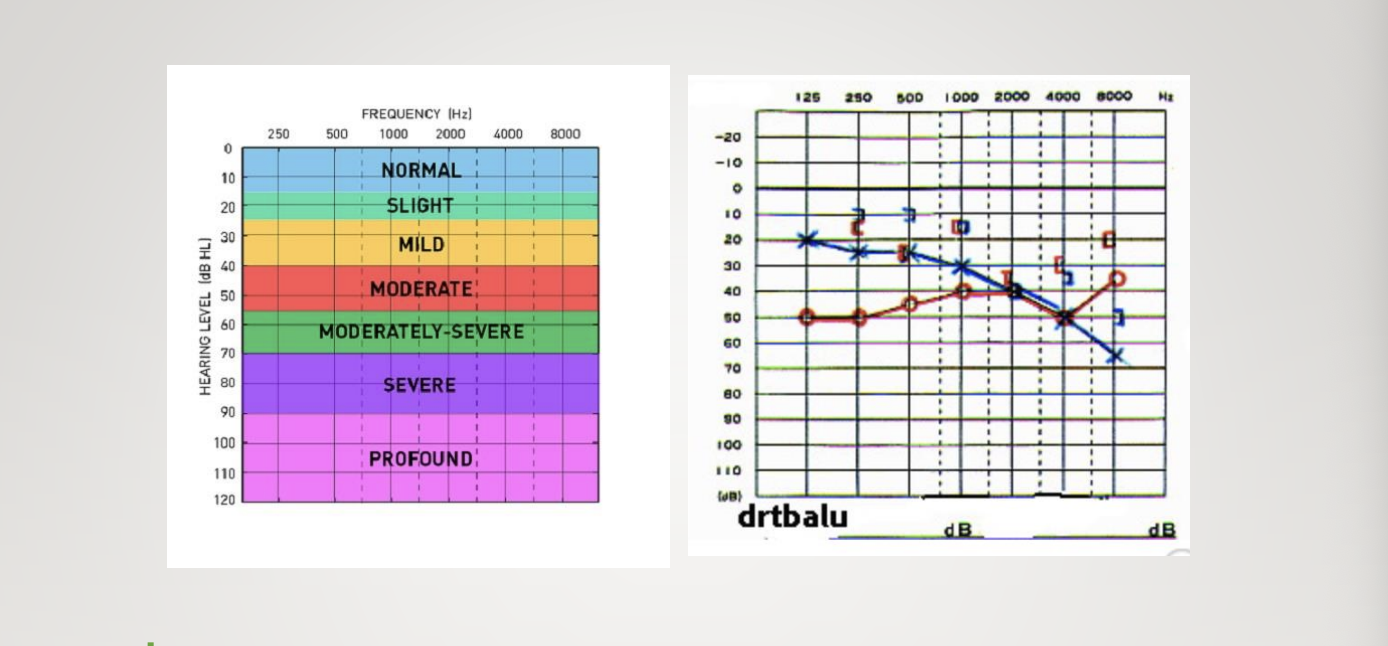
Degree of Hearing Loss
Adults range from mild to severe-profound
Children range from slight to profound
Normal = -10 to 15 dB
Patient hears almost everything well, but may struggle in less than ideal situations (i.e., noise)
Slight = 16 to 25 dB (only in children)
Mild = 26 to 40 dB
Patient may have difficulty understanding speech if it is faint or distant
#1 problem in schools
Moderate = 41 to 55 dB
Listening is strain and he/she often asks for repetition
Moderately-severe = 56 to 70 dB
Severe = 71 to 90 dB
Patient may hear loud voice about 1 foot away from ear
Profound = 91 dB+
Patients will not rely on hearing as primary use of communication
Normal HL
-10 to 15 dB
Slight HL
16 to 25 dB
Mild
26 to 40 dB
Moderate
41 to 55 dB
Moderatley Severe
56 to 70 dB
Severe
71 to 90 dB
Profound
91+ dB
Symmetry
How much right and left ears mirror one another
Configuration
Pattern that describes relationship of low-frequency hearing to high frequency hearing
Asymmetrical Loss
When one hear has loss and other is normal or one ear is much more severe than other
Noise Exposure
Sensorineural notch at 3000 or 4000 Hz
ME Effusions (fluid in ME space)
Rising conductive loss reflects stiffness tilt
Ossicular discontinuity, ME tumor and thickened TM
Sloping conductive loss reflects mass tilt
Otosclerosis
Hardening at footplate of the stapes – Carhart notch
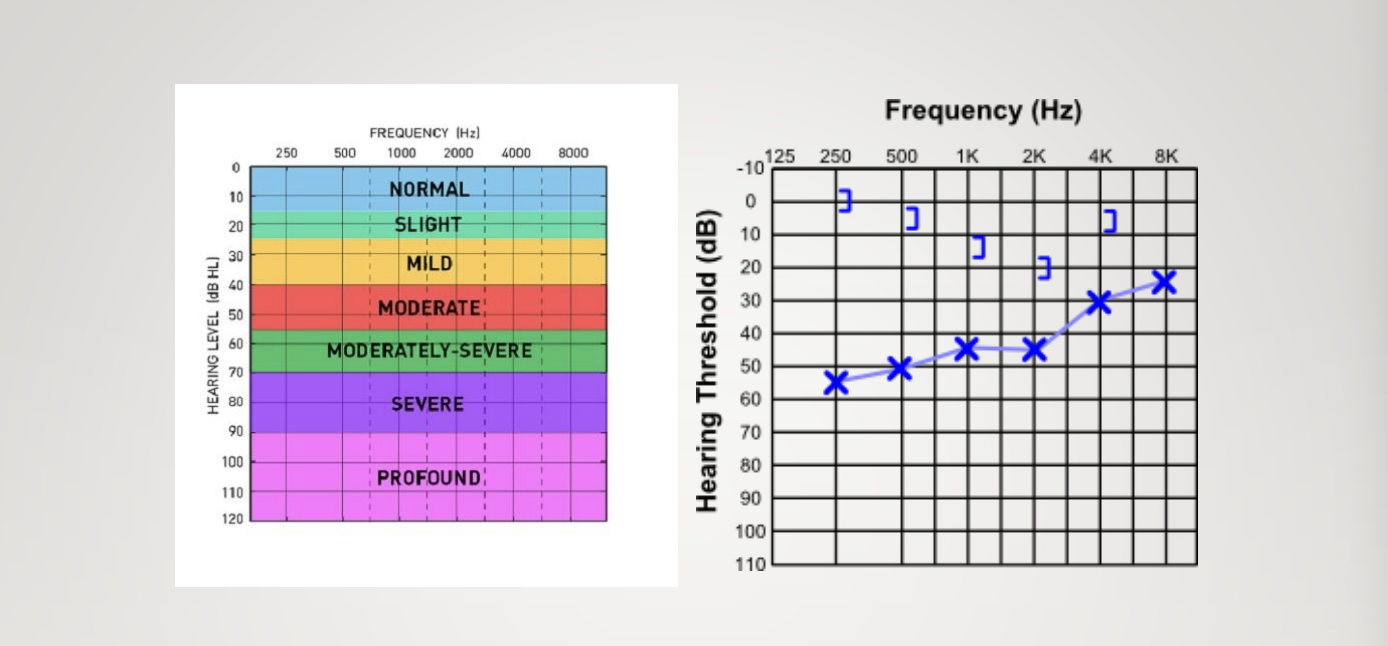
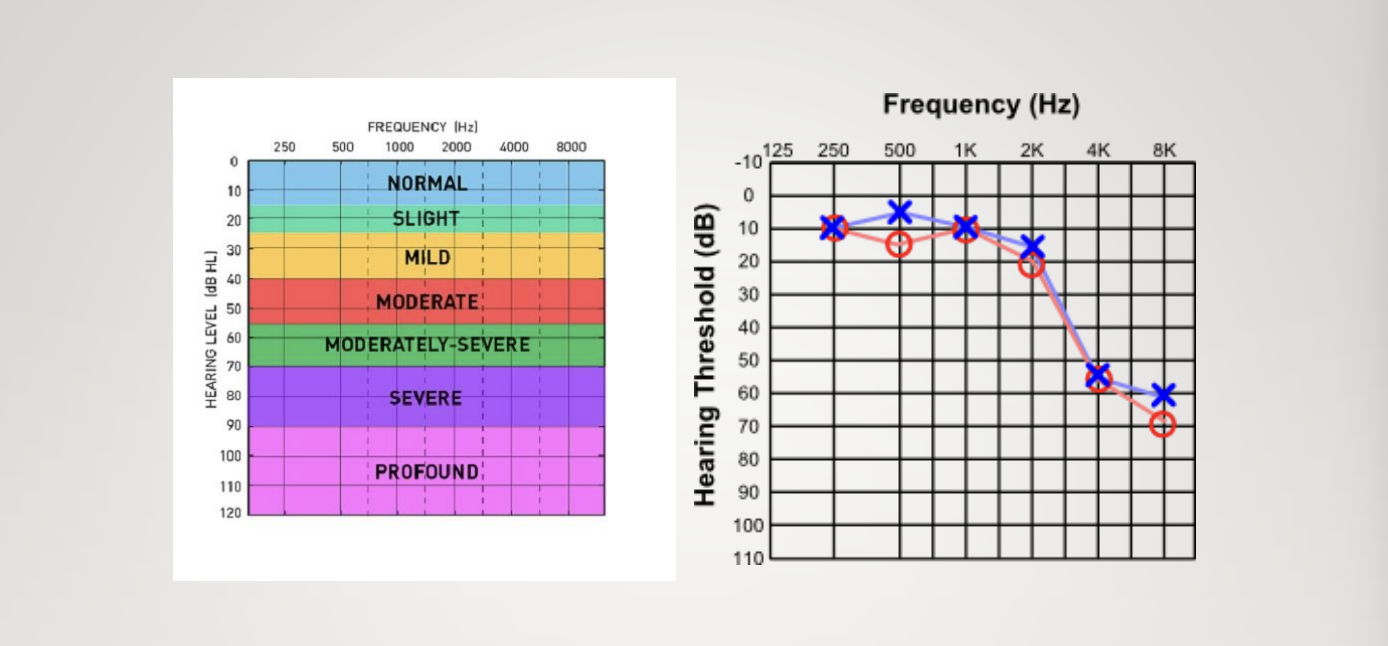
Presbycusis
Age related high frequency hearing loss
Noise Induced
Rising Conductive Loss
Ossicular Discontinuity
Otosclerosis
Carhart’s Notch
Presbycusis
Time of Onset (time course)
Time of onset or time course deals with how long the patient has been experiencing problems
Describe hearing loss as progressive versus stable
Describe it as acute, sudden, or gradual
Malingering
May report functional hearing loss
Also referred to as non-organic hearing loss (NOHL), pseudohypacusis, or psychogenic hearing loss
Intra- and intertest discrepancies that cannot be accounted for
EX: Poor SRT-PTA agreement
Should not exceed 6dB
Patient may only repeat half of the spondee
Absence of shadow curve (greater than 60 dB difference between right and left ears for unmasked air conduction thresholds)
Bone conduction thresholds will be poorer than air conduction thresholds
Most common in boys who are young school age
Malinger to gain attention or to compensate for poor academic performance
Difficult to explain to the parent, so it may be important to ask if anything else was going on when the loss was first noticed
Divorce, a new baby, or a major move
Adults = secondary financial gain
Objective physiologic levels = Stenger test
Two pure tones of equal intensity are presented bilaterally; whichever ear sounds louder, that is the one that responds, and the other ear acts dead.
Pseudohypacusis
Inconsistency in audiometric data
Mainly seen in children
Psychogenic hearing loss
Seen suddenly in girls between the ages of 8 and 12
Loss does not affect school ability or vocal quality
Impact of hearing loss on communication depends on
Degree of sensitivity loss
Audiometric configuration
Type of hearing loss
Degree and nature of speech perception deficits
Auditory Perception
Communication depends on the quality of auditory perception of
Segmentals
Suprasegmentals
Begins before birth
After birth, the process of selective listening extends to speech stimuli within a few weeks
Segmentals
Intensity
Frequency
Duration
Suprasegmentals
rate
rhythm
intonation
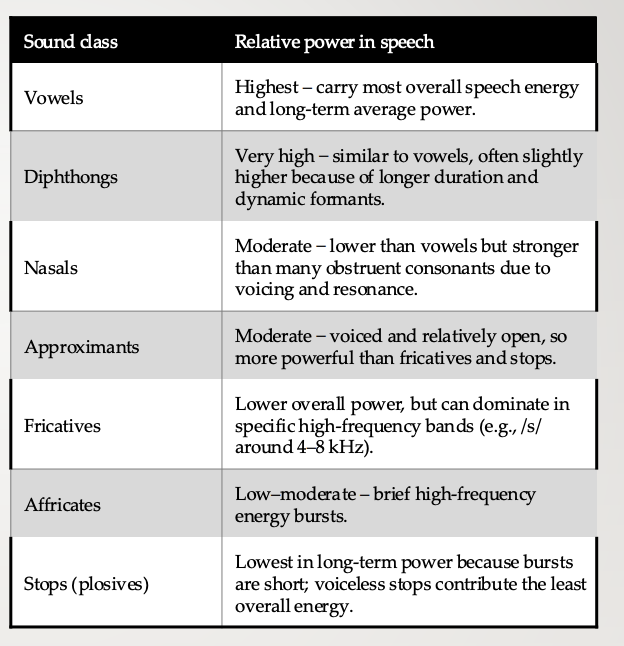
Sound class and relative power in speech
Suprasegmentals
Convey important information, primarily in low frequencies through cues associated with fundamental frequency (e.g., pitch falls or rises at end of utterance)
True or False: Every sound is composed of its own specific acoustical energy (due to the resonance of the vocal tract)
True
True or False: Every sound also has its own relative power (energy, intensity)
True
True or False: Voicing, nasality, duration, and place of articulation are NOT key distinctive features found in speech
False
Perception implies understanding and comprehension NOT
Just reception of speech
Detection
Do you hear the sound, yes or no?
Discrimination
Do the 2 sounds sound the same or different?
Identification
What is that sound?
Attention
Degree/ quality of listener’s attention matters
Memory
Ability to retain or store verbal information
Closure
Bringing speech elements together into a meaningful whole
Comprehension
What does that mean?
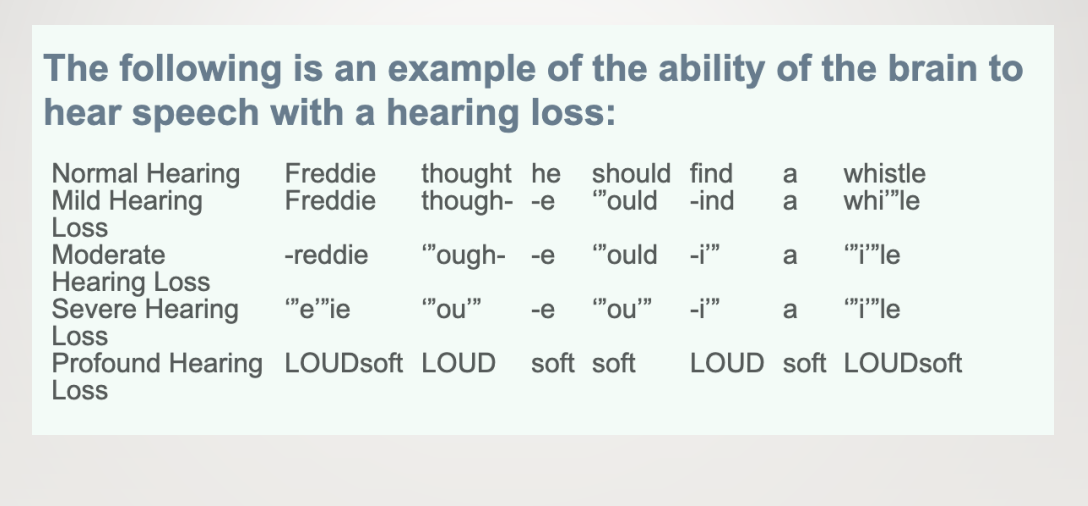
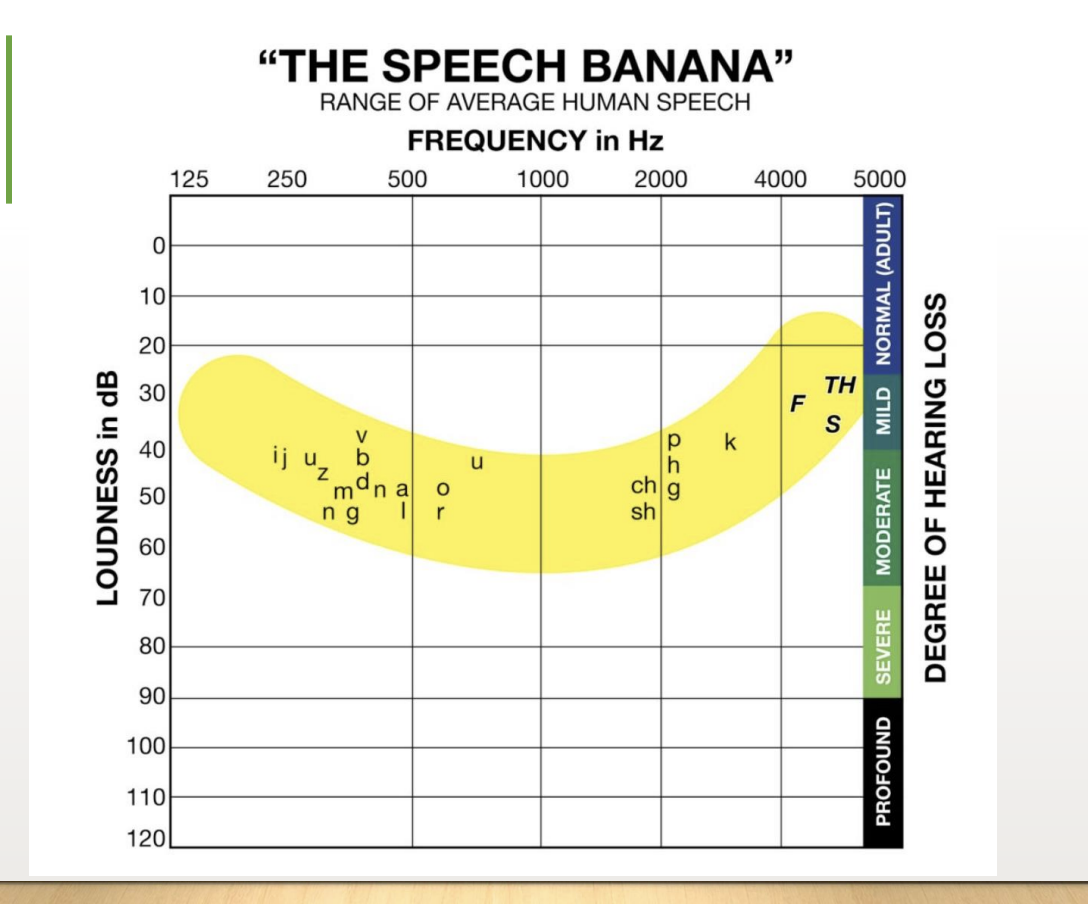
Example of Perception with HL
Speech Banana
True or False: Do not assume a slight loss will not impact their speech/ language skills, particularly in academic setting
True
Slight Loss (16-25 dB)
Perceived as if index fingers are in ears
Difficulty hearing faint or distant speech
Child can miss up to 10% of the speech signal at a distance of greater than 3 feet
This is amplified in background noise (imagine a classroom)
Preferential seating
FM System
Mild Loss (26-40 dB)
Greater listening difficulties than “plugged-ear” hearing loss
Can hear but misses parts of speech
Leads to a misunderstanding of the message
30 dB Loss
Child can miss up to 25-40% of speech signal
40 dB Loss
A child misses up to 50% of the speech signal
Will frequently have difficulty learning early reading skills
Sound/letter association
Moderate (41-55 dB) HL
Associated with frequent misunderstanding of signal
50 dB HL
A child may miss up to 80% of the speech signal
Without early amplification, a child will likely be language delayed with impaired syntax, limited vocabulary, disordered speech sound production, and flat vocal quality
Even with proper amplification, but with sufficient background noise = child will miss much of what is being said, as the signal-to-noise ratio is corrupted
Perception with Severe HL
Perception of sound is very limited
Earlier child wears amplification consistently with parents/caregivers providing language models in activities of daily living and/or intensive language intervention (verbal or sign or both) increases chances that speech, language, and learning will develop at a relatively normal rate
The ability of the brain to interpret sounds as meaningful input is determined by the patient’s individual ability and intensive intervention prior to 6 months of age
Hearing loss greater than 70 dB = candidates for cochlear implant (CI)
90 dB+ hearing loss = won’t perceive most speech sounds with a traditional hearing aid
Importance of Modeling
Modeling language will be crucial for language development since children imitate what they hear
Amount this is done will affect how much and how well the child speaks
True or False: Not Important for a child to look at the parent who is talking to learn how to begin to read lips as a compensatory strategy
False
True or False: You should control distance between speaker and listener by being no more than 5 feet away, especially important in young children
True
Suggestions for parents
Talk slightly louder than normal
Minimize the background noise
Use language stimulation strategies:
Parallel and self talk during activities
Expansions of what child says
Expatiations by adding new information
Use new words
Provide adult speech model for speech sound development
Read aloud together
Should begin when the child is less than a year old
Can help promote bonding and language growth
Work with an SLP