Peds/OB 4.2: GI
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
What are the definitions of atresia, stenosis, & volvulus, respectively?
Atresia: closed/absence of a natural body passage
Stenosis: narrowing
Volvulus: an obstruction caused by twisting of the stomach or intestine
What is meant by VACTERL?
Group of growth abnormalities that often occur together
V: vertebral anomalies
A: anal atresia/agenesis
C: cardiac defects
T: trachea (fistula or atresia)
E: esophagus (fistula or atresia)
R: renal abnormalities
L: limb abnormalities
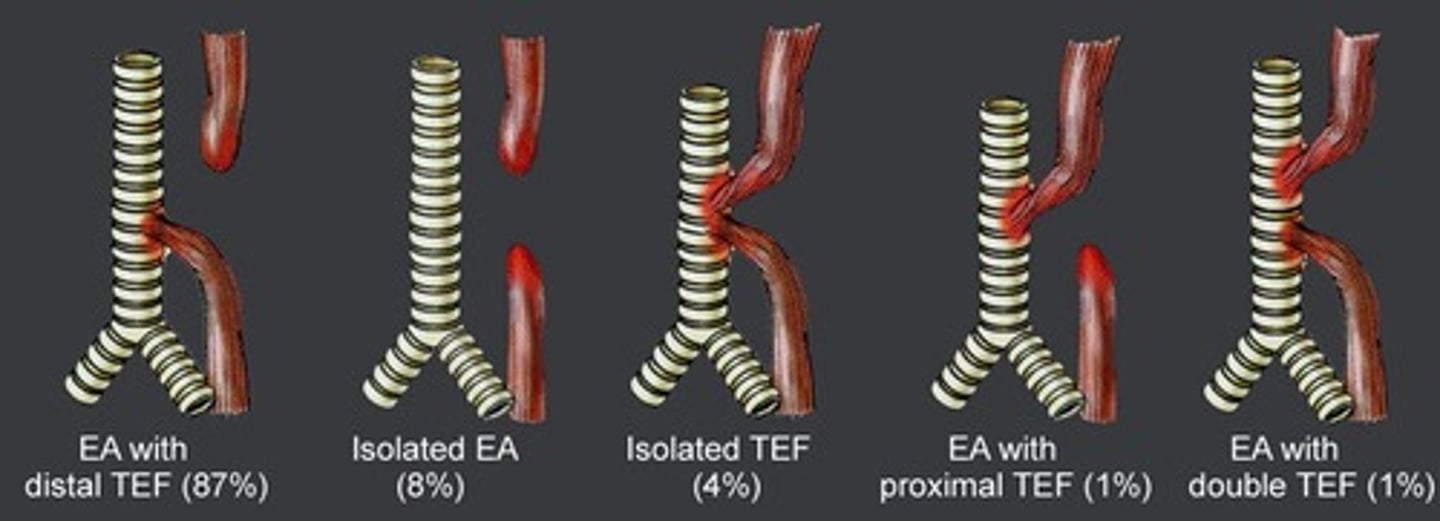
What is the most common type of esophageal atresia (EA) / tracheoesophageal fistula (TEF) combo?
EA w/ distal TEF (though there are several possible combos)
What are some s/sxs of EA/TEF? What does the mother often have a history of?
Respiratory distress shortly after breath worsened w/ feeding, regurgitation, excessive salivation, drooling, signs of aspiration pneumonia, failure to pass NG tube; polyhydramnios
What is the best initial test to diagnose EA/TEF, & what will be seen? What other test should we order?
Plain film (CXR) - blind upper pouch appearance as well as a coiled NG tube; echocardiogram (remember condition is part of VACTERL)

What is the definitive treatment for EA/TEF?
Surgical repair
What is duodenal atresia, & what is it often associated with? What is a way we may detect this before birth?
Congenital absence or complete closure of part of the duodenum; trisomy's (especially Down syndrome); fetal US may show polyhydramnios
What are some s/sxs of duodenal atresia?
Bilious vomiting, failure to pass meconium (FPM), failure to thrive (FTT), scaphoid abdomen w/ epigastric distension
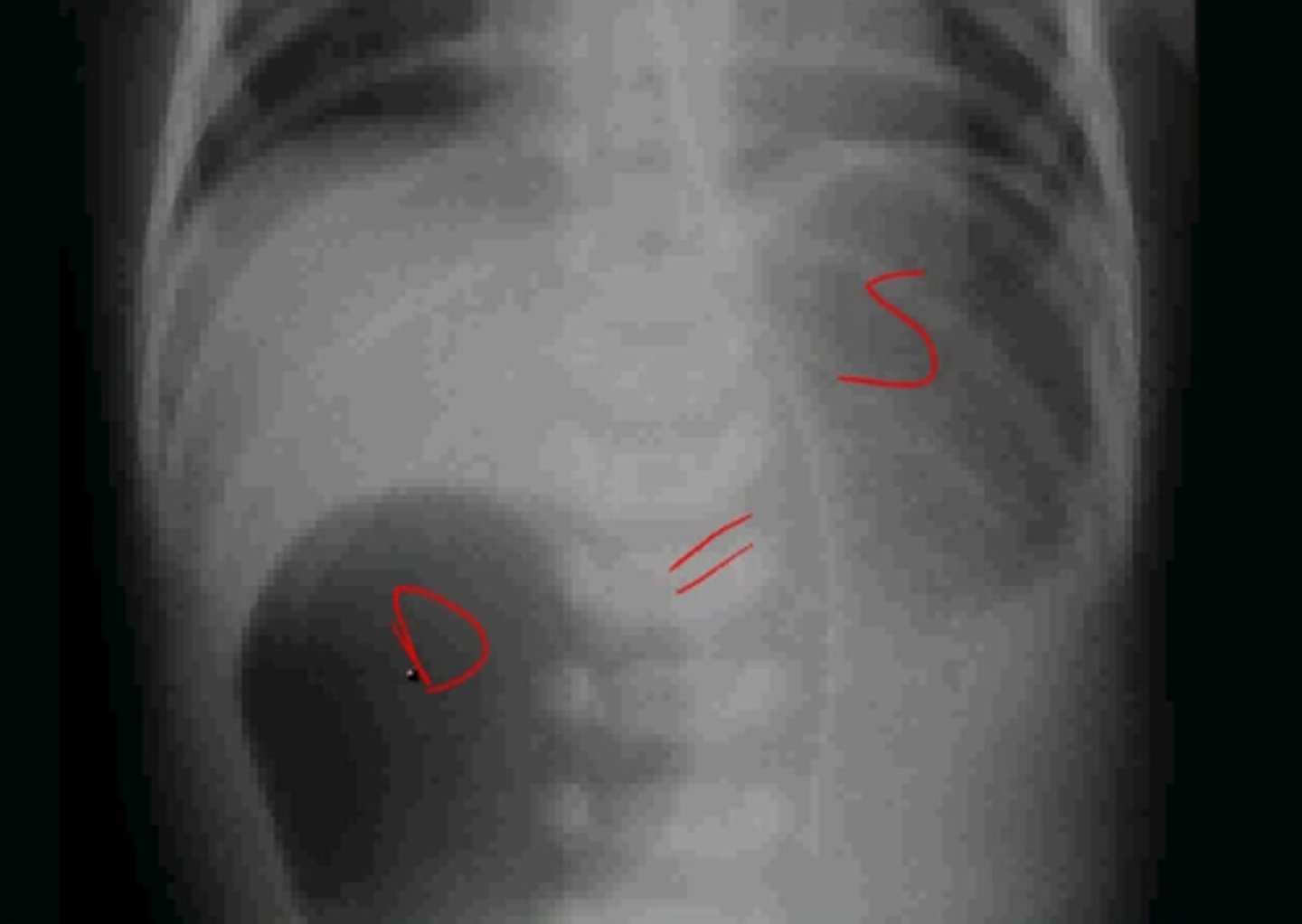
What is the best initial diagnostic test for duodenal atresia, & what will be seen? What condition do we need to absolutely r/o before diagnosing this?
Abdominal x-ray - shows "double bubble" sign; need to r/o volvulus (contrast enema can d/dx these)
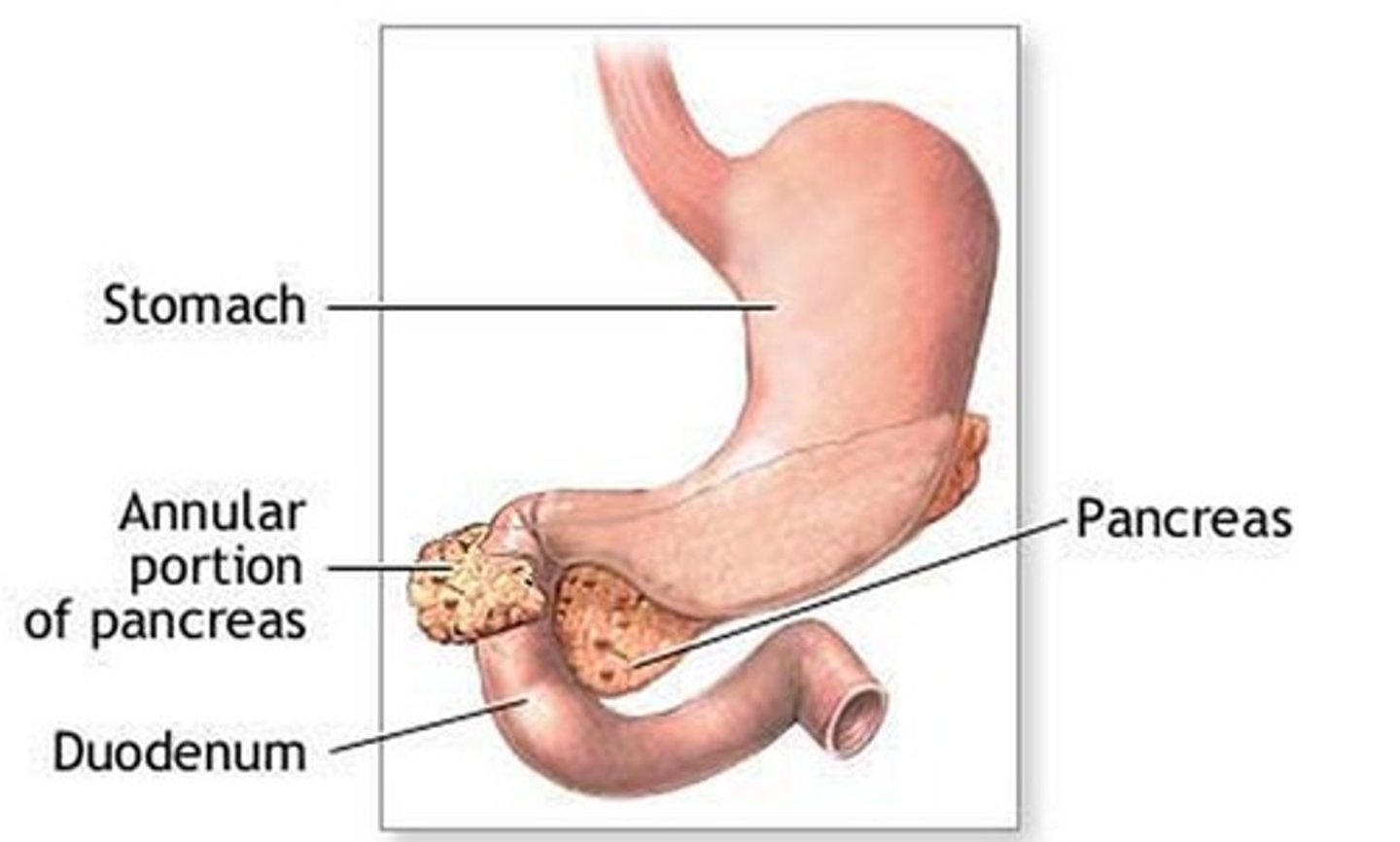
If a patient is found to have an annular pancreas while undergoing corrective surgery for duodenal atresia, what do we do?
No clue, but I do know that we never divide the pancreas
What is intestinal atresia, & what is it often associated with?
Atresia elsewhere in the GI tract (anywhere but the duodenum); vascular accidents in utero (as opposed to congenital like in duodenal atresia)
What are some s/sxs of intestinal atresia?
Similar to duodenal atresia - bilious vomiting in the first 24-48 hrs, FPM, abdominal distension
What is the best initial diagnostic test for intestinal atresia, & what will be seen? What is an additional test we can do to aid diagnosis (technically the "best" test)?
Abdominal x-ray - shows "apple peel" sign or triple bubble sign; contrast enema
How is intestinal atresia treated?
Peds surgery consult; continue parenteral nutrition post op until stool passes
What is hypertrophic pyloric stenosis? What are some s/sxs?
Hypertrophy of pylorus muscle resulting in gastric outlet syndrome; projectile non-bilious vomiting followed by a desire to feed (nothing is getting past), dehydration (sunken fontanelles), palpable olive-like mass in the epigastric/RUQ area
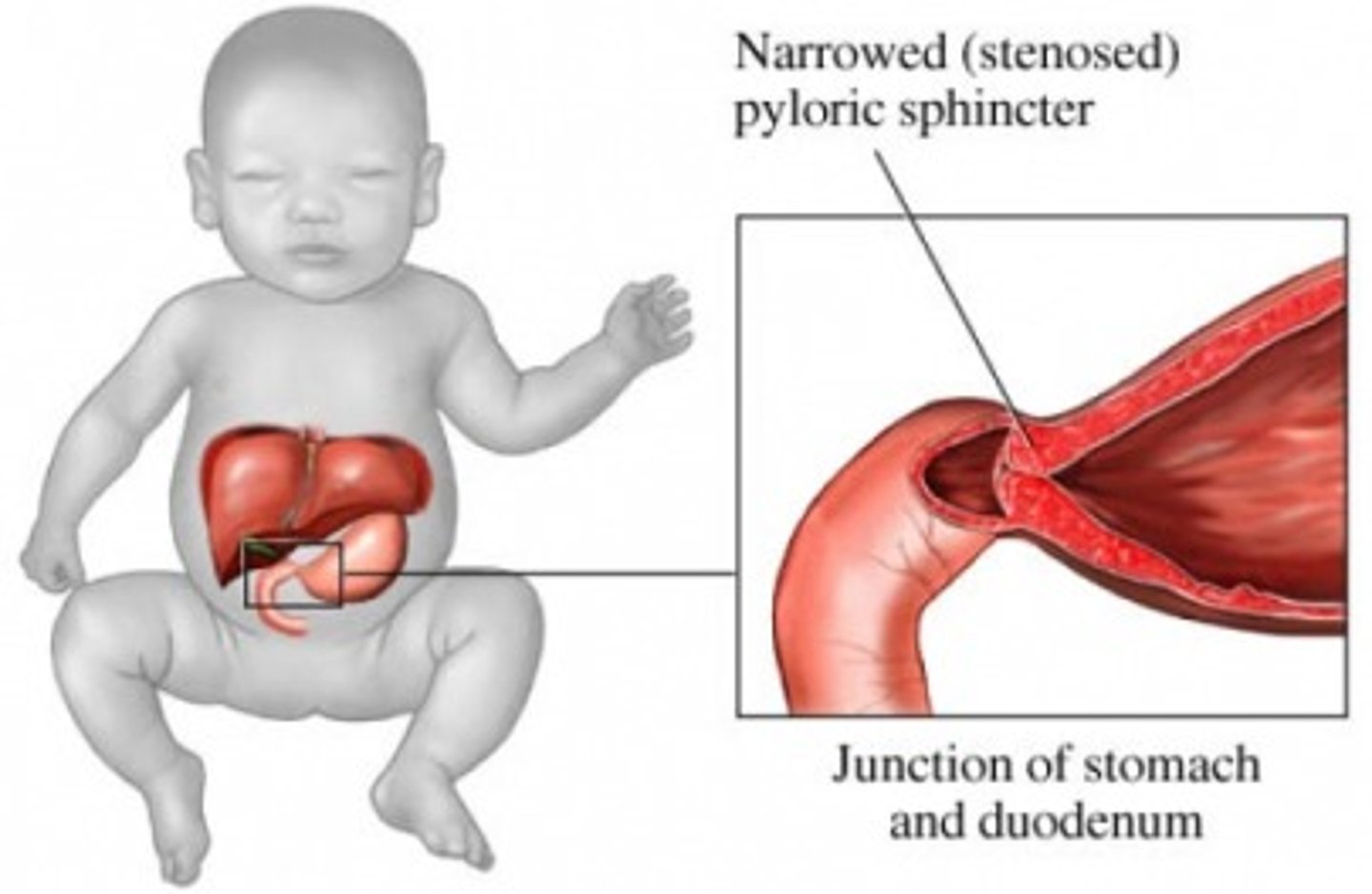
What is best initial & best overall test to diagnose hypertrophic pyloric stenosis? What will be seen?
Initial: abdominal US
Best: upper GI contrast series - string/apple core sign

What is the first step of treating hypertrophic pyloric stenosis? What do we do after this?
Correct dehydration & electrolyte abnormalities via normal saline & K+ administration (monitor UO to ensure adequate hydration); pediatric surgical consult
What is intestinal malrotation, & what is it often caused by?
Abnormal/incomplete rotation of the bowel during fetal development; Ladd's bands (fibrotic bands that cover parts of the small intestine)
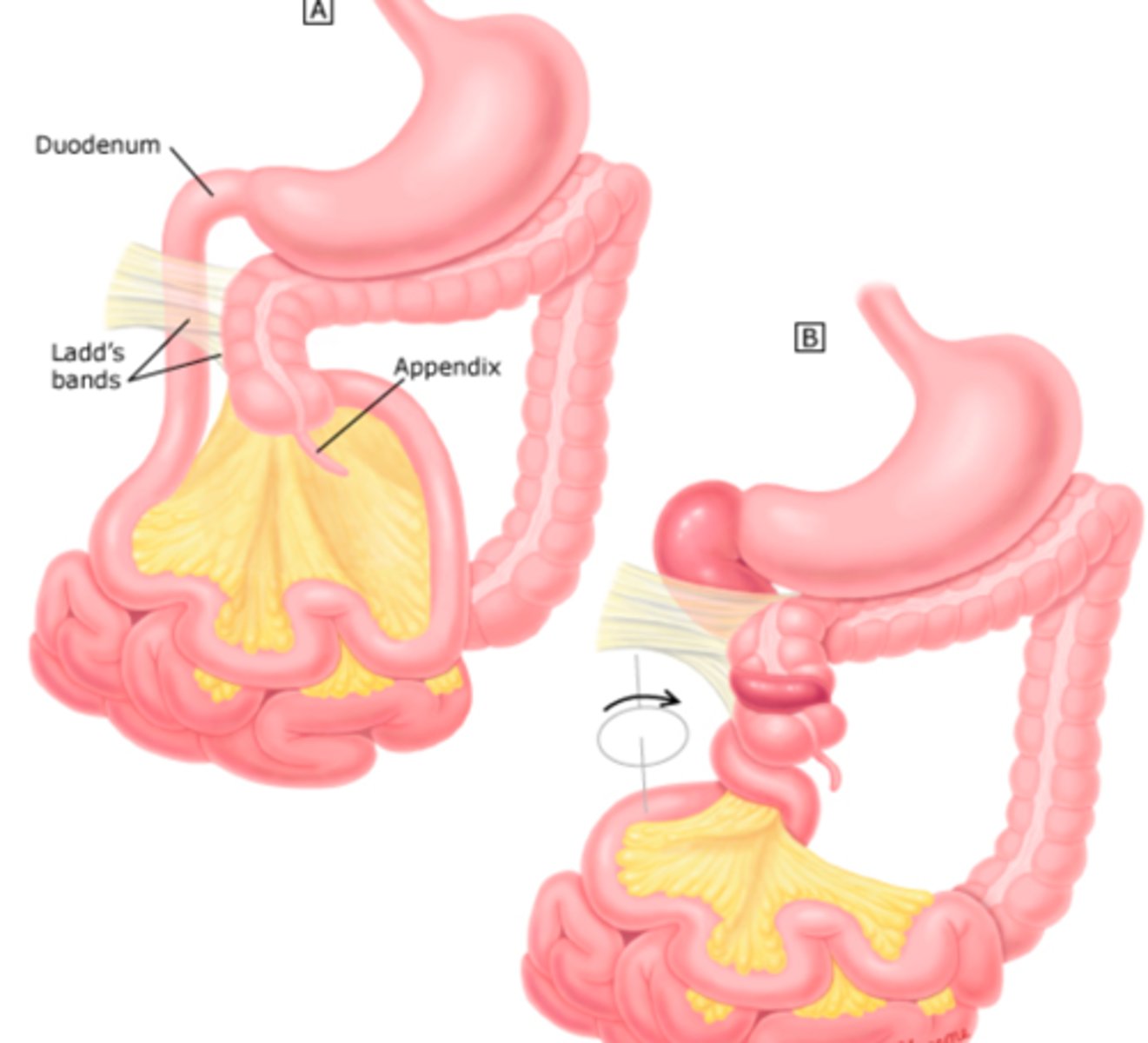
What are the 2 major possible complications of intestinal malrotation?
Intestinal obstruction (usually due to Ladd's bands) or midgut volvulus (small bowel ischemia)
What are some s/sxs of malrotation/midgut volvulus?
Bilious vomiting, bloating, distension, fever, N/V, blood-streaked stool, acute onset of severe pain out of proportion to the PE in a previously healthy baby
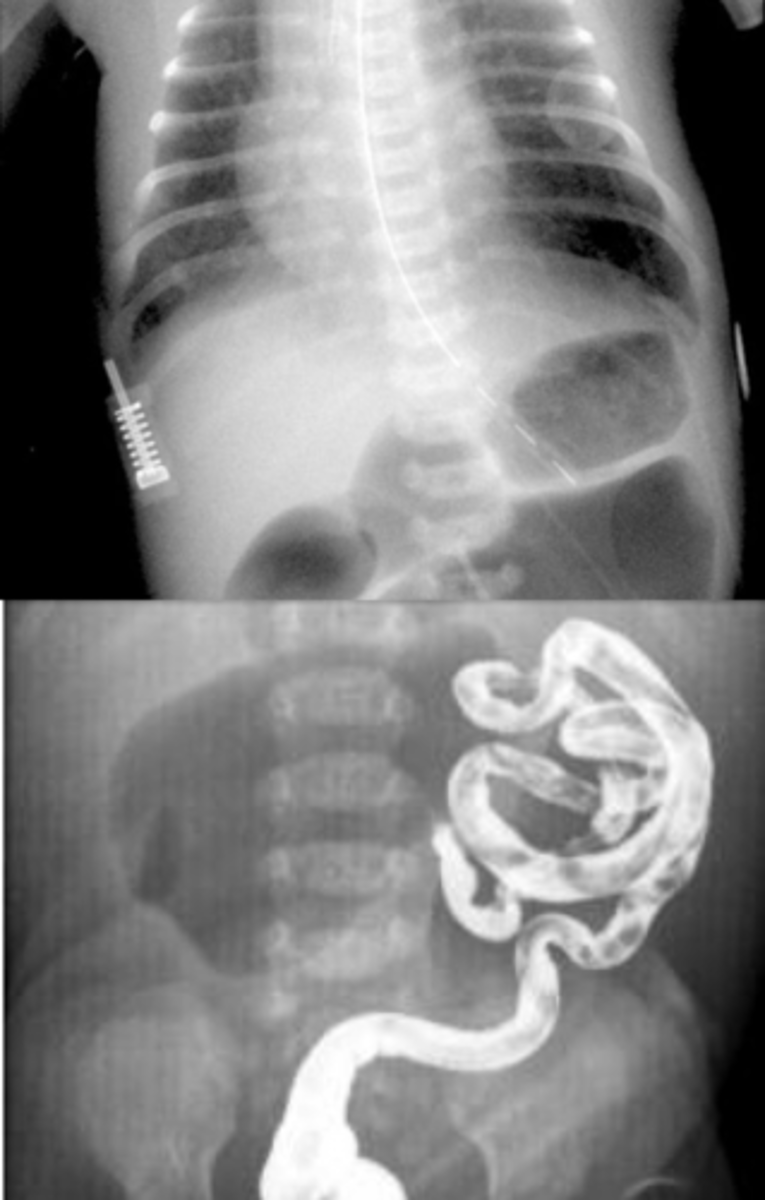
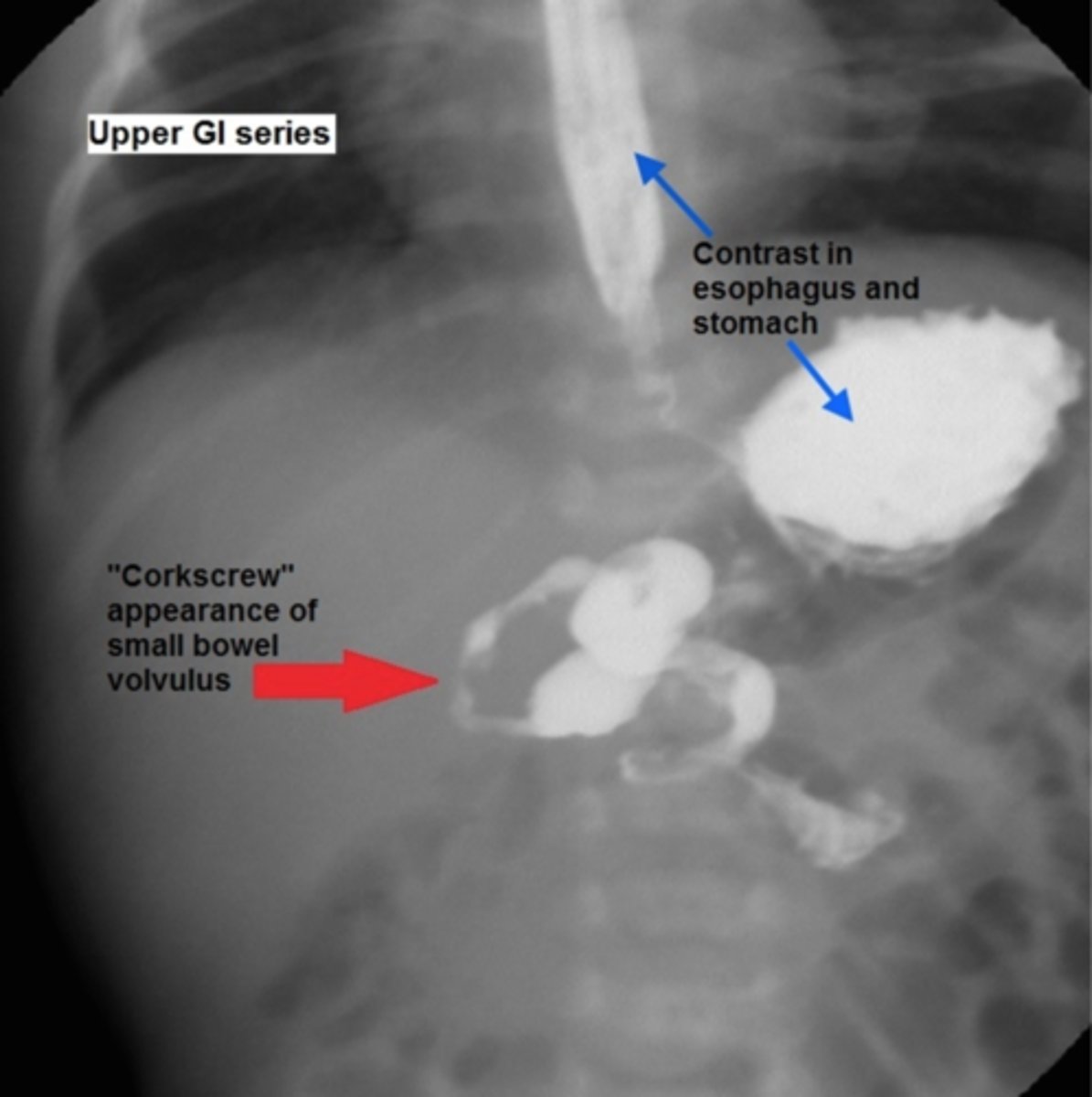
What is the best initial diagnostic test for suspected malrotation/midgut volvulus, & what must this be followed up by? What will be seen?
Initial: abdominal x-ray - double bubble sign and/or air-fluid levels (remember need to d/dx duodenal atresia from this)
Best: upper GI contrast series/contrast enema - twists of barium w/ bowel pushed over to the right
How is malrotation/midgut volvulus managed?
Emergent peds consult & surgical correction (usually cut Ladd's bands & resect any dead bowel)
What is omphalocele, & when is it usually diagnosed?
Defect of the abdominal wall musculature resulting in protrusion of the abdominal viscera through the umbilical cord, encased by the peritoneum; in utero via US

How is omphalocele treated?
Initial = cover exposed area w/ moistened sterile gauze to prevent fluid loss & infection; pediatric surgical consult = definitive
What is gastroschisis? Again, when is it usually diagnosed?
Incomplete fusion of the abdominal wall results in free herniation where abdominal viscera are not protected by peritoneum; in utero via US

How does the risk of complications with gastroschisis compare to that of omphalocele?
Patients are at a much higher risk of things such as peritonitis & sepsis
How is gastroschisis treated?
Initial: cover abdominal contents w/ moistened sterile gauze
Definitive: urgent surgery within 24-48 hrs
What is a congenital diaphragmatic hernia (CDH), & what is the primary complication of this condition?
Failure of diaphragmatic tissue to close resulting in the abdominal contents to herniate into the thoracic cavity; respiratory insufficiency (herniated intestines interfere w/ lung development)
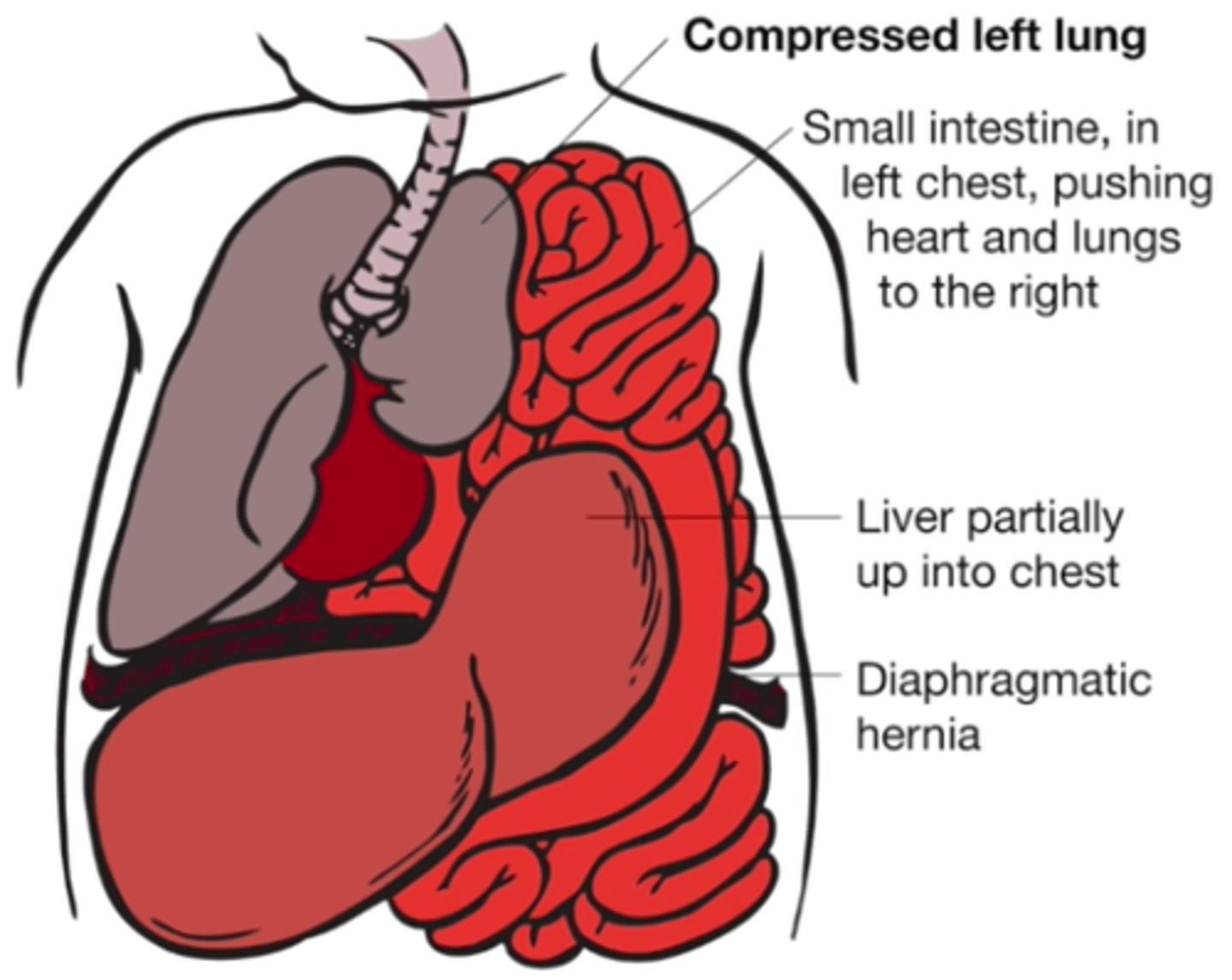
What are some s/sxs of a CDH?
Respiratory distress, scaphoid abdomen, shift of heart sounds to the right, tachypnea, nasal flaring, cyanosis, bowel sounds or absent breath sounds on affected side
What is the best initial test for a CDH? How is it managed?
Diagnosis: CXR
Treatment: intubation & mechanical ventilation, surgery after 24-48 hrs (delayed to allow for improvement in pulmonary HTN)
What is meconium ileus, and what condition is it super highly-associated with?
Impaction of meconium in the small bowel; cystic fibrosis until proven otherwise
What are some s/sxs of meconium ileus?
Abdominal distension, bilious vomiting, FPM, respiratory complications if distension
What is the best initial test to diagnose meconium ileus, & what should this be followed up by? What will be seen?
Initial: abdominal x-ray - shows multiple loops of small bowel in "soap-bubble" appearance
F/U: upper GI contrast series & contrast enema - shows microcolon inspissated w/ meconium

How is meconium ileus managed?
During diagnostic enema, administer n-acetylcysteine (NAC) to dissolve meconium (works ~50% of the time); unsuccessful enemas will require pediatric surgical consult
What is meconium plug syndrome, & how is it different from meconium ileus? What is it often associated with?
Impaction of meconium not due to meconium abnormalities (as in meconium ileus), but rather because the intestine is functionally immature; infants w/ diabetic moms who were on MgSO4 (given to prevent preeclampsia)
How is meconium plug syndrome diagnosed? What is seen?
Contrast enema - incomplete microcolon (d/dx from meconium ileus where the entire colon will be micro)

How is meconium plug syndrome treated? What other condition does this pathology sometimes coexist with?
NAC administration during the diagnostic enema usually works (very few patients require surgery); Hirschsprung's disease
What is Hirschsprung's disease, & what area of the GI tract does it tend to affect?
Absence of ganglion cells in the mucosal & muscular layers of a segment of the colon leads to impaired peristalsis; rectosigmoid area
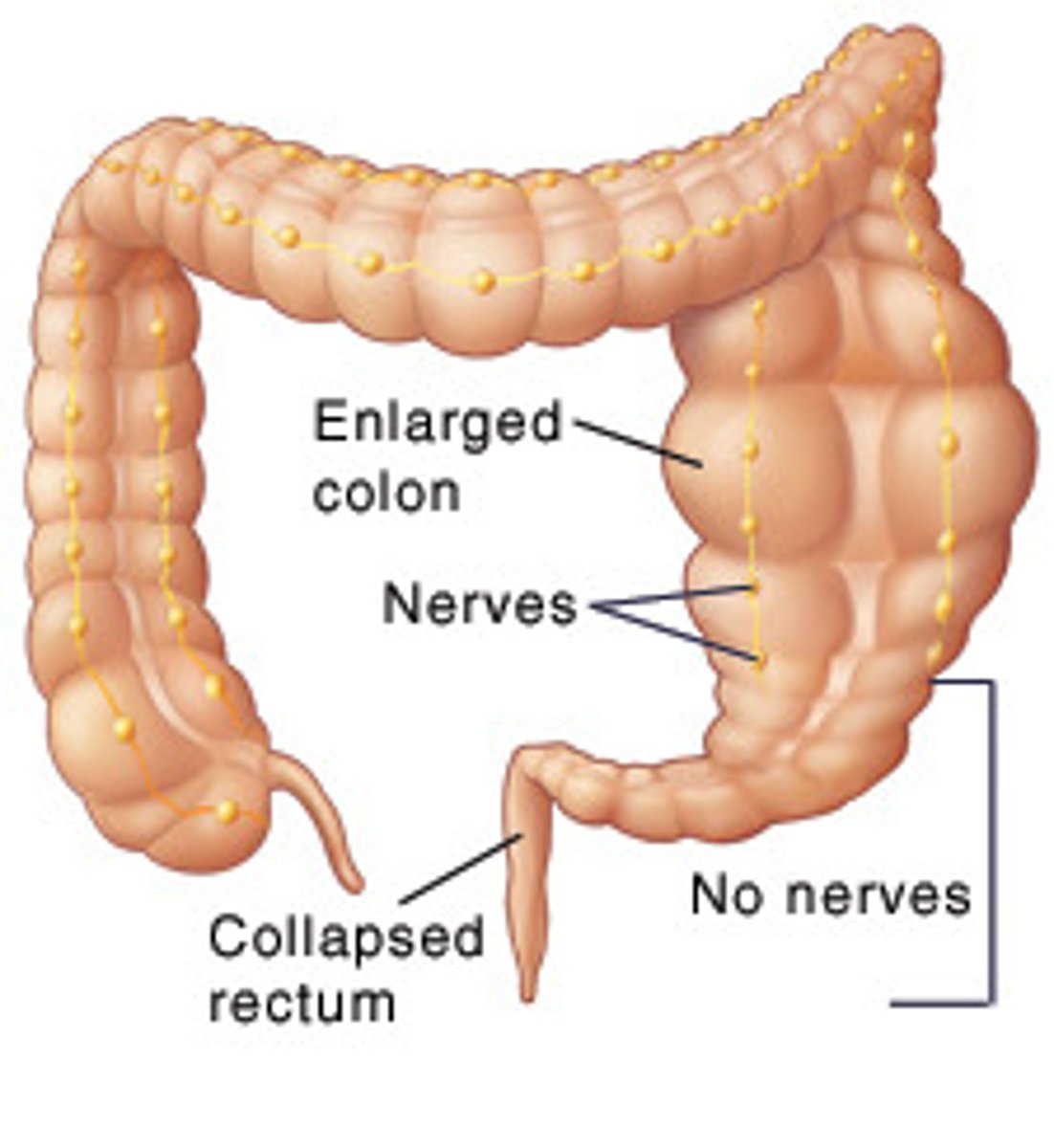
What are some s/sxs of Hirschsprung's disease? What is a characteristic PE finding?
FPM, vomiting, abdominal distension, enterocolitis; empty rectal vault on DRE, but explosive release of stool or flatulence after removing finger
What is the best initial test to diagnose Hirschsprung's disease, & what do we follow this up with? What test is definitive?
Initial: abdominal x-ray followed by contrast enema & anorectal manometry (evaluates whether or not they can create pressure)
Definitive: rectal biopsy

How is Hirschsprung's disease treated?
Surgical resection of the aganglionic portion
What is necrotizing enterocolitis, & what kinds of babies does it tend to affect?
Unclear etiology leads to hypoxia of the bowel leading to intestinal sloughing, bacterial invasion, inflammation, & gangrene/perforation; premature babies
What are some s/sxs of necrotizing enterocolitis?
Premature baby who comes in w/ abdominal distension, belly pain, bloody stool, intolerance to feeds, vomiting, diarrhea, abdominal erythema, & possible shock

What is the best initial diagnostic test for necrotizing enterocolitis? What is a pathognomonic finding?
Abdominal x-ray; pneumatosis intestinalis (intramural air, dilated bowel, & edematous walls)

How is necrotizing enterocolitis treated? What are some indications for surgery?
Inpatient management, NPO, & broad-spectrum ABX (amp/gent, piperacillin/tazobactam); evidence of perforation, abdominal cellulitis, deterioration despite maximal medical support
What is an imperforate anus, & what is the difference between high & low lesions?
Abnormal termination of the anorectum
High: rectum may connect to the urinary tract
Low: rectum does not connect to the anus
What are some s/sxs of an imperforate anus?
Usually grossly visible, FPM (although high lesions may pass feces through the urinary tract), recurrent UTI, VACTERL association
How is an imperforate anus diagnosed & treated?
Diagnosis: combo of PE, UA, & pelvic radiographs
Treatment: surgical repair (also get an echo due to VACTERL association)
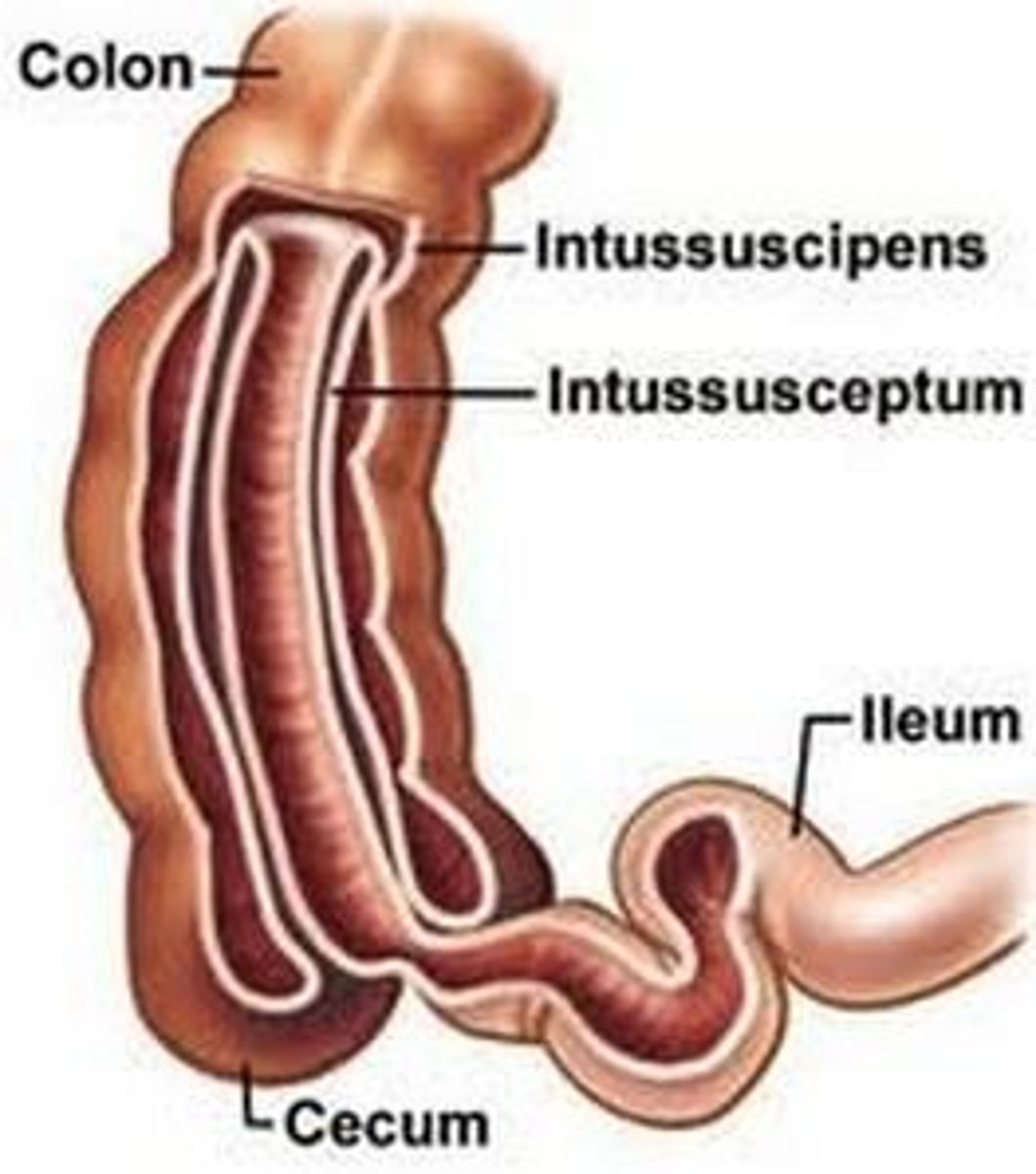
What is intussusception, & where is the most common area for this to occur? What is the most common lead point (trigger) for this?
Telescopic invagination of the bowel lumen resulting in obstruction; ileocolic junction; viral infection
What are some s/sxs of intussusception?
Bouts of severe colicky abdominal pain (interspaced by periods of lethargy), vomiting, blood in the stool ("currant jelly stool" = buzzword), possible sausage-shaped mass on PE

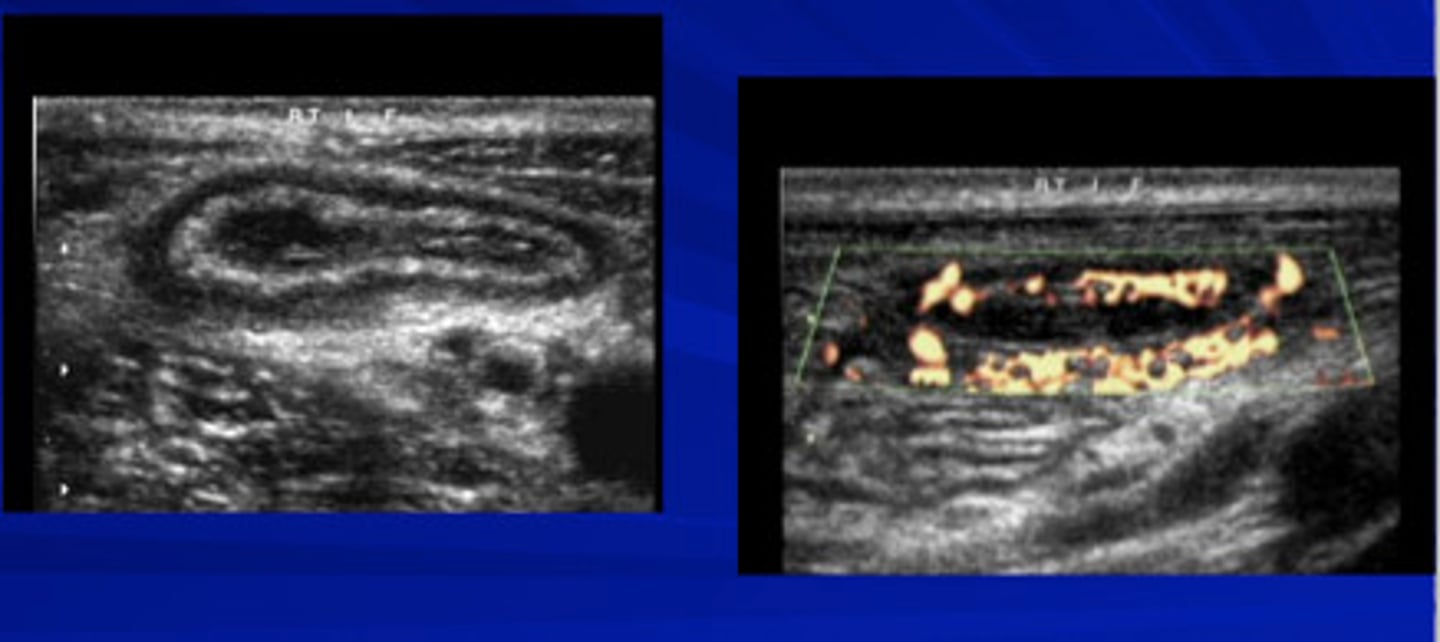
What is the best initial test for intussusception, & what will be seen? What is the best overall test for this condition?
Initial: ultrasound (shows "target sign")
Best: air contrast enema (both diagnostic & therapeutic)

How is intussusception treated?
Supportive care, air enema is ideal first & surgery can be done if this fails
What is Meckel's diverticulum, & how does it usually present?
Outpouching of the intestinal wall resulting from a fetal remnant that contains gastric & pancreatic mucosa; painless GI bleeding w/ maroon stool (Meckel's diverticulum until proven otherwise)
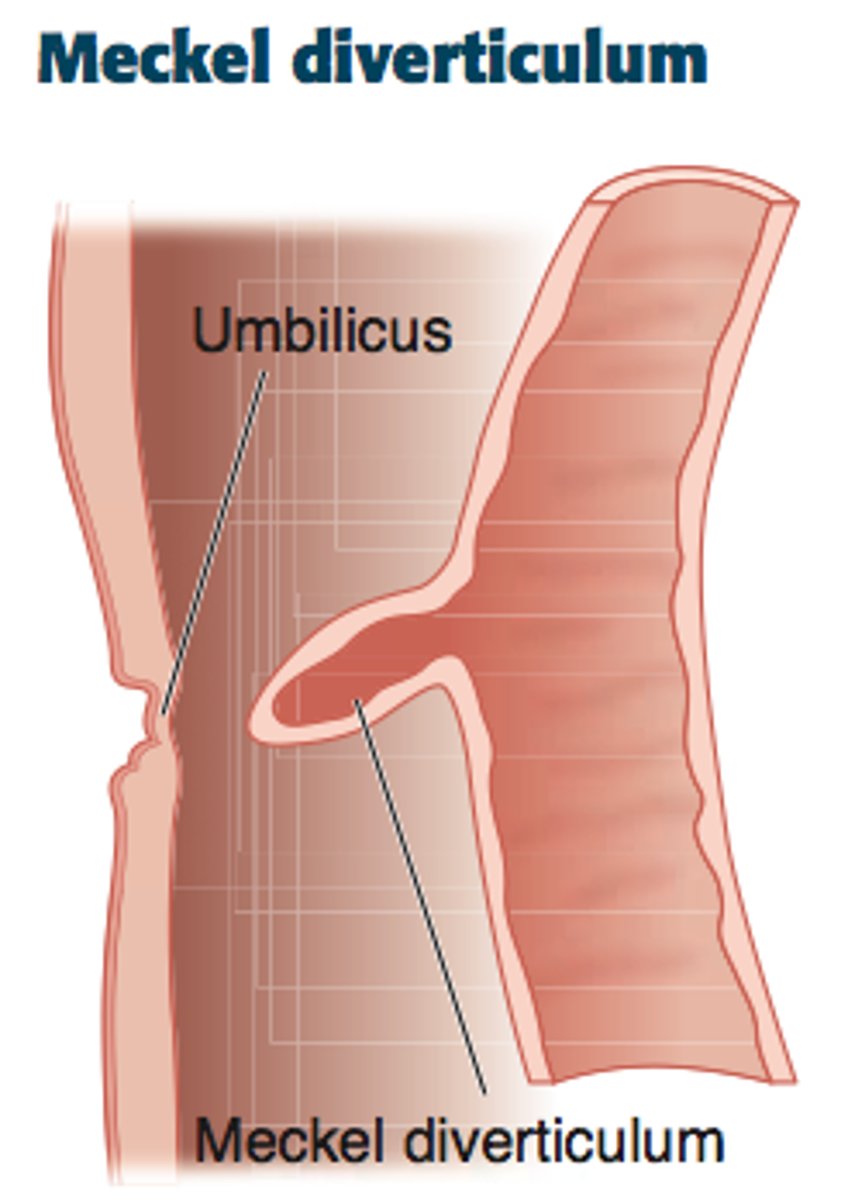
What is the Rule of 2's when it comes to Meckel's diverticulum?
Describes common patterns of this condition:
- Occurs in 2% of the population
- 2x more common in males
- Usually 2 ft from proximal ileocecal valve
- 2 inches in length
- 2 secretions: gastric & pancreatic
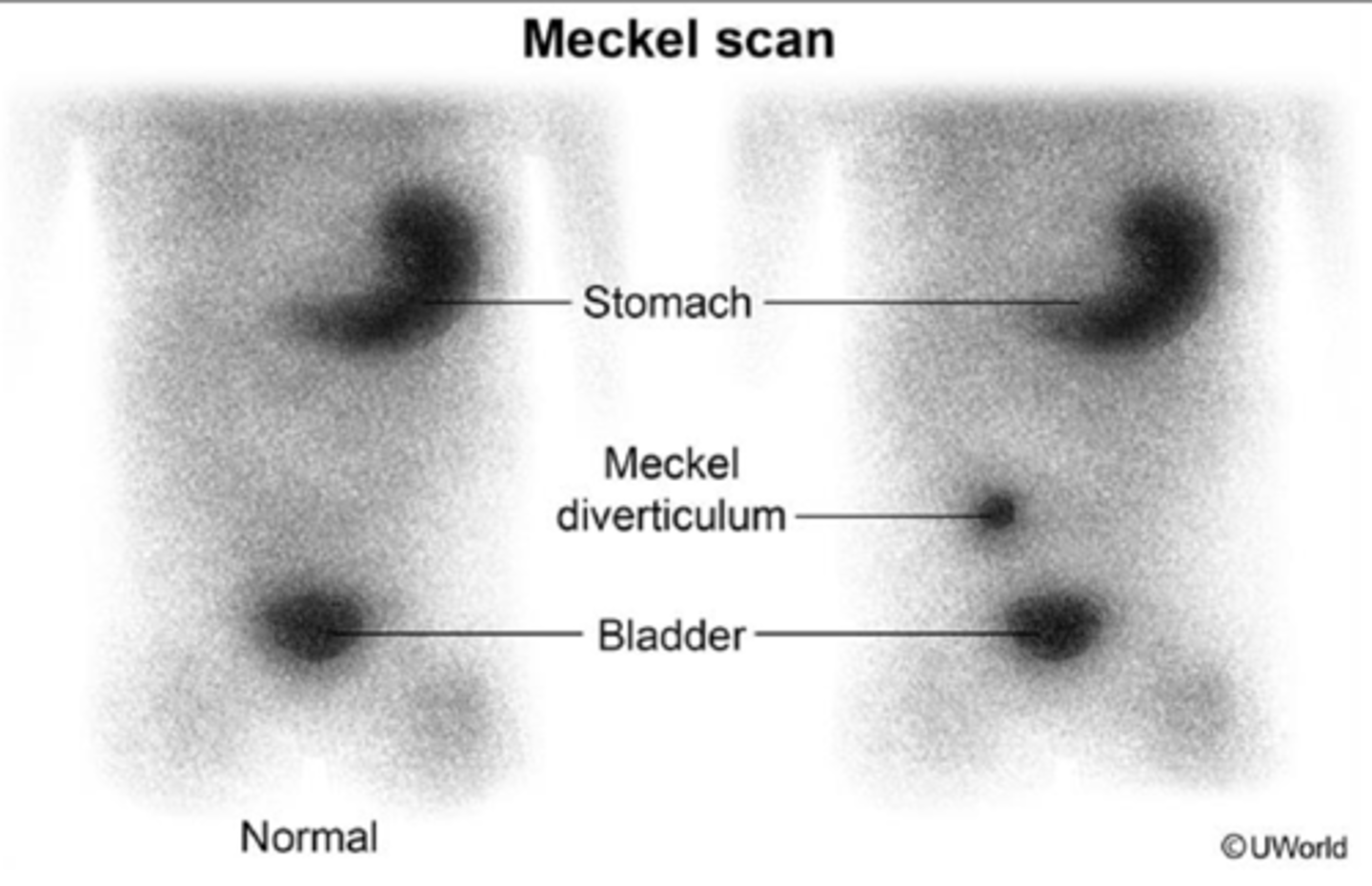
What is the best diagnostic test for Meckel's diverticulum? How is it treated?
Diagnosis: Tc-99 scintigraphy/radionucleotide scan
Treatment: surgery
What is acute appendicitis, & what is it often caused by? What is the most common lead point (trigger) in kids?
Sudden infectious inflammation of the vermiform appendix often due to obstruction of the appendiceal lumen by a fecalith; lymphoid hyperplasia

What are some s/sxs of appendicitis (particularly in kids)?
Usually starts as nonspecific malaise & constant periumbilical pain, patient may develop fever & nausea, pain may migrate to RLQ, possible urinary tract irritation present, pain to palpation of McBurney's point, guarding, psoas sign, obturator sign, Rovsing's sign
JUST KNOW: there is no single PE finding that is sufficient to rule in or rule out appendicitis, especially in kids. Any patient presenting with abdominal pain & no prior history of appendectomy needs to be considered for this condition
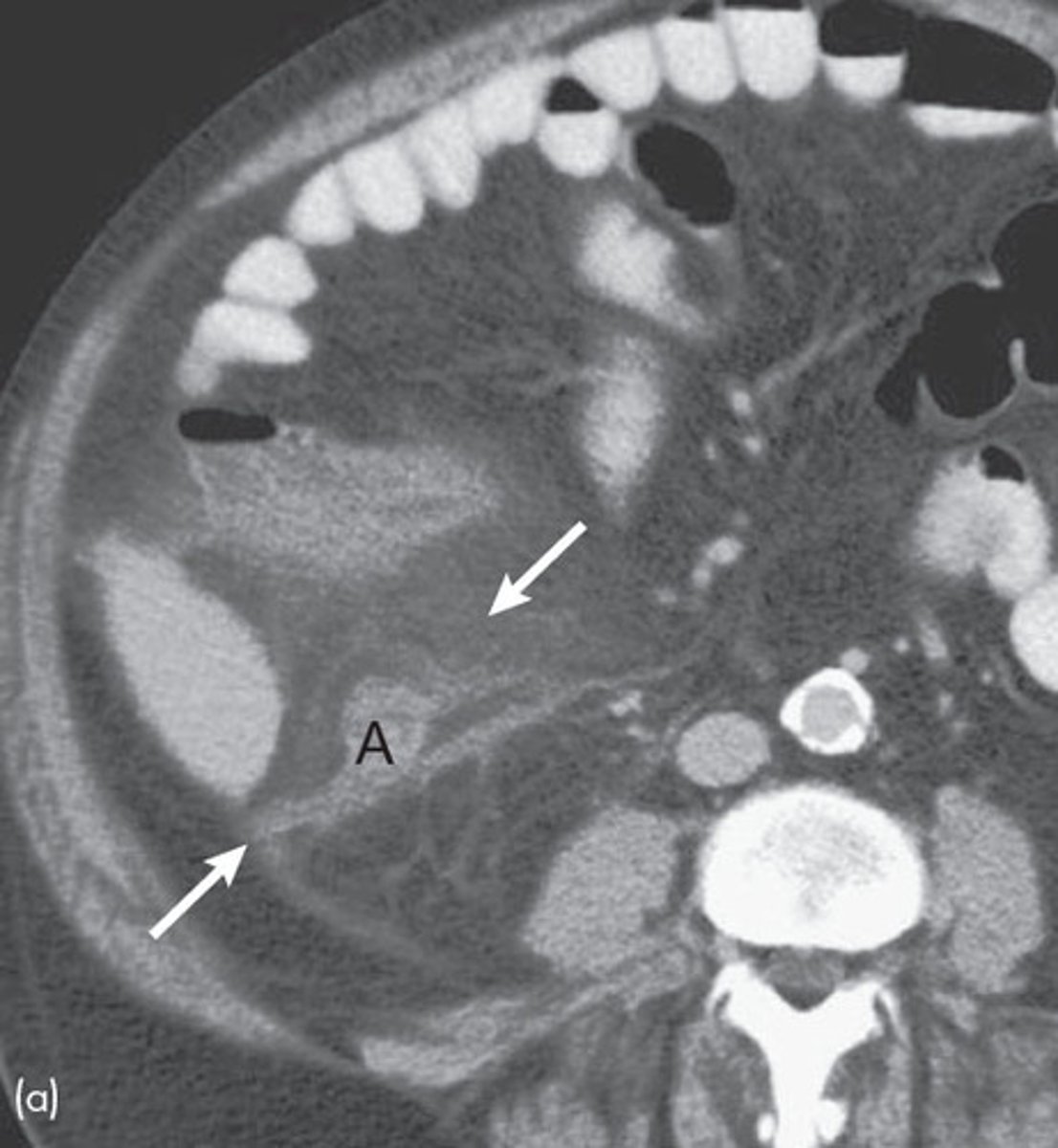
What is the best initial diagnostic test for appendicitis in kids, & what is this followed up by?
Ultrasound (in adults it's CT but we want to avoid radiation exposure here) followed by MRI (best test)
What is a finding on imaging that can clue us in that a patient has appendicitis?
Fat stranding around the appendix (indicates inflammation)
How is appendicitis managed?
Inpatient management & classic supportive stuff, pre-op ABX, appendectomy within 24 hrs
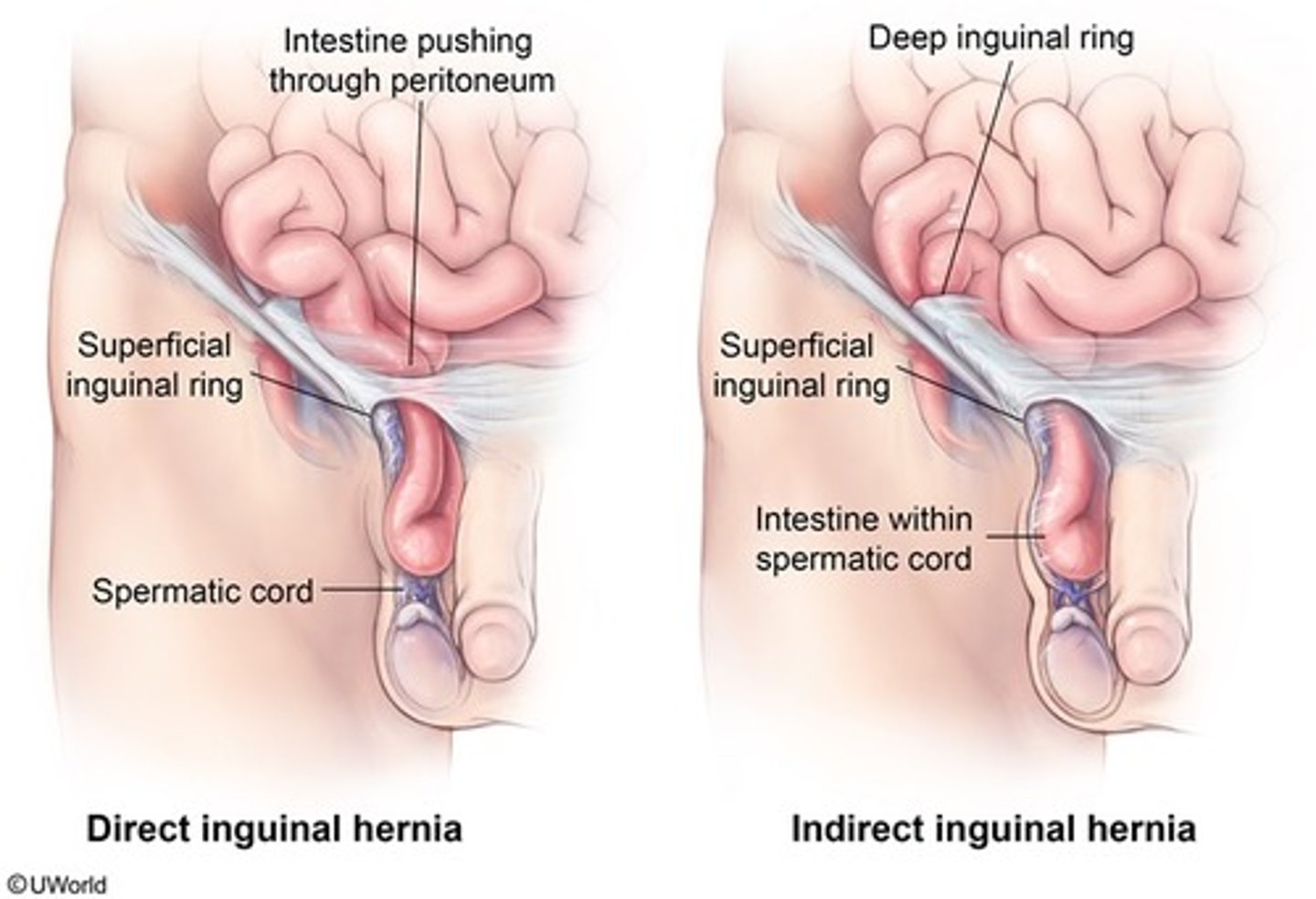
What is the difference between indirect & direct inguinal hernias, & which one is more common in kids?
Indirect: herniation of abdominal contents through deep inguinal ring & down inguinal canal (MC in kids)
Direct: herniation of abdominal contents through floor of inguinal canal
How are inguinal hernias diagnosed & treated?
Diagnosis: clinical
Treatment: herniorrhaphy (usually wait ~1 year before doing surgery tho because they'll often self-resolve; only exception is incarcerated/strangulated hernias)
What is an umbilical hernia, & what is it often caused by in kids? How does it present?
Protrusion of abdominal contents through naval, often due to a congenital defect in the linea alba; soft swelling beneath skin around umbilicus that protrudes during crying or straining

How are umbilical hernias diagnosed & treated?
Diagnosis: clinical
Treatment: herniorrhaphy (again usually wait until age 3 because 95% will resolve by then)
What is a patent omphalomesenteric duct, & how does it present?
Failure of this embryonic structure to close results in the ilium connecting to the umbilicus; herniation of the intestinal contents into the umbilical cord, mucoid/fecal discharge from the umbilicus (d/dx from umbilical hernia)

What is the best initial diagnostic test for a patent omphalomesenteric duct, & what test is used to confirm the diagnosis? How is this treated?
Initial = ultrasound, confirmatory = CT
Treatment: surgical excision
Where is the most common site for ingested foreign bodies to become lodged in kids? How do they usually present?
Cricopharyngeus muscle; drooling & feeding intolerance, esp. in young kids
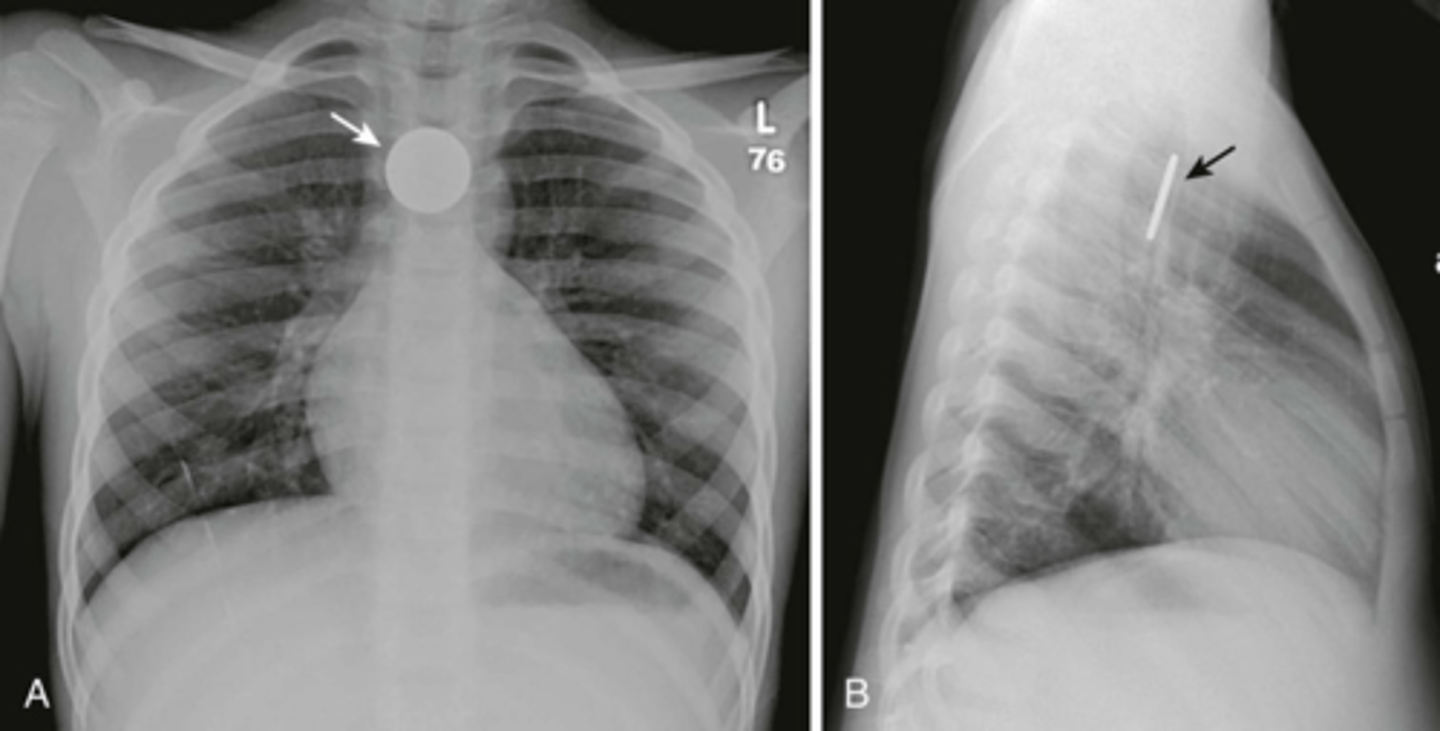
What is the best initial test for an ingested foreign body?
X-ray (get CT if object is not radiolucent)
How are ingested foreign bodies treated depending on if they're dull/sharp, longer than 6 cm, rounded > 2.5 cm, batteries, & magnets, respectively?
Dull/sharp: endoscopic removal if threatening perforation
Long: endoscopic removal
Round > 2.5 cm: endoscopic removal if not passed into stomach within 2-3 weeks or if not moved for > 1 week
Batteries: urgent endoscopic removal
Magnets: 1 is okay, 2 requires removal
As a whole, what are bezoars? What are trichobezoars, phytobezoars, pharmacobezoars, & lactobezoars, respectively?
Concentrations of nondigestable materials formed in the stomach
Tricho: hair
Phyto: vegetable fibers
Pharmaco: undigested meds
Lacto: milk curd

How are bezoars diagnosed & treated?
Diagnosis: US or CT
Treatment: endoscopic removal

What is the difference between functional fecal retention (FFR) & organic constipation? What are some s/sxs of each?
FFR: most common type, due to traumatic/environmental effects; may present after toilet training, normal growth & development
Organic: some underlying disease causing sxs (Hirschsprung's most common); delayed meconium passage, constipation during infancy, hx of pelvic surgery, inability to toilet train
What is the best initial test to diagnose constipation? How are FFR & organic subtypes treated, respectively?
X-ray (need to r/o Hirschsprung's via contrast enema, manometry, & biopsy tho too)
FRR: clean out fecal mass, soften stool, educate family
Organic: treat underlying cause
What is encopresis, & what is often caused by?
Repeated passage of stool in inappropriate places from a child who is chronologically or developmentally > 4 y/o; constipation
How is encopresis treated?
Stool evaluation, increase water intake, educate & support patient (avoid punishing), consider psych consult