Physio Ch. 13 Part 1 Electrical Activity in the Heart & ECG
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Cardiovascular System
Made of the heart and blood vessels
System that moves blood around the body
- Brings oxygen and nutrients to tissue
- Removes carbon dioxide and waste from tissues
- Regulation of blood volume and pressure
- Bodily communication via hormone transport
Atrioventricular (AV) valves
Valves that separate atria and ventricles
- Right AV valve / tricuspid valve
- Left AV valve / bicuspid valve / mitral valve
Semilunar valves
Valve between ventricles and vessels they empty into
- Right ventricle: Pulmonary valve
- Left ventricle: Aortic valve
Right AV valve/tricuspid valve
Located between the right atria and ventricle
Opens passively
- When atrial pressure is greater than ventricular
Cause first heart sound when they close
- “Lub”
Left AV valve/bicuspid valve/mitral valve
Located between the left atria and ventricle
Opens passively
- When atrial pressure is greater than ventricular
Cause first heart sound when they close
- “Lub”
Pulmonary valve
Located between the right vertical and pulmonary trunk
Opens passively
- When ventricular pressure is greater than arterial pressure
Cause second heart sound when they close
- “Dub”
Aortic valve
Semilunar valve
Located between the left vertical and aorta
Opens passively
- When ventricular pressure is greater than arterial pressure
Cause second heart sound when they close
- “Dub”
Pacemaker/nodal cells
Located throughout the heart but concentrate in Sinoatrial (SA) node and Atrioventricular (AV) node
Able to generate their own action potential
Sinoatrial (SA) node
Bundle of pacemaker cells that act as the pacemaker of the heart
Sets heart rate at 70-80 AP per minute
Makes a pacemaker potentials
Atrioventricular (AV) node
Bundle of pacemaker cells that act as the pacemaker of the heart
Sets heart rate at 40-60 AP per minute
Acts as the backup system for the pacemakers
- “Ectopic pacemaker”
Conduction fibers
Long cells that spread out across the heart to conduct electrical impulses
Large diameter for fast conduction
Myocardial contractile cells
The muscle cells of the heart that contract
Electrical synapses
Gap junctions between heart muscle cells
- Allow for the fast conduction of electrical impulses
Electrical Events of a Heartbeat
Step 1: SA node initiates an AP
Step 2: AV node transmits AP
Step 3: Impulse travels through atrioventricular bundle/bundle of His in interventricular septum
Step 4: Impulse travels down the left and right bundle branches to each ventricle
Step 5: Impulse spreads through the Purkinje fibers (“subendocardial conducting network”) throughout the ventricular myocardium
AV bundle/Bundle of His
Produces 20-40 AP per minute
Purkinje fibers
Produces 30-40 AP per minute
Acts as the backup system for the pacemakers
- “Ectopic pacemaker”
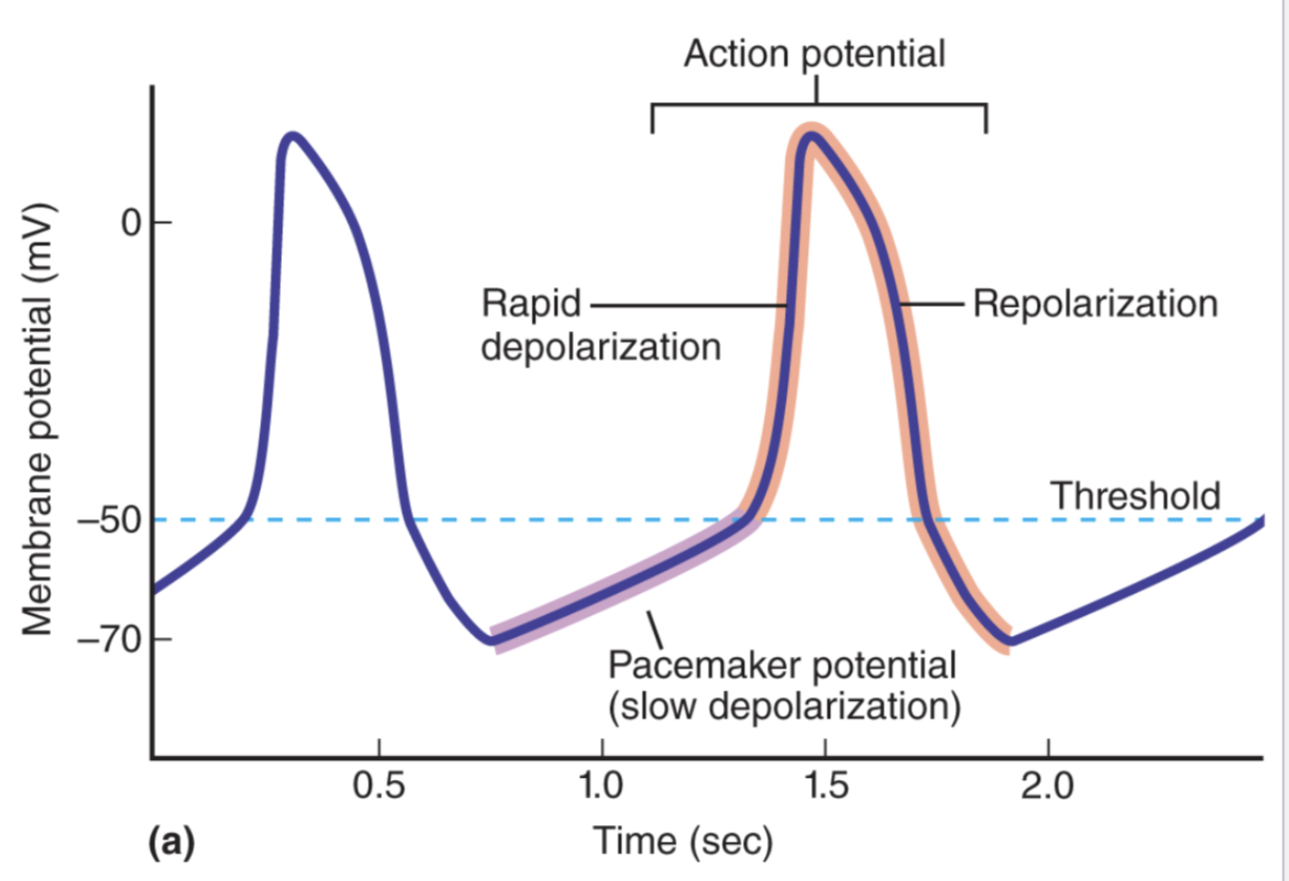
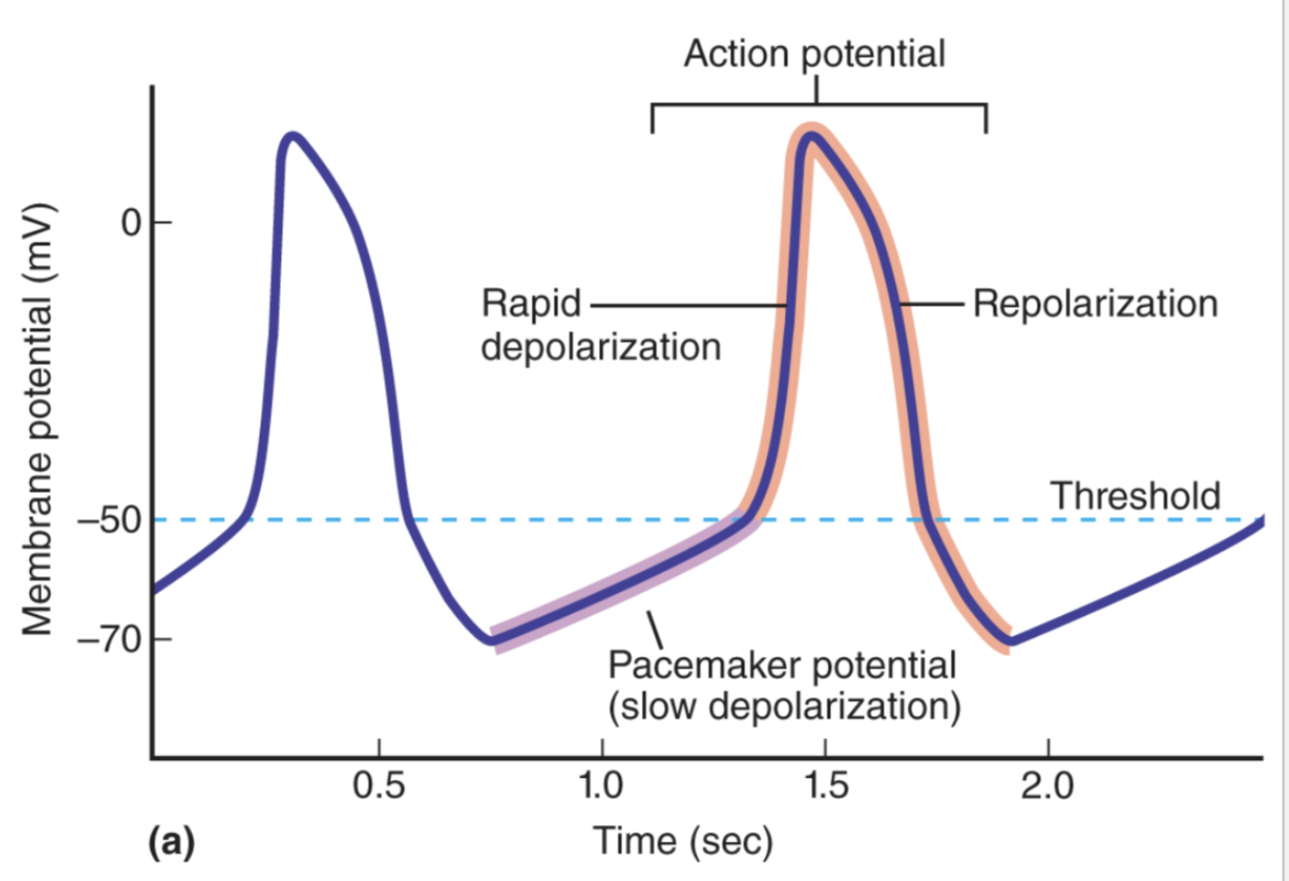
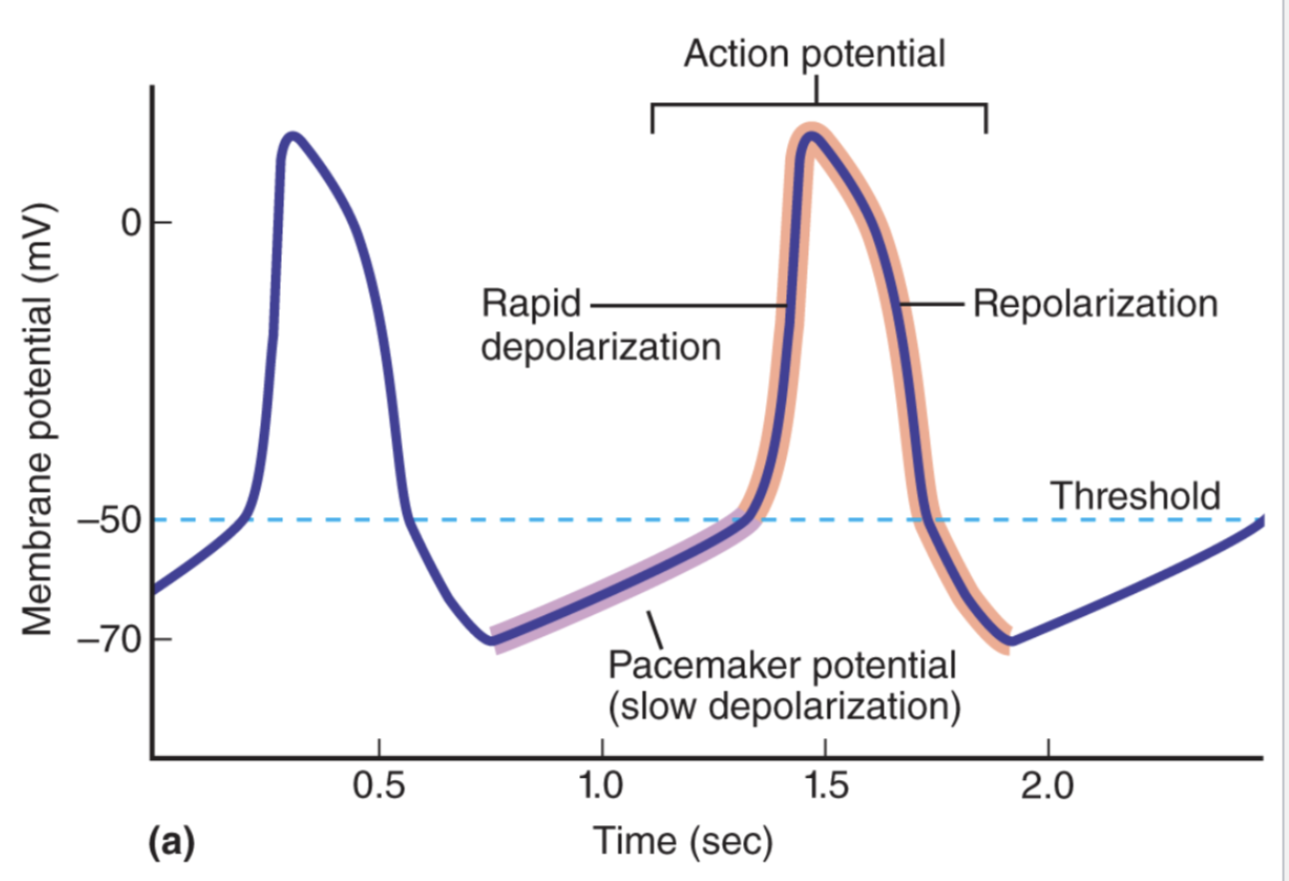
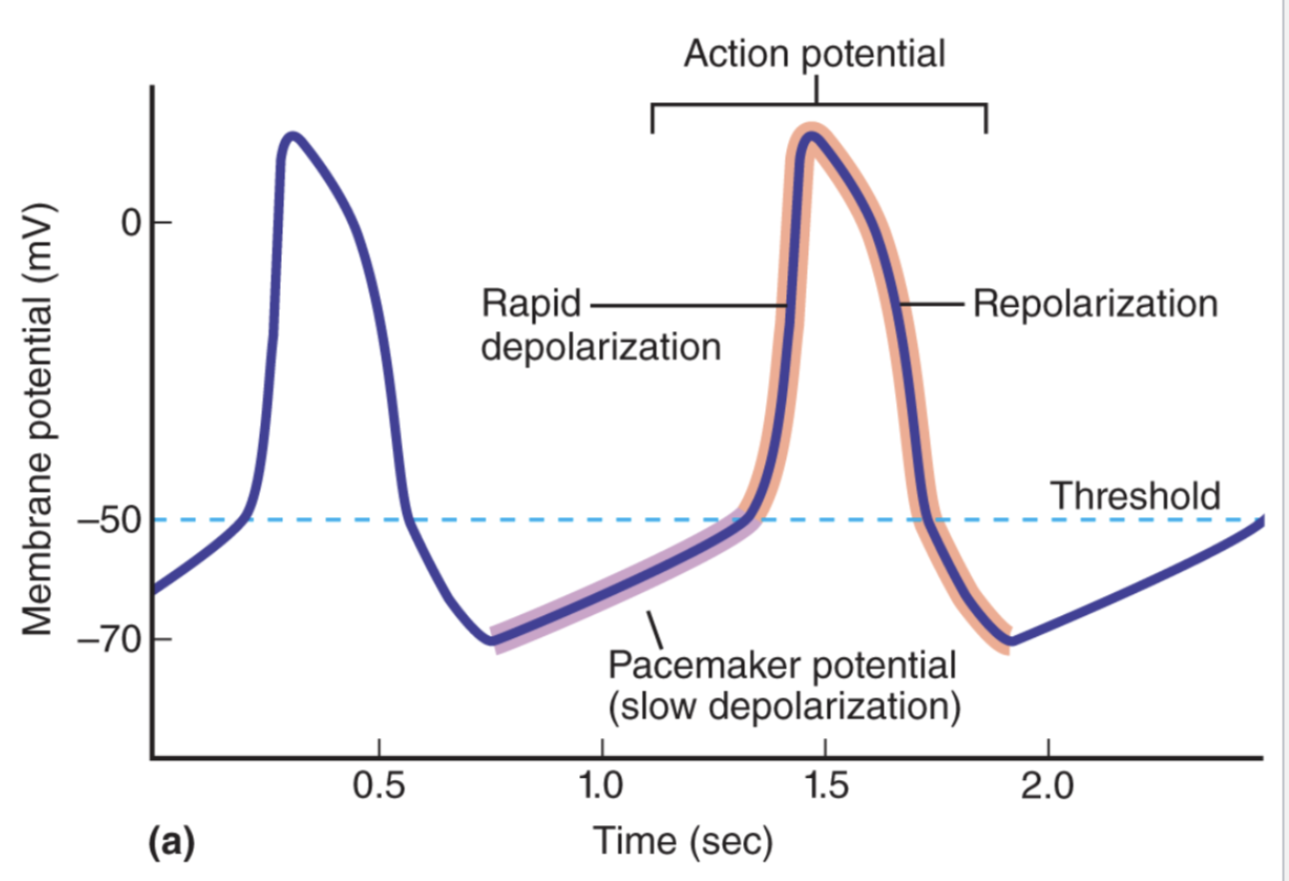
Pacemaker potential
A slow depolarization that is sent out to muscular cells of the heart after contraction
Continues until threshold is reached
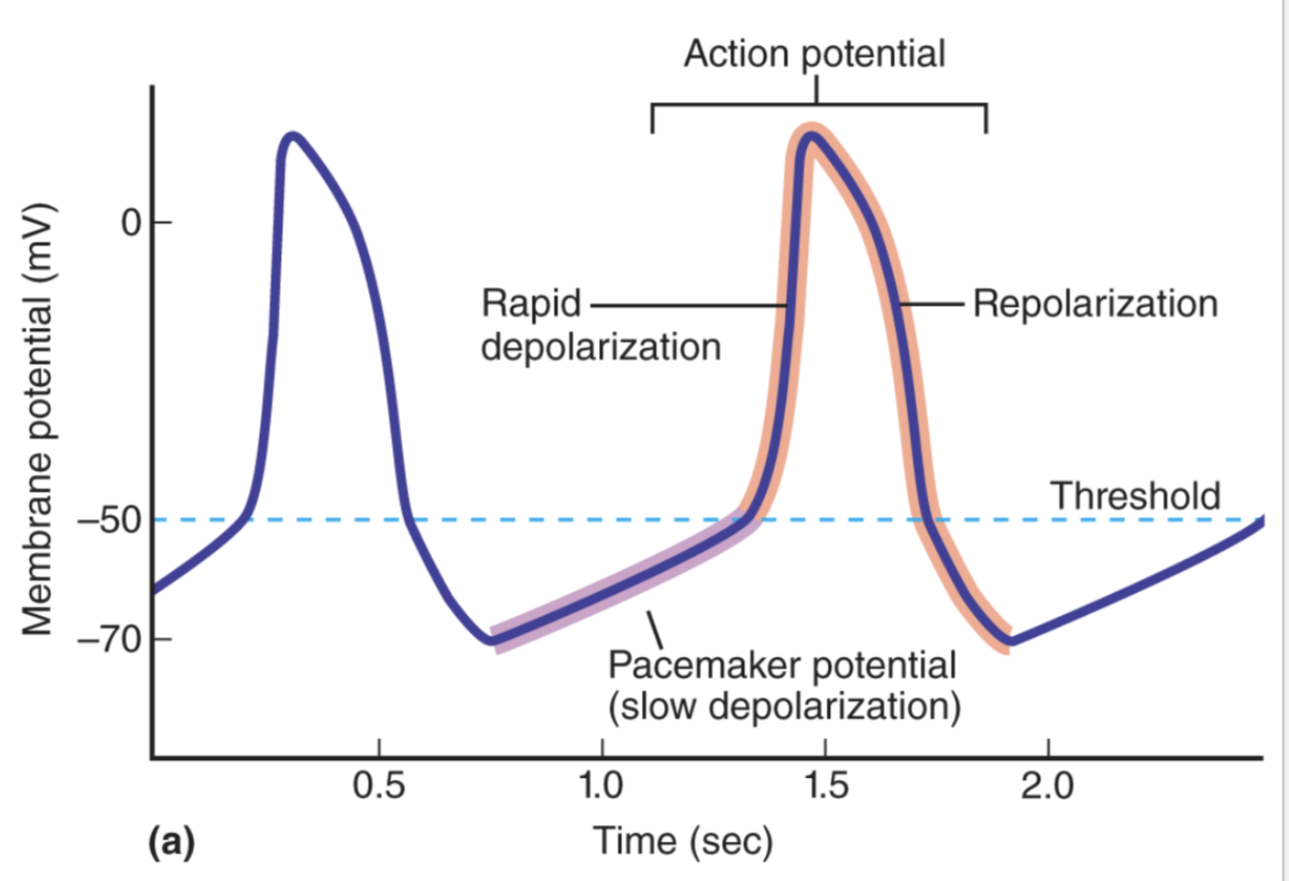
Ion Channel Changes in Pacemaker Cell
Use K, Na, Ca to drive action potential production
Multi step process that changes permeability
- Step 1: Initial spontaneous depolarization, K permeability decreases and Na permeability increases
- Step 2: Later spontaneous depolarization, Ca permeability increases and Na permeability decreases
- Step 3: Rapid depolarization, Ca permeability increases
- Step 4: Repolarization, Ca permeability decreases and K permeability increases
Funny channels
Channels that are are necessary for pacemaker cells to produce and action potential
- Responsible for initial period of spontaneous depolarization
Allows Na to move in and K to move out
- Na moves in at much greater value and depolarized the cell
Open as soon as cell hyper-polarizes to -70mV and closes when the charge nears -55mV
T-type calcium channels
Channels that are are necessary for pacemaker cells to produce and action potential
- Responsible for later period of spontaneous depolarization
Allows Ca to move in
Open as soon as cell hyper-polarizes to -55mV
L-type calcium channels
Channels that are are necessary for pacemaker cells to produce and action potential
- Responsible for rapid depolarization phase of action potential production
Allows large amounts of Ca to move in
Open as soon as cell reaches threshold and close as soon as cell reaches peak of AP
Potassium channels effect on AP production
Channels that are are necessary for pacemaker cells to produce and action potential
- Responsible for repolarization phase of action potential production
Allows large amounts of K to move out of the cell
Open as soon the cell reaches peak of AP and closes when cell has repolarized to -70mV
Refractory in Cardiac Contractile Cells
Long refractory period prevents summation and tetanus
Cardiac Contractile Cell’s response to Action Potential
Multi step process
- Step 0: Depolarization phase
- Step 1: Brief drop in potential
- Step 2: Plateau phase
- Step 3: Repolarization of membrane potential
- Step 4: Resting membrane potential
Depolarization phase
Phase 0 of Cardiac Contractile Cell Action Potential
Na channels open
- Peak of 40mV caused
Brief drop in potential
Phase 1 of Cardiac Contractile Cell Action Potential
Na channels close and depolarization is set in motion
- L calcium channels open and membrane depolarizes
Plateau phase
Phase 2 of Cardiac Contractile Cell Action Potential
Membrane stays in a depolarized state
- K channels stay closed
- Ca channels stay open
Repolarization of membrane potential
Phase 3 of Cardiac Contractile Cell Action Potential
Potassium channels “delayed rectifier channels” open
Inward rectifier channels open
Calcium channels close
Resting membrane potential
Phase 4 of Cardiac Contractile Cell Action Potential
All ions are at resting values
-90mV
Excitation-Contraction Coupling in Cardiac Contractile Cells
AP spreads to cardiomyocyte through gap junctions which causes depolarizes to threshold
- AP triggers opening of voltage-gated calcium channels on SR + PM
Calcium removal from cytosol
- Ca2+-ATPase in SR membrane
- Ca2+-ATPase in PM
- Na+-Ca2+ exchanger in PM
Electrocardiogram (ECG/EKG)
Monitors electrical activity of heart
- Record of the overall spread of electrical current through the heart as a function of time during the cardiac cycle
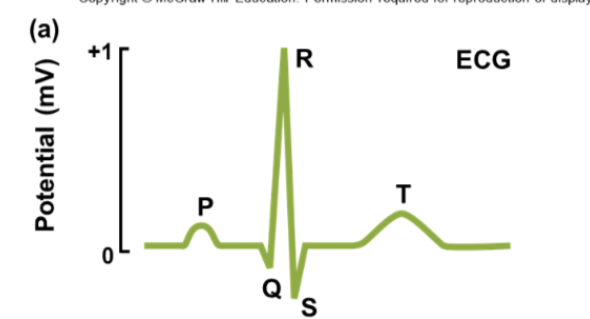
P wave
Part of an electrocardiogram reading
Upward deflection caused by atrial depolarization
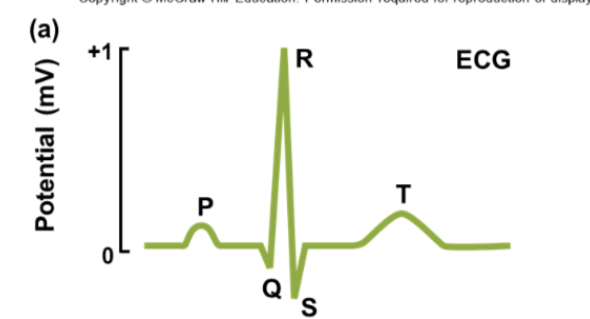
QRS complex
Part of an electrocardiogram reading
Sharp upward and downward deflections, ventricular depolarization
Corresponds to phase 0 of ventricular contractile cell AP
Atrial repolarization occurs at this time but is usually not detected by ECG
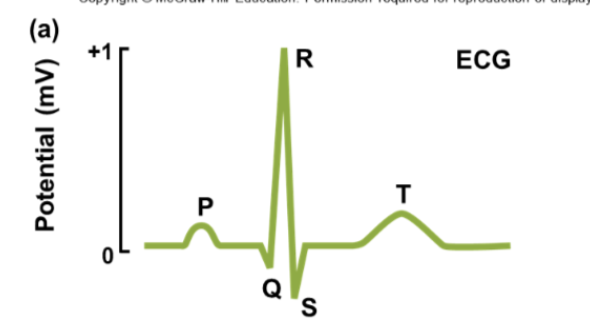
T wave
Part of an electrocardiogram reading
Upward deflection, ventricular repolarization
Corresponds to phase 3
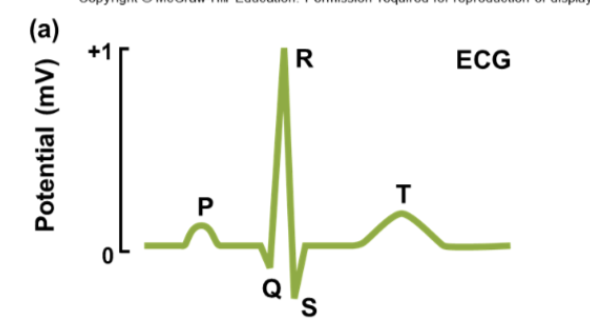
Isoelectic line
Part of an EKG
Horizontal line between waves, no electrical activity occurring
P-Q/P-R interval
Between onset of P wave and onset of QRS complex
Estimate of time of conduction through AV node
Atrial systole
Q-T interval
From onset of QRS complex to end of T wave
Estimate of time ventricles are contracting
T-Q segment
From end of T wave to beginning of QRS complex
Estimate of time ventricles are relaxing
R-R interval
Between peaks of two successive QRS complexes
Time between heartbeats
Bradycardia
Slow heart rate
- Below 50 bpm
Tachycardia
Fast heart rate
- Above 100 bpm
Ventricular tachycardia
Increased rate of contraction in ventricles
Leads to ventricular fibrillation and death
Flutter
Extremely fast (200 to 300 bpm) but coordinated contractions
Fibrillation
Uncoordinated pumping between two similar heart valves
- Either both atria’s or both ventricles
Atrial fibrillation
Atrial muscle fibers depolarize independently
- Not deadly as long as ventricular contraction remains functional
Ventricular fibrillation
Ventricular muscle fibers depolarize
independently → blood cannot be efficiently pumped to tissues
Defibrillation: apply large external current to depolarize all muscle cells at the
same time & return synchronous electrical activity to heart
Chordate tendineae
Tendons that extend from the ventrals to the AV valves
Pull downward on the valve cusps to preventing the AV valves from being pushed into the atria (prolapsing)