Lecture 2: History of Clinical Neuropsychology
1/16
Earn XP
Description and Tags
mi-am bagat picioarele in capitol
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
clinical neuropsychological disorder
Condition that arises directly from abnormalities/dysfunctions within the brain's biological structures and processes
Condition that is shaped and defined by social, cultural and environmental contexts
Clinical neuropsychology both establishes phenomena and finds mechanistic explanations for them.
Clinical neuropsychology is shaped by philosophical and scientific angles, careful observation from case studies, development of systematic assessment.
history overview
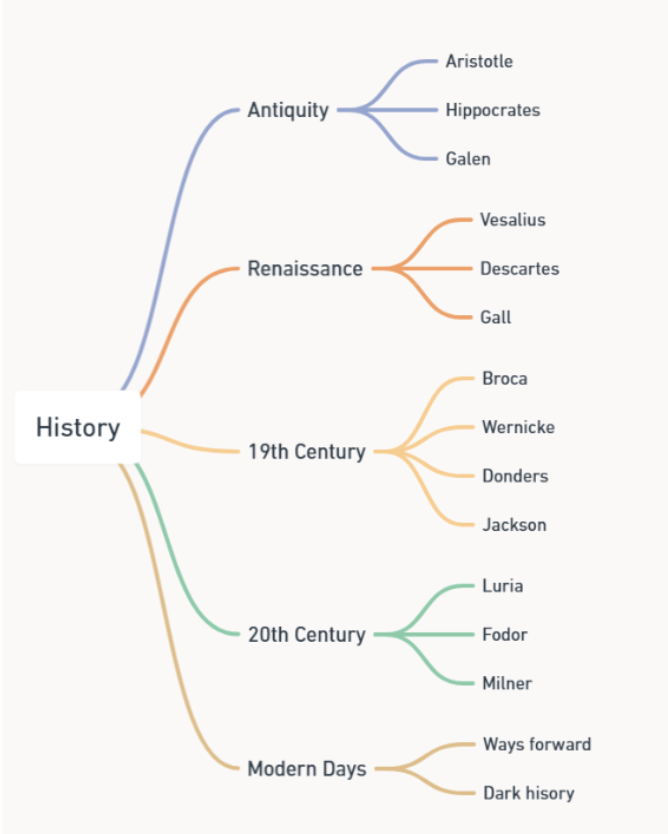
antiquity
Antiquity (500 BCE – 500 CE): philosophy and empiricism
Aristotle: highly influential thinker; "heart is the seat of intelligence", "brain cools the body", compared different animals
Hippocrates: father of modern medicine, "brain is for mental functions", pioneered lesion observations
Claudius Galen: pioneered dissection and comparative anatomy in mammals, mapped ventricular system ("animal spirits") and nerves, "morosis" (dementia)
neuropsychology before the Renaissance
gross anatomy established, some idea that the brain is important for mental function, no specific theory of brain-behaviour relationships.
Little progress because of: notion that the soul had no physical basis, forbidden to experiment on humans, scientific method not fully established, exchange of ideas limited
Renaissance
Renaissance (1400–1700): scientific method! soul gets localised!
Vesalius: founder of modern human anatomy, systematic human dissections, detailed descriptions and drawings, corrected Galen's anatomical errors
René Descartes: shaped mind-body dualism, viewed body as a machine, influenced empirical physiology
Franz Joseph Gall: shaped idea of localisation, developed phrenology.
neuropsychology before the 19th century
more knowledge about structure of brain, relationship between brain and behaviour still unclear, no conceptual framework tying both together, views heavily influenced by religion and politics
neuropsychology in the 19th century
Neuropsychology in the 19th century: brain mapping! Language areas!
Paul Broca: established methods of behavioural observation and post-mortem anatomy; identified a critical area of language production
Monsieur Leborgne: patient of Paul Broca, severely affected language production: aphasia; good language comprehension; lesion in left frontal lobe (Broca's)
Carl Wernicke: identified critical area for language comprehension (left superior temporal gyrus), established idea of disconnection aphasia.
Fransiscus Donders: Dutch ophtalmologist, simple choice and go/no go reaction time tasks, subtraction method
John Hughlings Jackson: British neurologist, studied mostly epilepsy, Jacksonian March (type of simple focal aware seizure that begins in one small part of the body—typically the hand, foot, or face—and "marches" or spreads to adjacent areas); hierarchy in nervous system; higher brain regions control and inhibit lower ones; positive and negative symptom distinction
neuropsychology in the 20th century:
20th century: development of Neuropsychology tests, guns (?), strict localisation fades away
Guns and rifles: WW1,2: large-scale Npsy assessment
Army Alpha, Army Beta: the first widely administered group intelligence assessments, used to classify 1.5–1.75 million World War I recruits
Trail Making Test, Wechsler IQ
WW2: high velocity weapons, better healthcare; generation of brain-injured patients, studying brain-behaviour relations
Aleksandr Luria: studied soldiers with brain injuries, pioneered systems view of brain function, developed a comprehensive assessment battery, rehabilitation protocols for brain injury
Jerry Fodor: philosopher, huge influence on cognitive science, neuroscience, AI; proposed idea of modularity of mind:
Brenda Milner: uncovered brain basis of memory through work with HM, established dissociations between different aspects of memory (STM vs LTM; procedural vs declarative)
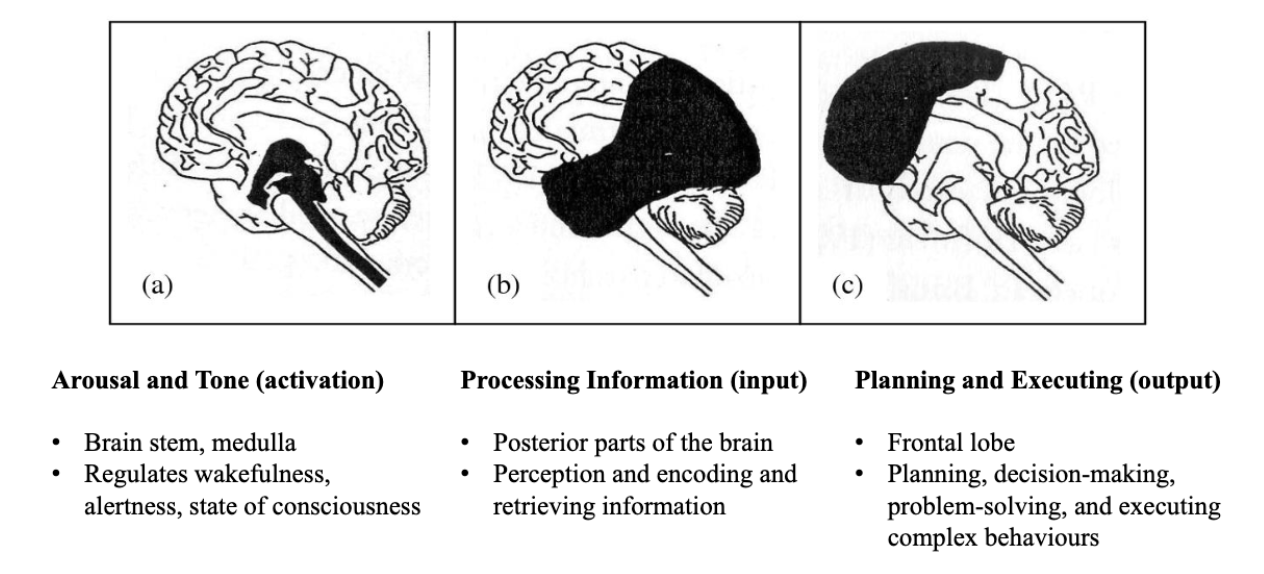
Aleksandr Luria
Luria's functional units: see picture
Luria's hierarchical organisation: hierarchical processing within each functional unit
Primary zone: input
Secondary zone: processing
Tertiary zone: integration other areas
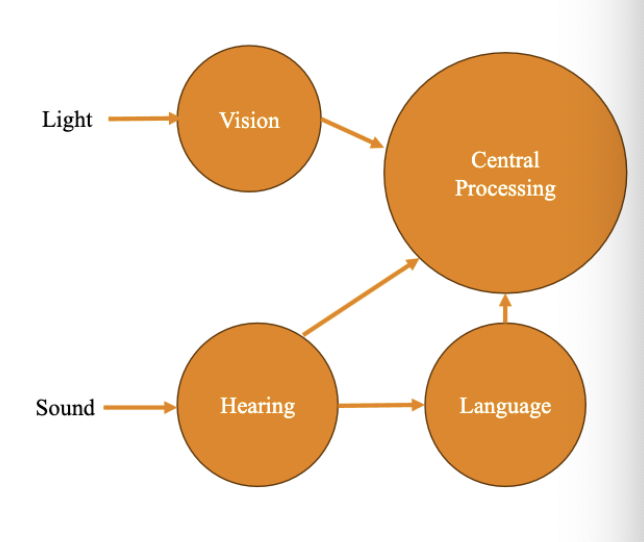
Jerry Fodor
Characteristics of modules:
Process only specific inputs
Operate automatically
Are informationally encapsulated
Process information quickly
Have fixed neural architecture
Different systems:
Input systems: modular (perception, language)
Central systems: not modular (reasoning, decision making)
neuropsychology after the 20th century
Fodor and Luria complementary perspectives on brain function (Fodor: useful for what broke and why; Luria: what to do next) - still debated: localisation vs plasticity;
present day neuropsychology
diaschisis, compensation, individual differences, cognitive reserve
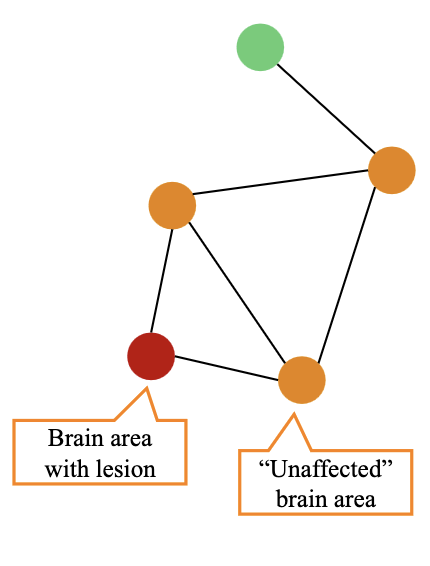
diaschisis
Diaschisis = brain injury/disease may have more widespread effects:
Differences in organisation may influence information processing streams
Connections may affect transfer between areas (axonal lesions)
Differences in synchronisation may affect communication
compensation
test performance doesn't necessarily reflect disrupted processing of a damaged mechanism; tasks can be performed using different strategies; patients can learn to adapt (use diff pathways to perform the same task)
individual differences
variation in typical brain anatomy and physiology (Broca's cannot be identified on the basis of morphology in 20% of typical population, despite typical language function)
cognitive reserve
way of explaining individual differences
Brain reserve: structural capacity
Cognitive reserve: how flexibly and efficiently the brain is used; shaped by life experiences (education, occupation, leisure activities):
Neural reserve: efficiency of existing networks
Neural compensation: recruitment of alternative networks when primary ones fail
dark history🥀
experimentation without consent, using experimental medical procedures, racial and class judgement, misuse of assessments
We should: informed consent, independent ethical review, monitored guidelines for introducing new treatments, more inclusive research, incorporating theories from other disciplines and cultures