PHTY2101 Module 4 - Burns
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
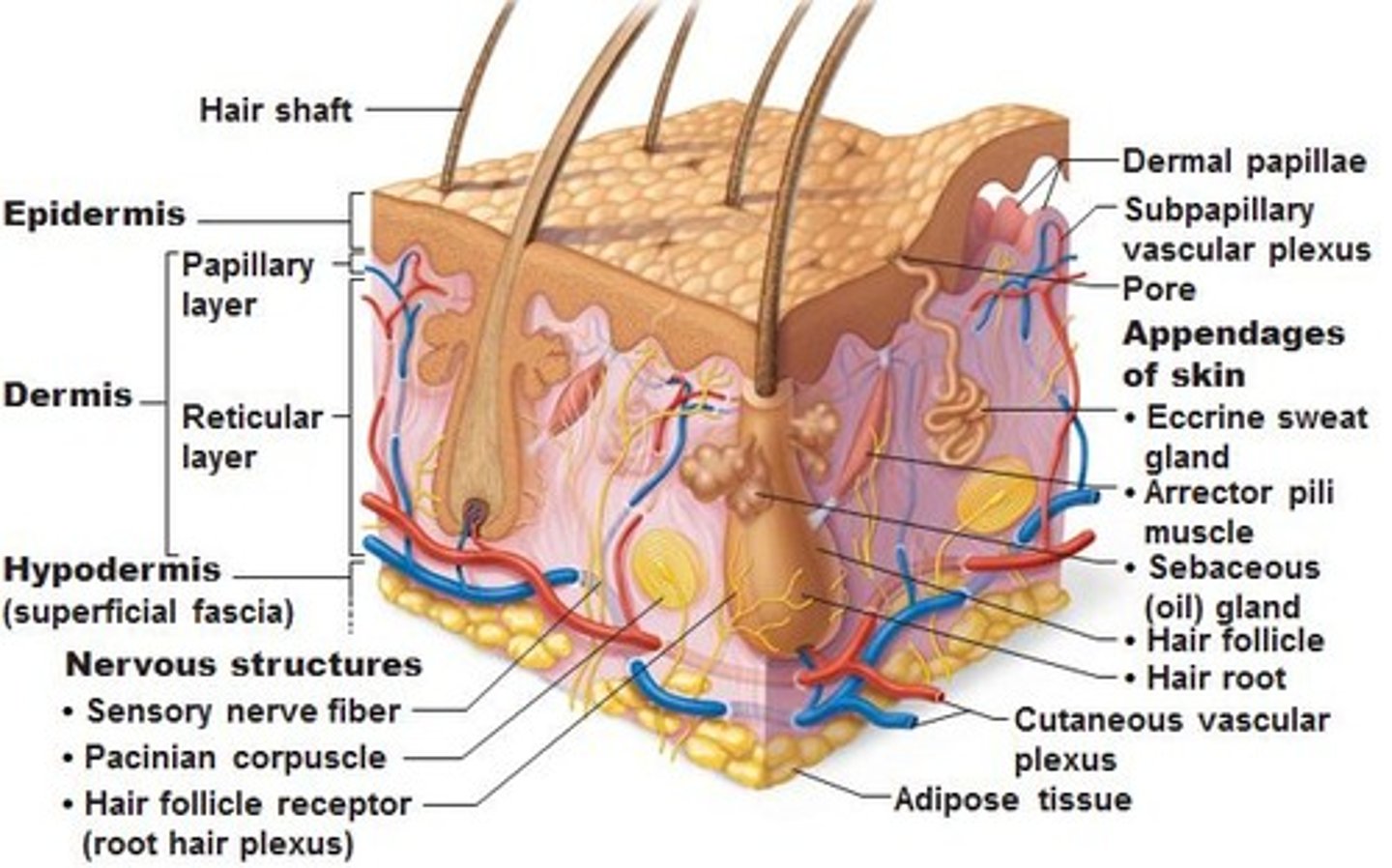
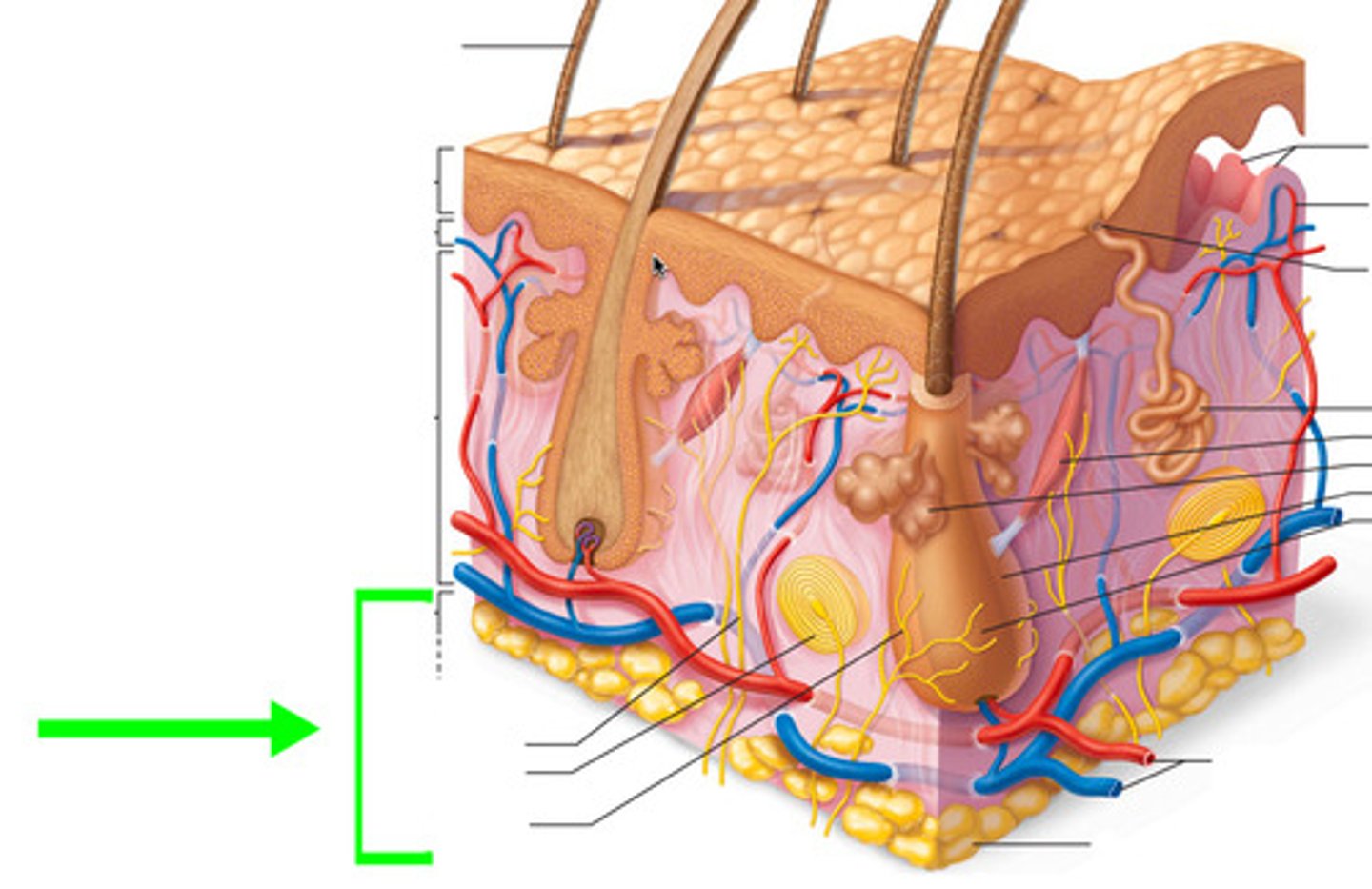
identify 3 layers of the skin in order of superficial to deep
1. epidermis
2. dermis
4. hypodermis
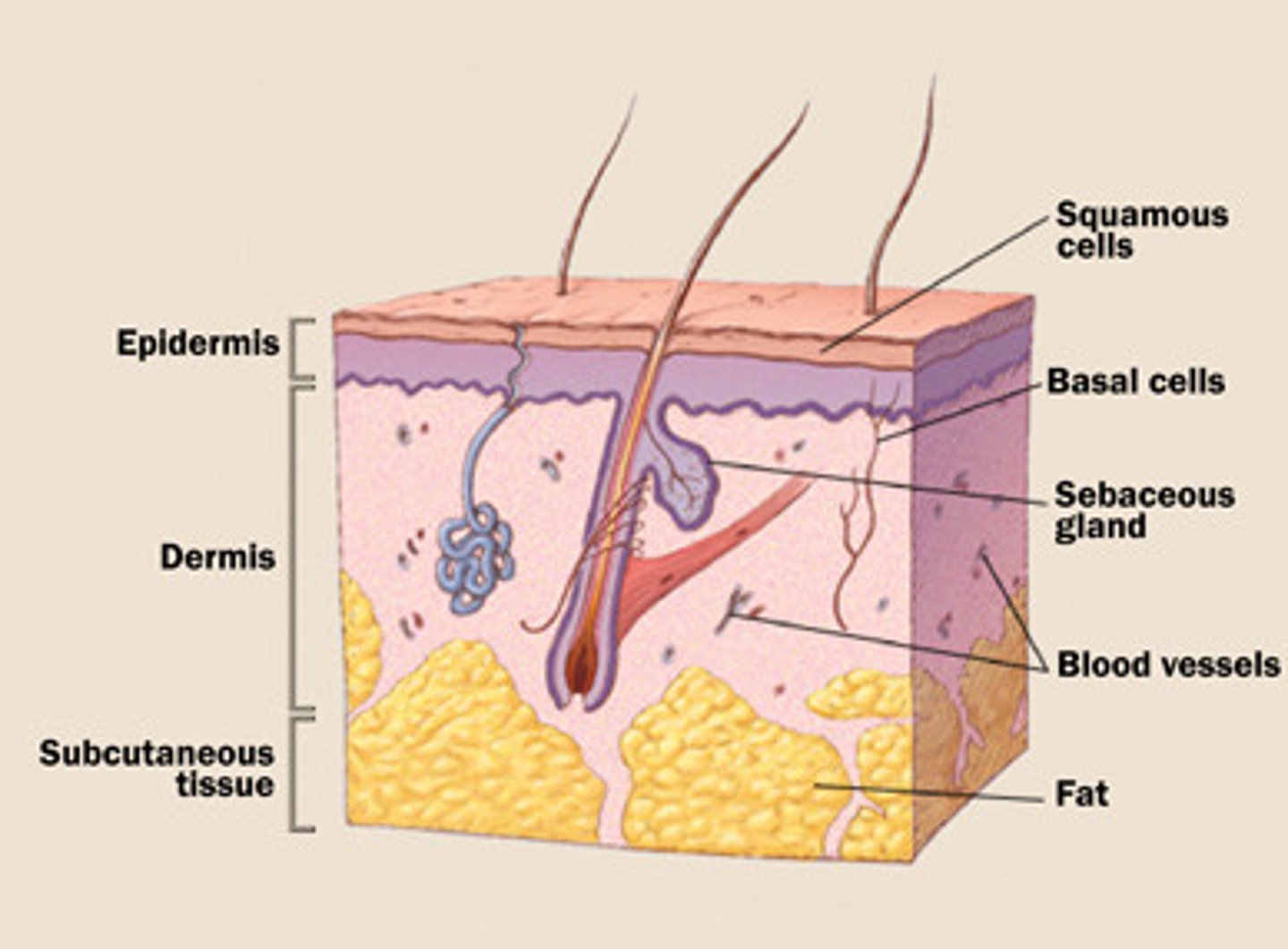
describe the epidermis (5 points)
1. superficial protective layer
2. keratinocytes produce keratin for toughness and waterproofing
3. melanocytes produce melanin for UV protection
4. has 'rete pegs' for attachment to dermis and epidermal appendages (hair, glands etc)
5. no blood vessels
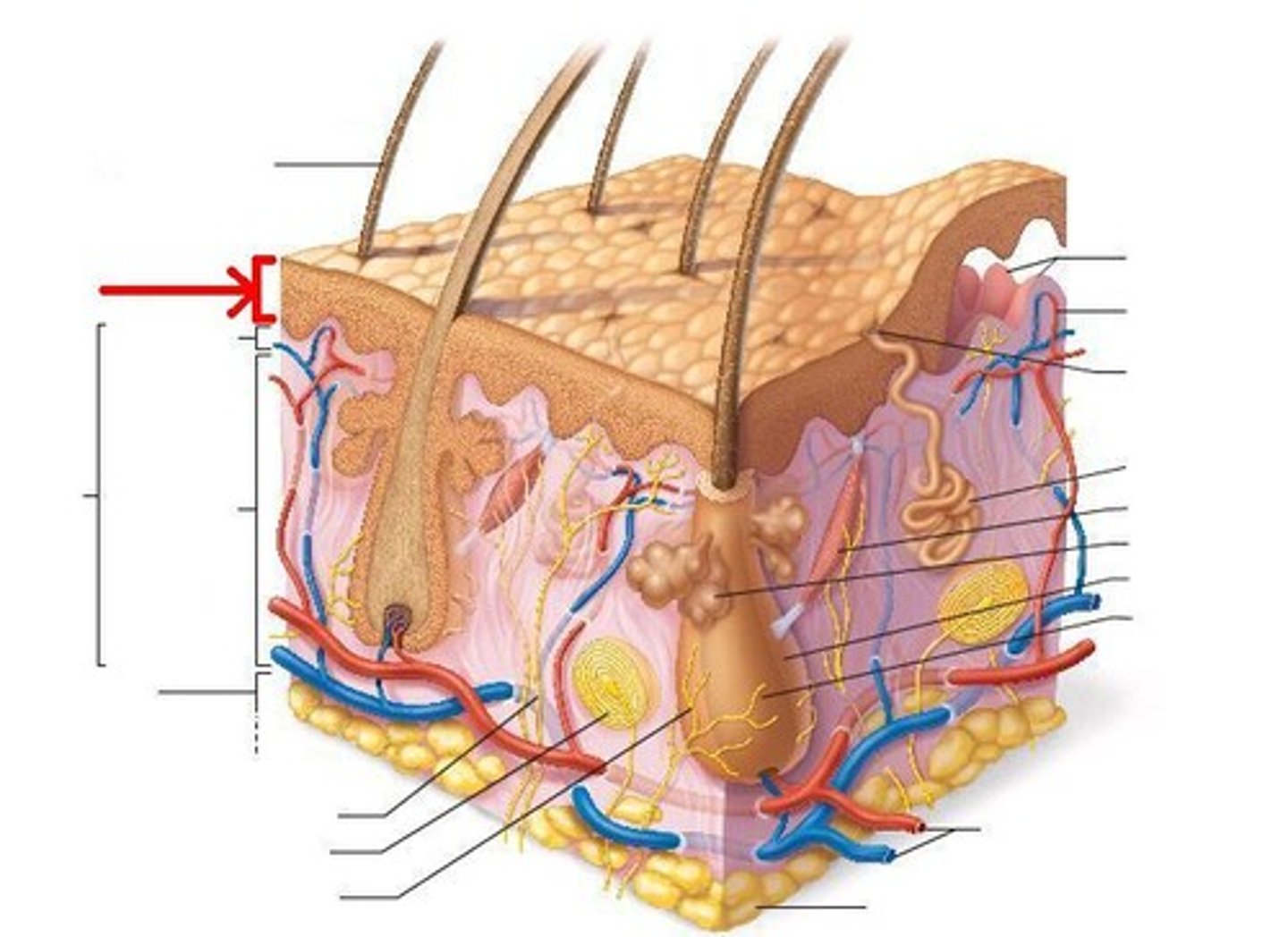
describe the dermis (4 points)
1. has 2 layers - papillary (superficial) and reticular (deeper)
2. vascularised, innervated, and has lymphatics
3. has elastin fibres and collagen
4. provides mechanical strength of skin
5. all structures in dermis surrounded by ground substance
what is ground substance
a semi-fluid matrix that lubricates cells during stretch and acts as a buffer during recoil, made up of glycosaminoglycans and proteoglycans
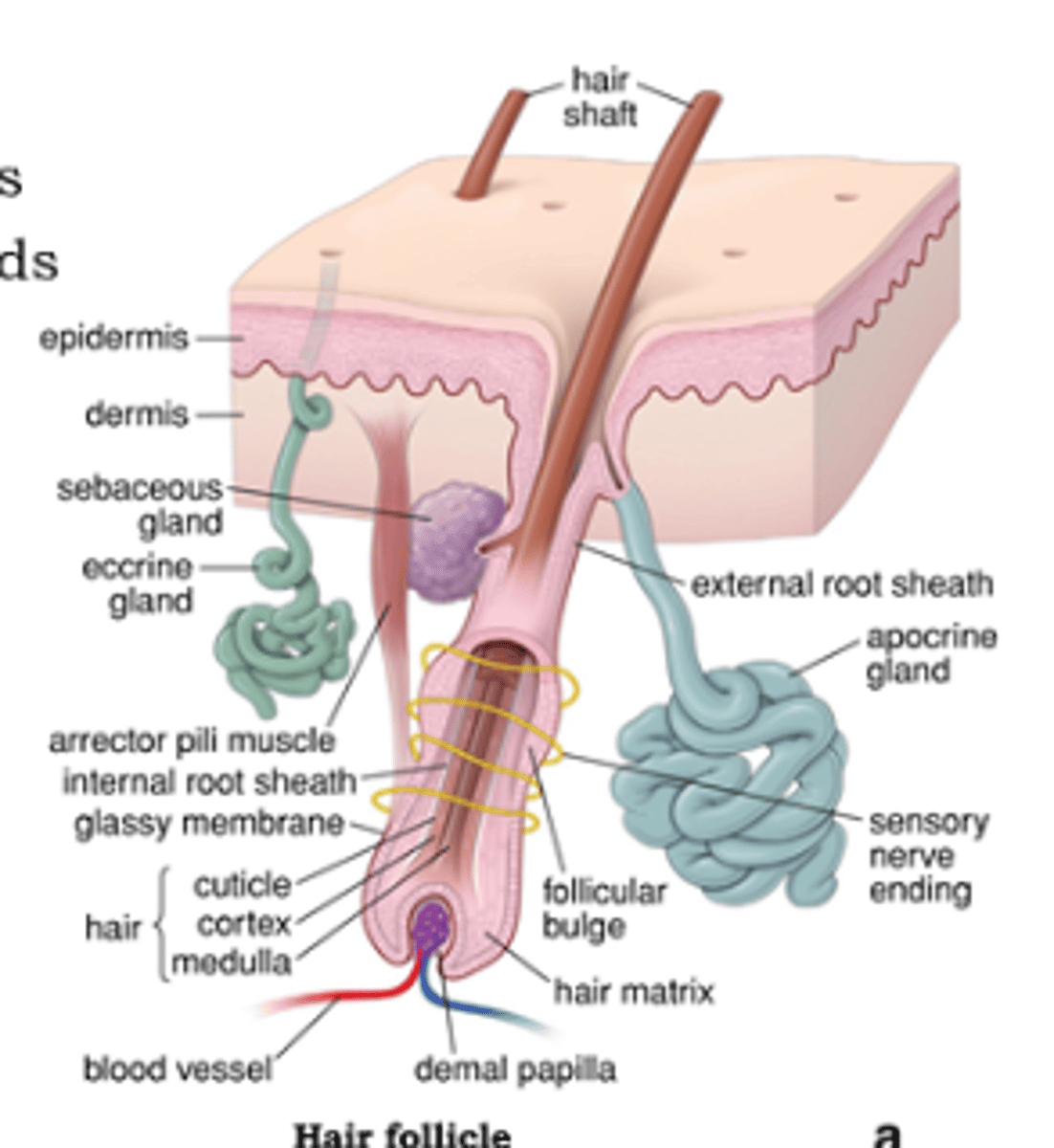
describe epidermal appendages (4 points)
1. consist of hair follicles, sweat glands, sebaceous glands
2. start deep in epidermis and extend outwards
3. surrounded by epidermal cells and a rich network of capillaries
4. are the centre of regeneration of epidermis
describe the hypodermis (3 points)
1. deepest layer
2. made of subcutaneous fat and fascia
3. vascularised, innervated, etc
describe glabrous skin - where is it
hairless skin
- thick epidermis with additional layer (stratum lucidum) which helps regeneration
- palms, soles of feet, lips, genitals
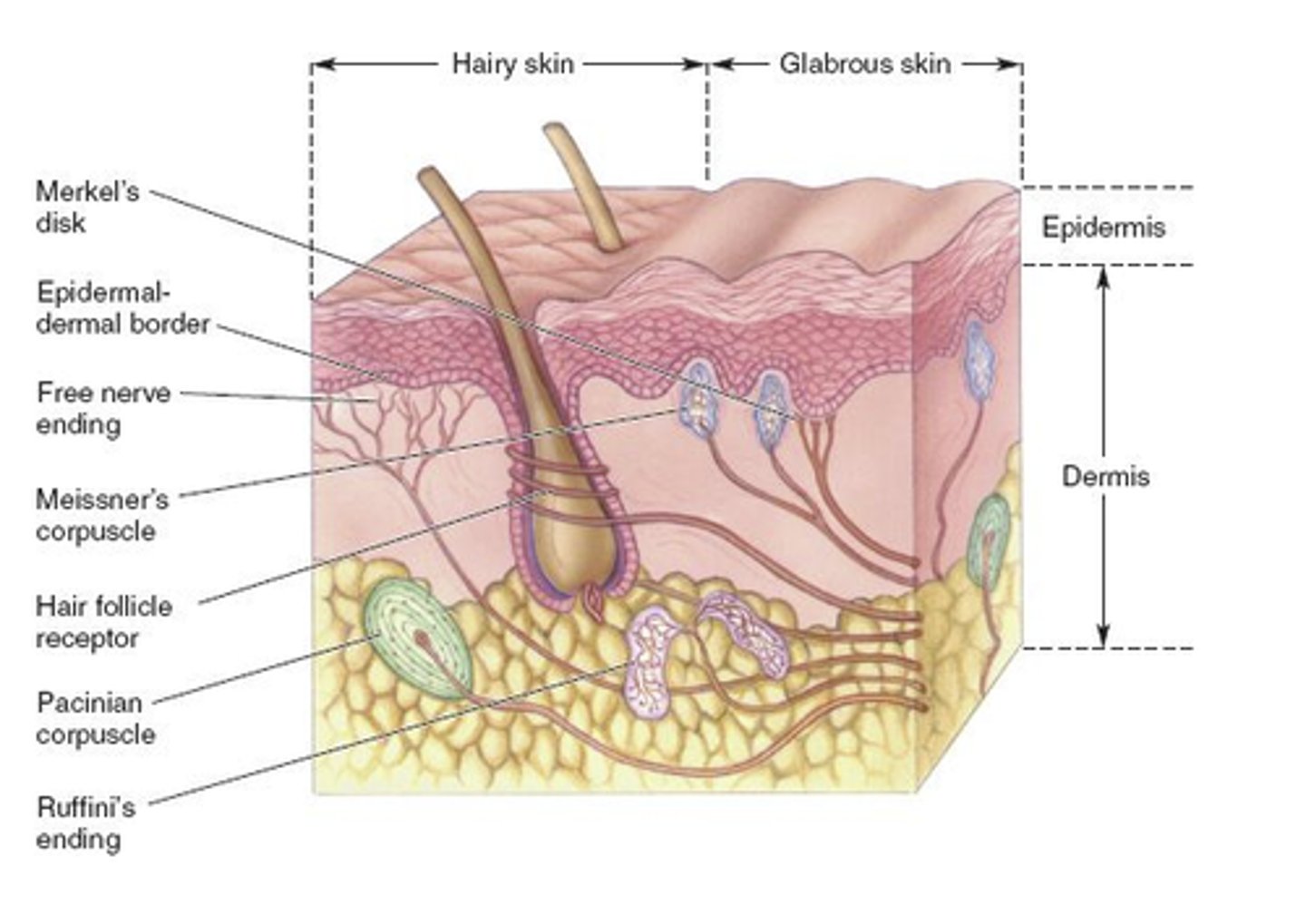
two types of skin classificaiton
1. hairy vs glabrous
2. thick vs thin
where is thick skin, where is thin skin
thin = eyelids
thick = palms, soles, back
2 differences between hairy and glabrous skin
1. hairy has hair follicles, glabrous doesn't
2. hairy has thin epidermis, glabrous has thick epidermis
describe Fitzpatrick Skin Type Scale
- numerical classification for skin colour
- rating (0-40) considered amount of melanin in skin (colour) and therefore tolerance to sunlight/burning
- score out of 40 scales down to 6 types (score 0-6 = type 1 etc)

what types of Fitzpatrick Skin Type Scale have highest risk to scarring
type 1, 5, 6
identify 7 functions of the skin
1. sensation
2. barrier to water loss/evaporation
3. temperature control
4. infection defense
5. maintains moist internal environment
6. pigment protection from UV
7. produces vitamin D
what are 2 consequences of impaired skin sensation
1. hypersensitivity
2. decreased sensation -> risk of further damage
what is 1 consequence of impaired ability for skin to prevent water loss
increased evaporation => renal complications
how does skin regulate temperature
- heat dissipation through conduction, convection, radiation
- sweat glands and evaporation
what are 3 consequences of impaired skin temperature control
1. metabolic disturbances
2. fluid balance disturbances
3. overheating or too cold
identify 3 classifications systems for burns
1. MOI
2. depth
3. size
identity the 4 types of burn MOI
1. flame
2. scald (hot water)
3. work-related (flame, chemical, electrical)
4. other (friction, contact, radiant heat, pressurised gas)
most common type of burn in adults
flame
most common type of burn in paediatrics and elderly
scald - hot water
identify 4 depths of burns
1. superficial
2. superficial dermal (superficial partial thickness)
3. deep dermal (deep partial thickness)
4. full thickness
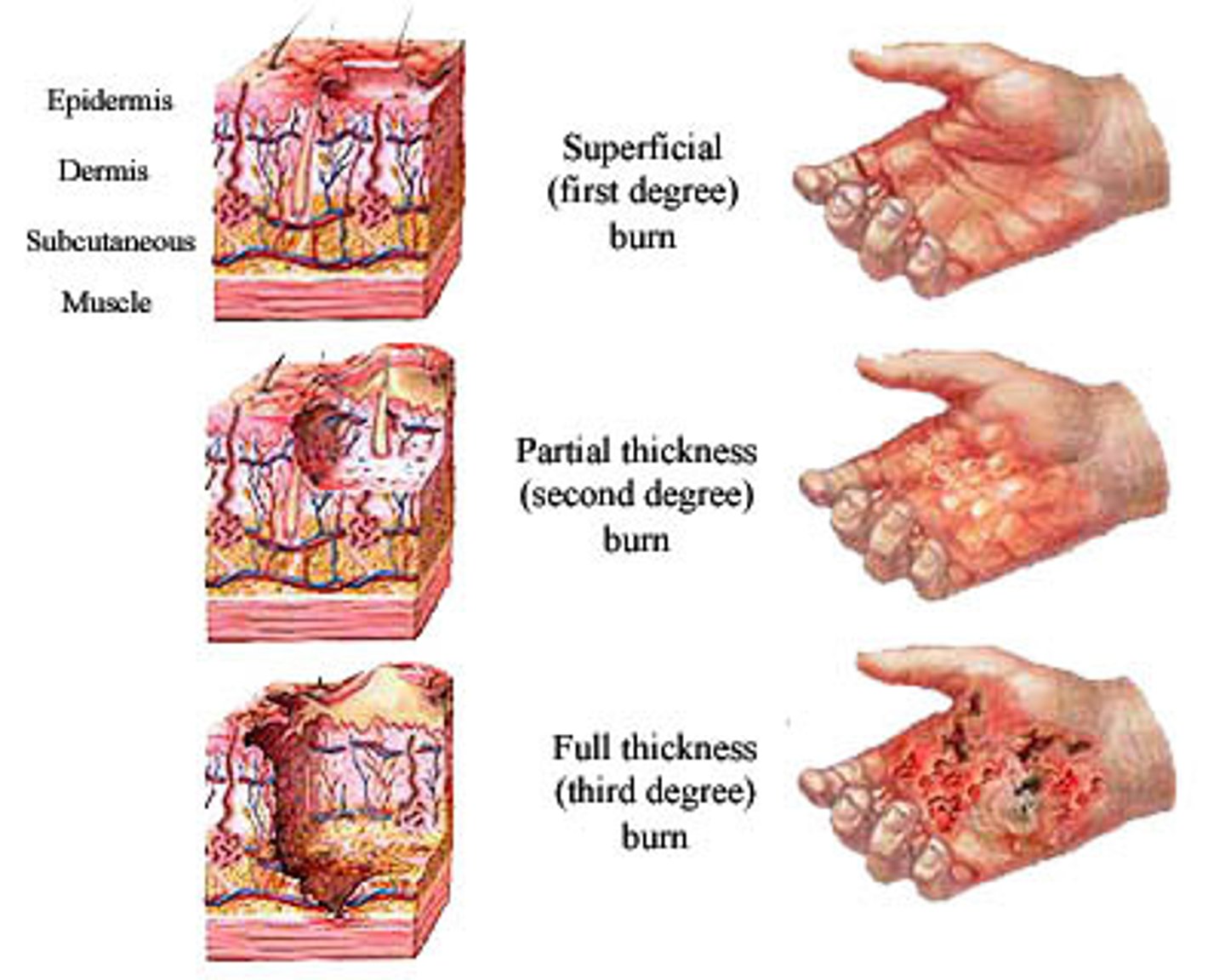
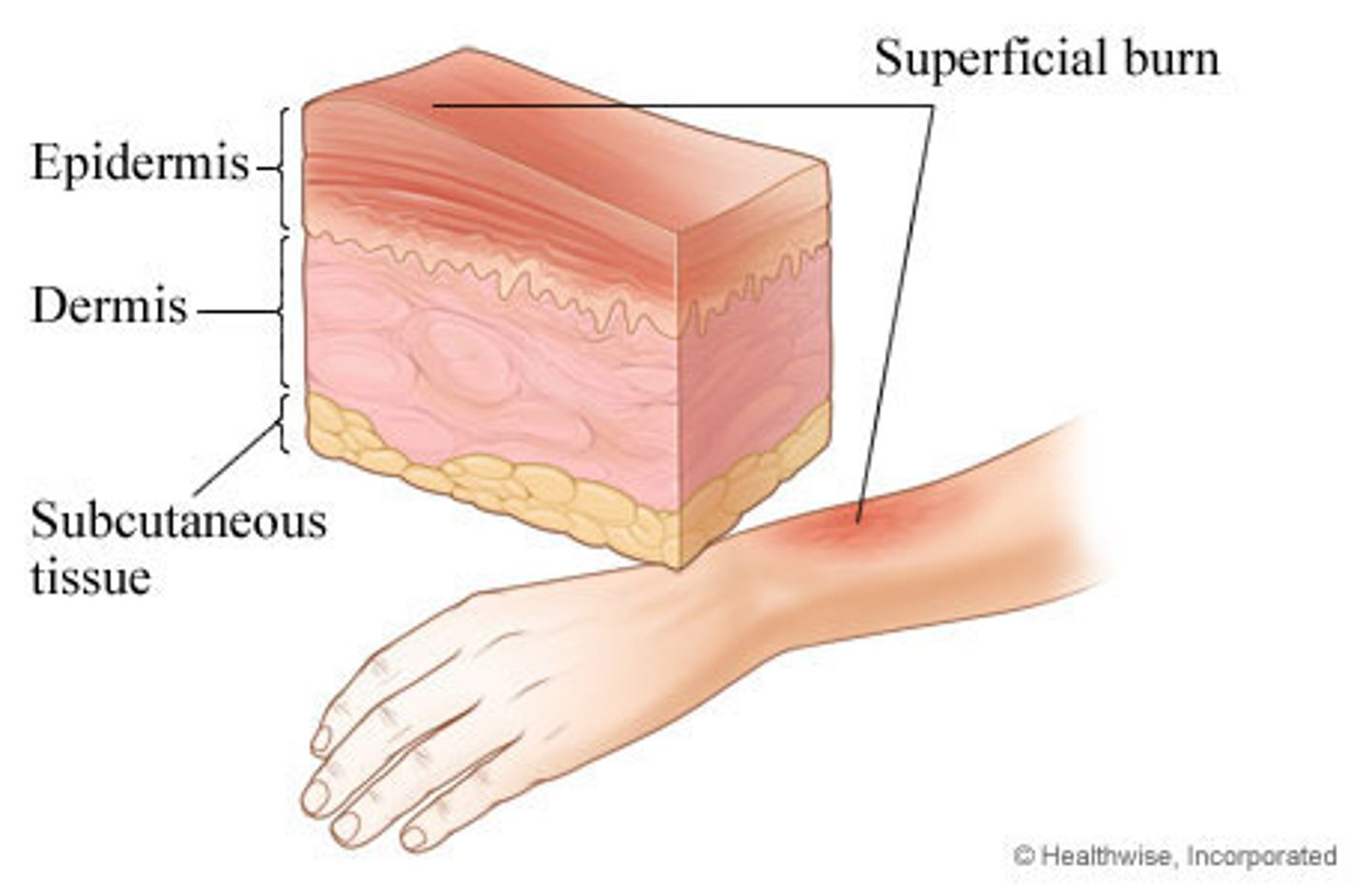
describe a superficial burn (5 points)
1. areas destroyed = epidermis
2. appearance = red and blistered
3. sensation = intact or hypersensitive
4. blanching/capillary return = rapid (intact circulation)
5. wound closure = spontaneously in 7-10 days
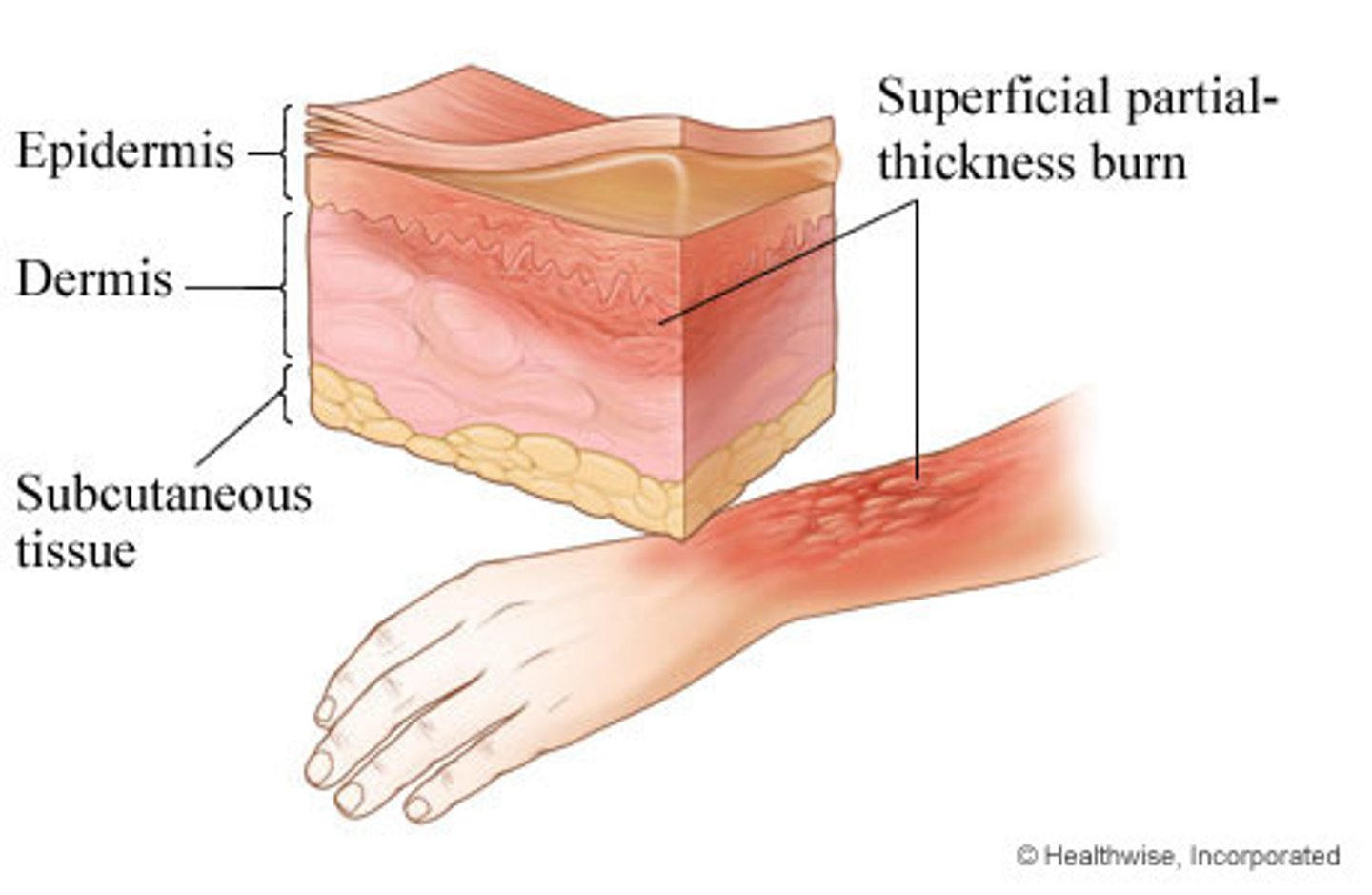
describe a superficial partial thickness burn (5 points)
1. areas destroyed = epidermis + superficial dermis
2. appearance = red/pink, blistered
3. sensation = intact, hypersensitive, painful
4. blanching/capillary return = rapid (intact circulation)
5. wound closure = spontaneously in 14 days
describe a deep partial thickness burn (5 points)
1. areas destroyed = epidermis + full dermis
2. appearance = creamy, white, moist, may have pseudo-membrane and oedema
3. sensation = intact but may have decreased light-touch (some nerve endings damaged)
4. blanching/capillary return = delayed but present
5. wound closure = >14 days, may need graft

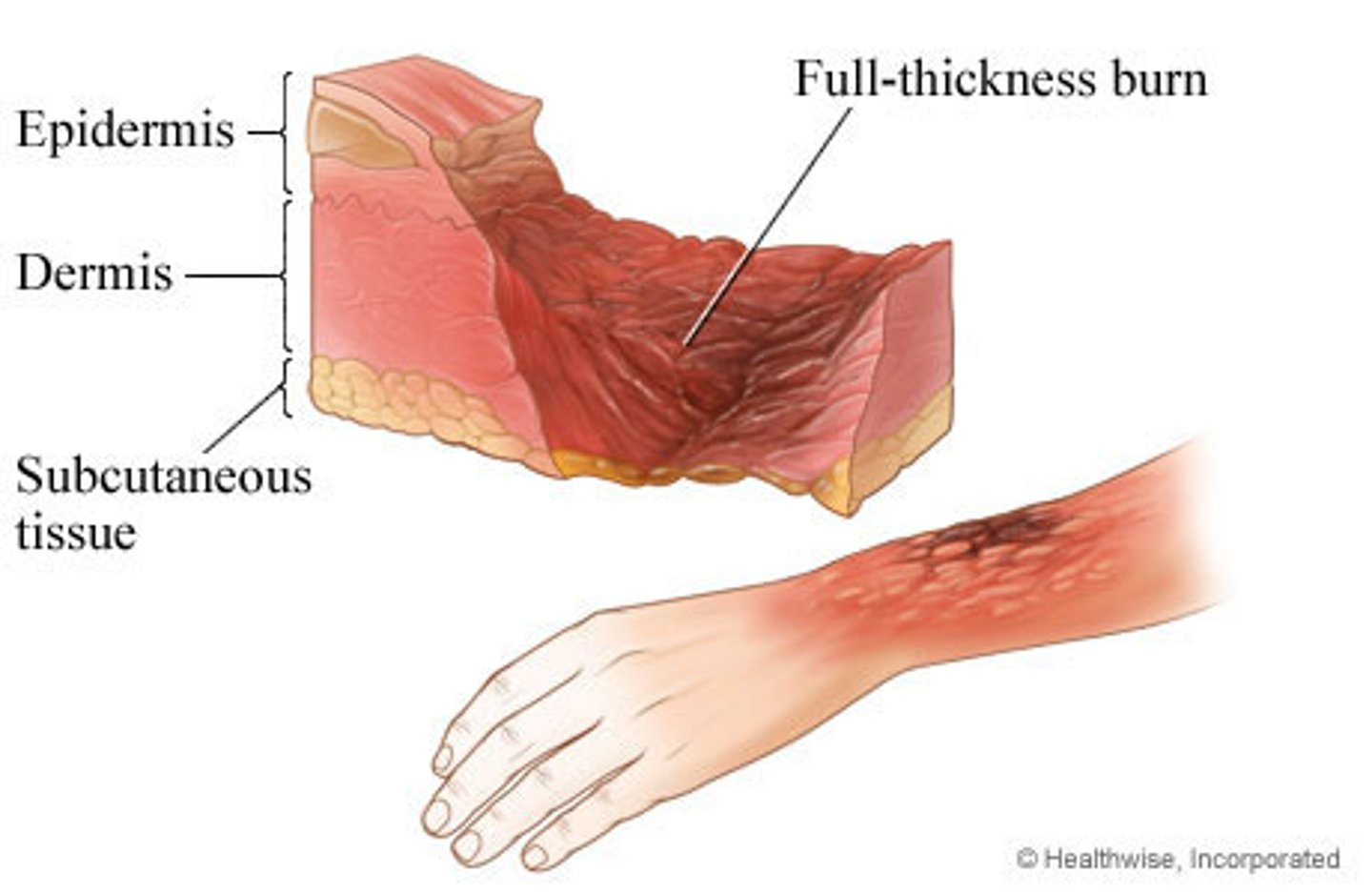
describe a full thickness burn (5 points)
1. areas destroyed = epidermis + dermis + underlying structures
2. appearance = dry/leathery, colour is MOI dependent
3. sensation = no light touch to skin, underlying sensation from muscles
4. blanching/capillary return = none
5. wound closure = requires graft, >3 weeks
how is size of burn calculated
total body surface area (%TBSA) either through 'rule of nines' by paramedics or on Lund and Browder chart in hospital
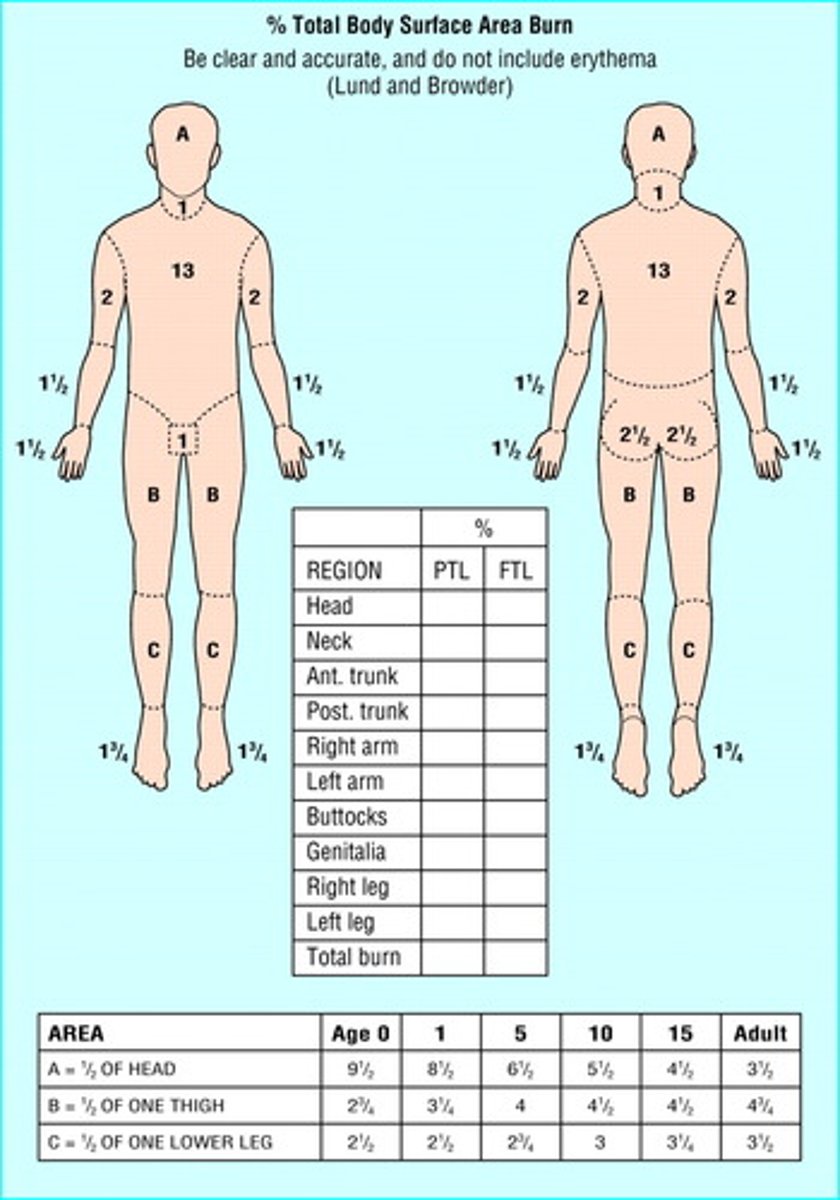
why is %TBSA useful for burns
accurate calculation of fluid replacement required
7 types of burns that need to be referred to Major Burns Unit
1. >10% TBSA or full thickness > 5%
2. special areas - face, hands, feet, genitals, major joints
3. electrical or chemical burns
4. associated inhalation injury or trauma
5. circumferential burns of limbs or chest
6. paediatric or elderly patient
7. pre-existing medical disorders that could complicate
identify the 3 stages of burn healing and timeframe
1. inflammatory (1-5 days)
2. cell proliferation (3 days - 3 weeks)
3. remodelling (3 weeks - 18 months)
describe cell proliferation phase of burn healing (4 points)
1. fibroblasts - synthesise collagen and ground substance to give wound strength and provide matrix for cell proliferation
2. fibroblasts differentiate into myofibroblasts - contractile cells that pull wound edges together until wound is closed but may cause contracture by continuing process after closure
3. keratinocytes - proliferate and mobilise across wound surface to make epithelial tissue
4. scar tissue forms
describe dermis and epidermis organisation in a scar
- demis is made of disoriented collagen
- epidermis lacks interconnection with dermis
- more prone to abrasion
describe remodelling phase of burn healing (5 points)
1. collagen cross-links increase tensile strength over 1 year
2. ground substance becomes more dense and bony
3. continual collagen synthesis and degradation (synthesis outweighs degradation)
4. collagen becomes more parallel with mechanical stress
5. myofibroblast number peaks around 4-5 months
what timeframe of healing are less/more likely to produce scarring
<2 weeks = usually no scarring
2-3 weeks = moderate scar
>3 weeks = significant hypertrophic scar + contracture + decreased function
how does a hypertrophic scar form - what is the timeframe
- excessive haphazard collagen deposition with reduced cross linking (reduced skin strength) and changes in granulation tissue and ground substance
- develops within 1-3 months post-injury, progresses for 3-6 months, gradually regresses over time

describe and explain appearance 6 characteristics of hypertrophic scars
1. remains within border of injury (differs from keloid)
2. red - increased blood supply
3. thick/raised = build-up of granulation tissue
4. less pliable - minimal regeneration of elastin
5. more bony/rigid - denser ground substance
6. reduced skin stretch - constant contraction via myofibroblast activity and adhesion to underlying structures
identify 6 risk factors for burn scarring
1. race - skin type 1, 5, 6, and Asian and African skin types
2. site of burn- more risk at head, hands, neck, axilla, joints
3. depth - deeper = longer healing = increased risk
4. conservative healing > 21 days
5. more surgical procedures and more TBSA
6. age/sex: risk for children > adults > elderly. Female > male
identify 5 EARLY management techniques hospitals use for burns
1. escharotomies
2. nutritional support (feeding tube)
3. plan for management - conservative, debridement or graft
4. pain management
5. DVT and ulcer prophylaxis
types of pain management used for burns
1. long acting for background pain e.g. MS Contin
2. short acting for procedures or physio e.g. morphine
3. Gabapentin - burning or neuropathic pain
describe a escharotomy
incision through eschar (dead tissue) relieves pressure and improves tissue perfusion in muscle compartment
what are indications for an escharotomy
- circumferential burns around limbs/chest
- paraesthesia/loss of function
- decreased capillary refill or peripheral pulses
- compartment 'feels tight' (pressure >25mmHg)
- increased ventilatory pressures
when would an escharotomy extend into a fasciotomy
- if pressure is not corrected from just escharotomy
- more common in electrical burns because they go through the body
describe conservative burn management
- Silver based dressings - cloths or creams - which provide antibacterial effects and promotes wound healing.
- cloths stay intact for 3-7 days and creams are changed daily
- may be used in interim before surgery
identify 5 types of skin grafts in order of severity of wound
1. autograft
2. cultured autologous keratinocytes
3. homograft
4. skin substitutes
5. flaps
describe how autografts are taken
- burn wound bed is debrided to viable tissue
- donor skin taken from another area of your own body
- donor site is usually thigh, takes 2 weeks to heal, doesn't scar much
describe the two types of skin preparation for skin grafts
meshed or non-meshed
- meshed = machine puts holes in skin to allow it to stretch over wound.
- non-meshed = no holes
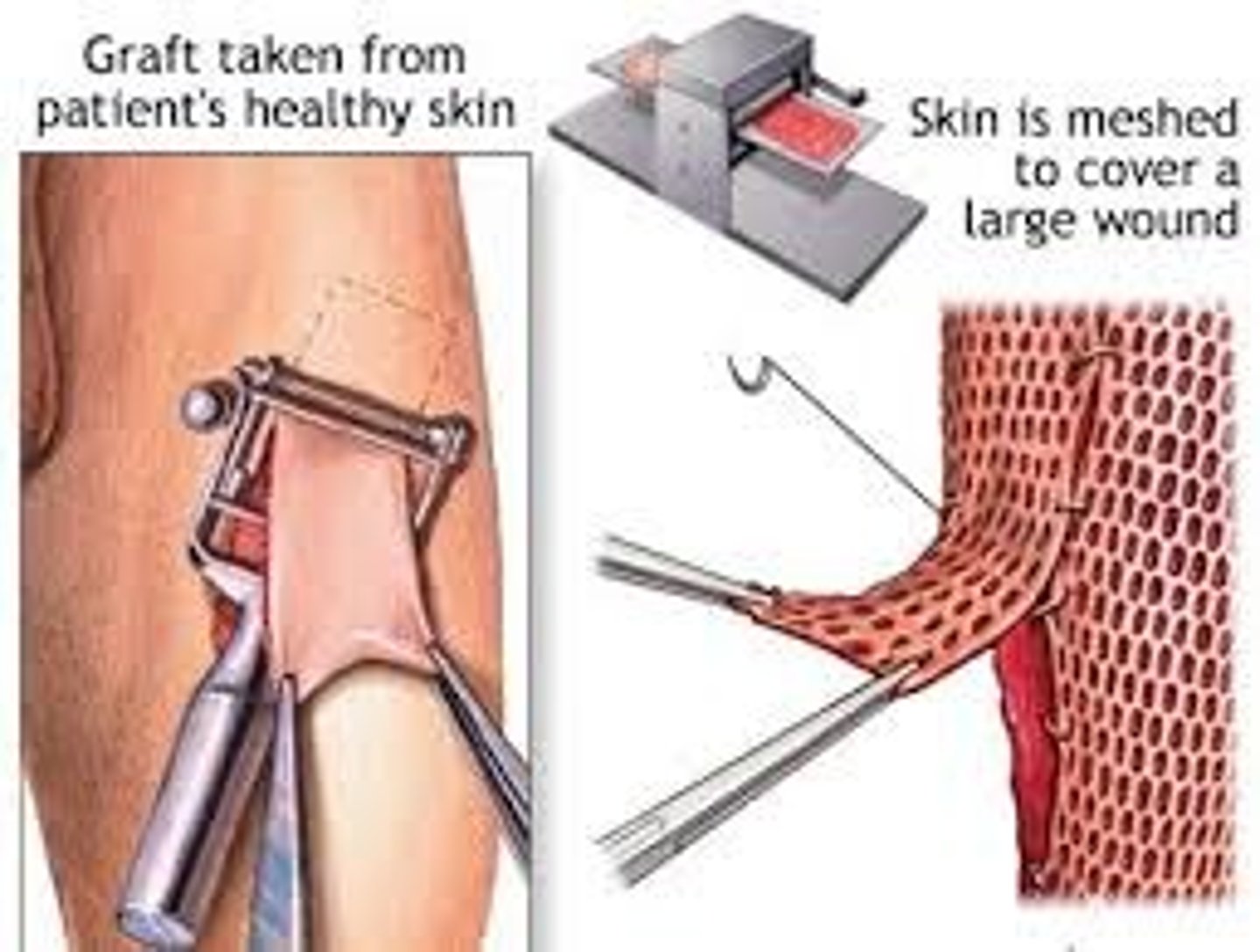
what are advantages and disadvantages of meshed vs non-meshed skin grafts
meshed = better earlier take of graft as exudate can come out through holes, but always leaves mesh-pattern which is worse cosmetically
non-meshed = better cosmetically and used for face and hands, but more fragile in early stages, needs to be pricked by nurses to allow exudate to escape
two types of donor skin for skin grafts
split thickness - just epidermis and some dermis, heals spontaneously <2 weeks
full thickness - all layers of dermis, donor needs to be covered with its own split thickness graft

describe appearance of a well-taken skin graft
pink colour, securely adhered, blanches with pressure
describe timeline of revascularisation of (normal) skin graft
first 48 hours = plasmatic imbibition (yes imbibition) = wound receives nutrition by absorbing plasma from capillaries
48-72 hours = anastomoses of vessels in graft bed, growth of new endothelial buds
complete revascularisation at 5-6 days
describe sensation return in each type of graft thickness
- more likely complete return in full thickness
- poorer return in split-thickness
- may take up to 2 years
describe how cultured autologous keratinocytes work
- biopsy of your own epidermal cells taken (usually from behind ear) and cultured in lab to form skin sheets in about 2-3 weeks or spray-on suspension in 5 days
what are advantages and disadvantages of cultured autologous keratinocytes
advantages
- allows large %TBSA burns covered without huge donor sites
- nil rejection (own skin)
disadvantages
- skin remains fragile - lack of dermal attachments
- inflammation could cause blistering and sloughing off
how does a homograft work
- tissue donation is from human donor that has been cryopreserved
- rejection occurs within 7-14 days
- used as a temporary cover over an autograft for protection
- gradually falls off and leaves patient's own autograph underneath hopefully healing well
advantages and disadvantages of homografts
advantage = protection of autograft
disadvantage = could transmit infections (but screened like blood donations), expensive, in short supply
identify two skin substitutes
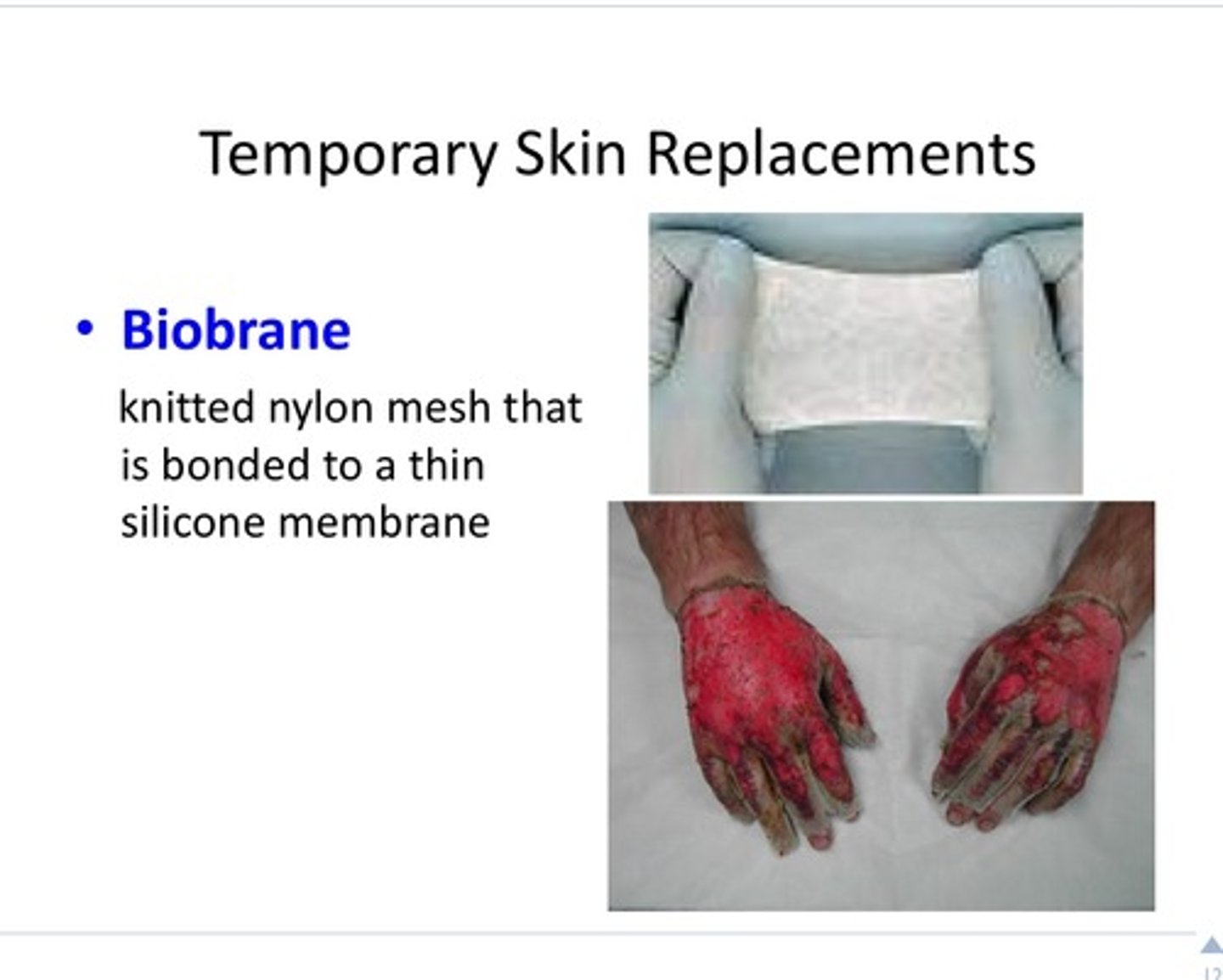
1. biobrane
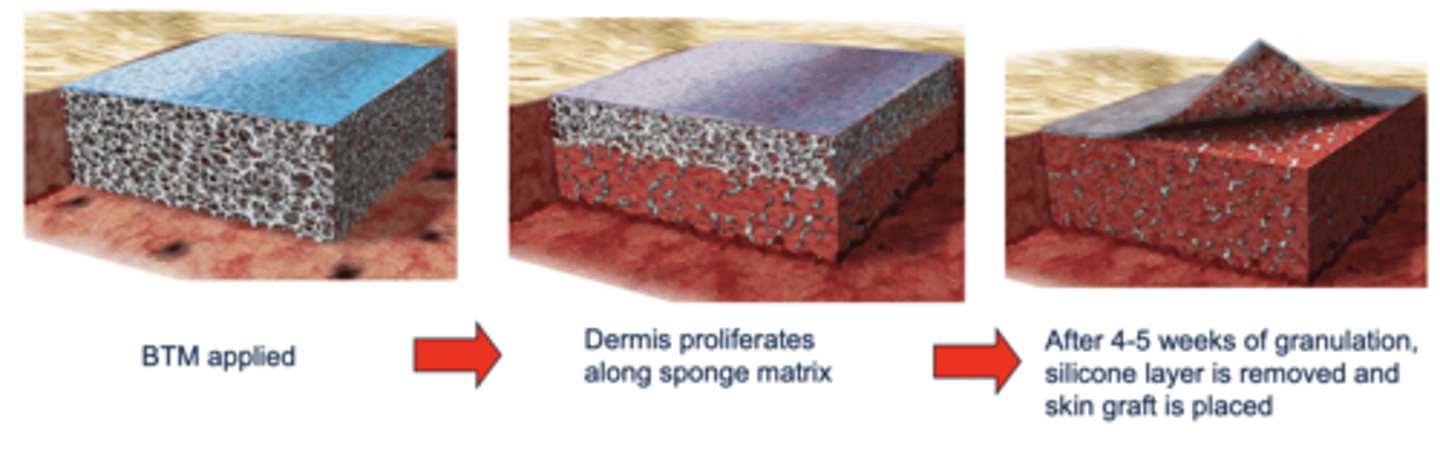
2. biodegradable temporising matrix (BTM)
describe biobrane and how it is used (6 points)
1. synthetic nylon mesh covered with silicone rubber membrane
2. semi-permeable to water
3. protective barrier to micro-organisms
4. temporary cover for partial thickness burns
5. staging procedure for full thickness burns
6. good for children - less dressing change, less pain
describe biodegradable temporising matrix (BTM) (3 points)
1. 2 layer system: dermal replacement (synthetic sponge) and epidermal replacement (silicone)
2. wound debrided to viable tissue and BTM layered on top for 4-5 weeks (allow granulation to occur)
3. dermis proliferates along sponge matrix
when are flaps performed for burn wounds
- when simple skin graft is not enough to cover wound
- when needed to cover exposed bone, tendon, etc
two types of flaps for burn covering
skin flaps - skin with or without underlying fascia
muscle flaps - created from muscle with or without overlying skin
main difference between flap and graft
flap is usually transferred WITH its own blood supply while skin grafts' blood supply comes from underlying wound bed
immobilisation period following a flap procedure
10 days
2 types of inhalation injury to upper respiratory tract
1. direct thermal injury
2. upper airway oedema
2 types of inhalation injury to lower respiratory tract
- interactions of chemical compounds in smoke
- high pressurised steam causing direct thermal damage to lungs
- rare to have direct thermal damage due to efficient cooling and fast glottic reflexes
5 consequences of inhalation injury
1. damage to mucosal lining
2. mucosal oedema
3. de-epithelialisation
4. pseudo-membrane formation (plugs airway and compromises alveoli)
5. deactivation of surfactant
2 common causes of burn inhalation injuries
1. burn injury occurred in enclosed space
2. lowered consciousness at time of fire
clinical signs and symptoms of an inhalation injury
1. respiratory distress -> increased RR, SOB, energy costs
2. bronchospasm
3. carbonaceous (sooty) sputum
4. auscultation yields wheezing and crackles
5. arterial blood gas = increased carboxyhemoglobin and decreased PO2
6. chest x-ray = pulmonary oedema and patchy atelectasis (partial collapsing due to impaired surfactant)
how to confirm an inhalation injury
bronchoscopy - see airway oedema, mucosal necrosis, pseudomembranous plugs, soot/char present
identify the 3 stages of inhalation injury and timeframe of each
1. acute pulmonary insufficiency (36 hours)
2. pulmonary oedema (6-72 hours, peaks at 12)
3. bronchopneumonia (3-10 days)
what does nebulised heparin do
breaks down pesudomembranous plugs
medical management of inhalation injuries (7 steps)
1. O2 delivered to flush out CO2
2. intubation and ventilation
3. bronchoscopy to assess damage
4. escharotomies to chest wall (help expansion)
5. bronchodilators and humidification to move secretion out
6. nebulised heparin - break down plugs
7. chest physiotherapy to cough out secretions
5 physiotherapy techniques for inhalation injury patients
1. manual/ventilator hyperinflation to increase air entry
2. remove sections by: percussion and vibration to chest wall, or suctioning
4. ventilation assistance: positioning, passive/active assisted ventilation, incentive spirometry, thoracic mobility, positive pressure devices
5. tilt-table activities
when can physiotherapists start percussion and vibration
right from the start - prior to grafting, can do directly over wound as patients are on good pain relief
when do physiotherapists stop and start manual techniques
- stop over newly grafted wounds (3-7 days)
- recommence depending on graft technique
long term complications of inhalation injuries
1. complications e.g. recurrent chest infections, pulmonary fibrosis, tracheal stenosis,
2. persistent impairment of lung function - decreased exercise capacity and fitness, respiratory muscle weakness, oxygen desaturation during exercise
identify the 3 steps to physiotherapy management of burns
1. respiratory management
2. oedema management
3. exercise prescription
4 ways to manage oedema after burns
1. elevate affected region above heart
2. breathing exercise to encourage lymph return
3. active exercises to activate muscle pump
4. compression bandaging from distal to proximal
5 aims of exercise prescription after burn injuries
1. decrease fear of movement
2. prevent/minimise contractures and maintain ROM
3. minimise effects of reconditioning from bed rest
4. minimise effects of hyper metabolism and muscle catabolism
5. minimise oedema
2 ways to minimise contractures after burns
1. exercises in opposite direction to possible contracture
2. elongation and stretching of underlying skin
- both allow collagen to arrange parallel to movement
3 precautions to movement/exercise after burns
1. other injuries e.g. fractures
2. escharotomy or fasciotomy
3. exposed tendons - don't tension/contract them
when do you mobilise burn patients
day 1 if possible with WBAT
precautions to FWB mobility
1. IV line in foot - secure properly
2. escharotomies down legs - need compression
3. exposed achilles tendon - isolated ankle ROM (step to gait)
4. burns to soles - need adequate protection/footwear
5. cellulitis - wait for IV antibiotics
how should burn patients be positioned while resting
- prolonged stretch but avoid stretching nerves
- anti-deformity positions e.g. shoulder in 90˚ ABd and 20˚ fwd F