Part 7a - 2026 - Collaterals, vascular sheathing, macroaneurysms, retinal emboli, sub-RPE subretinal hemorrhage, telangiectasia, ERM
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
What is the main reason for retinal vasculopathy?
Venous occlusion
What is retinal collateralization?
Blood vessels that develop within existing besselslk, usually near areas of nonperfusion. It can be capillary-to-capillary, vein-to-vein, artery-to-artery, artery-to-vein.
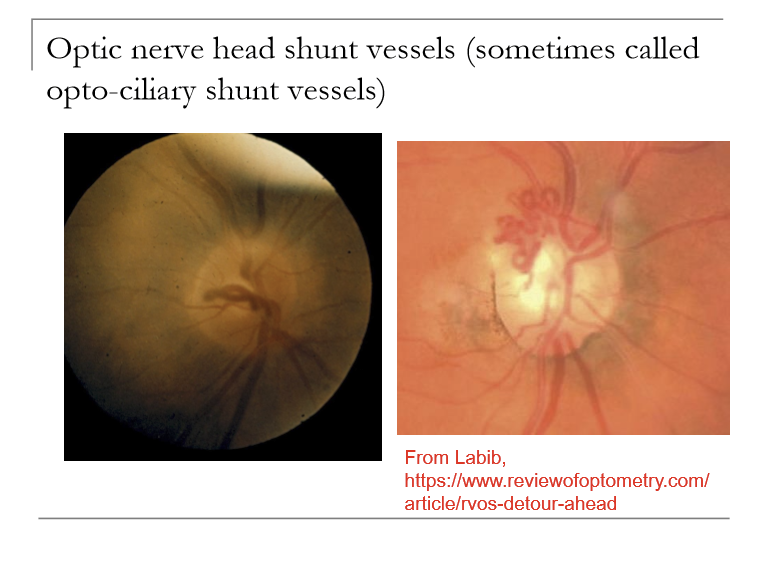
What are shunt vessels?
Retinal collateralization between vessels of different types
What can cause optic nerve head shunt vessels?
Congenital: does not mean much; pts are fine
Glaucoma: if IOP high enough, will crush optic nerve and central vein or artery.
Optic nerve tumor (progressive VF defect or central visual loss, optic atrophy, optic nerve head edema)
Post-CRVO
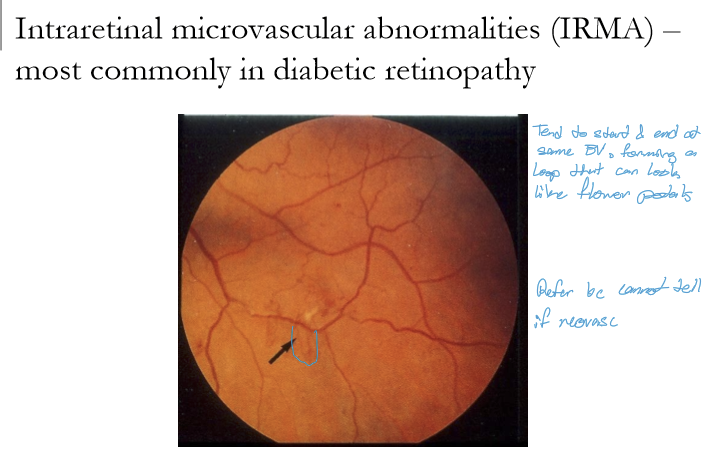
What are intraretinal microvascular abnormalities (IRMA), and in what condition are they most commonly seen?
IRMA are abnormal, dilated intraretinal vessels that form as shunts across areas of retinal capillary non‑perfusion.
They are most commonly seen in diabetic retinopathy.
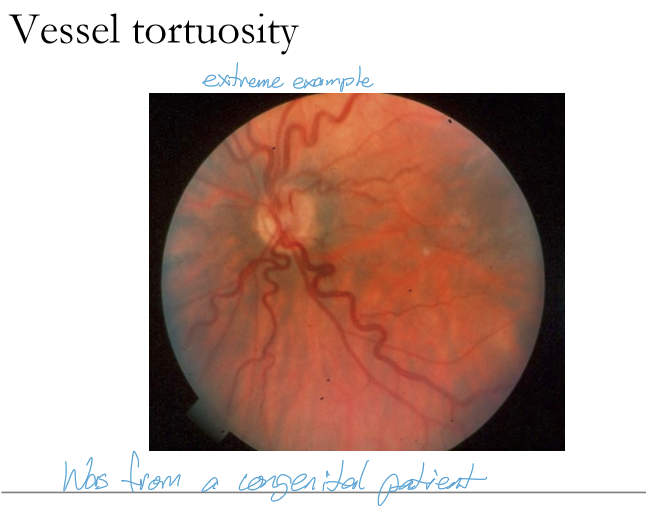
In which retinal vessels is tortuosity most commonly observed, and why?
Retinal vessel tortuosity occurs most commonly in the retinal veins because venous walls are thinner and more susceptible to dilation and distortion under increased venous pressure or hypoxic stress.
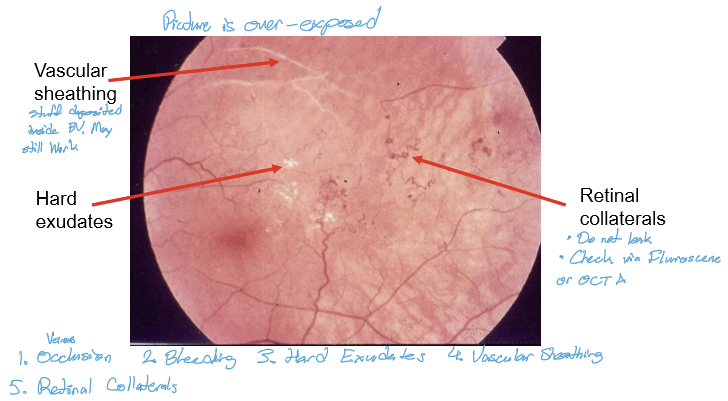
What is vascular sheathing? What is it made up of?
Deposition/thickening of retinal blood vessel walls
Materials include lipid, collagen, fibrin, hyaline, calcium
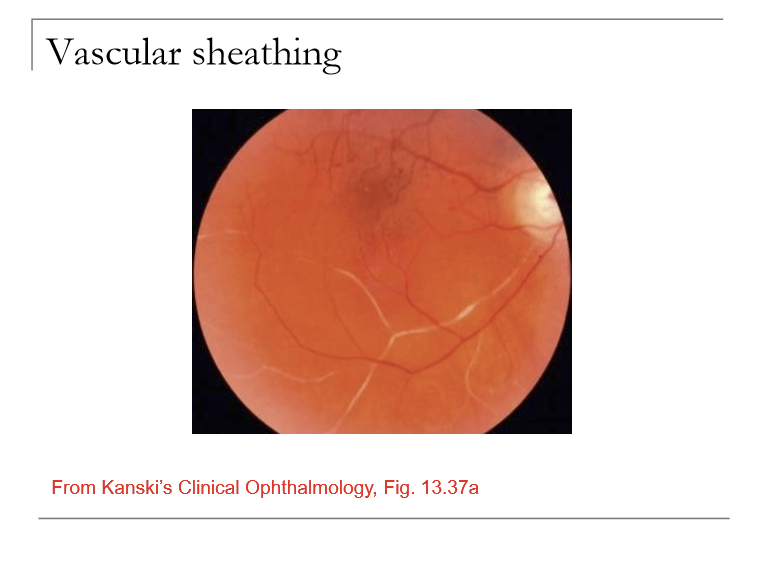
What causes vascular sheathing?
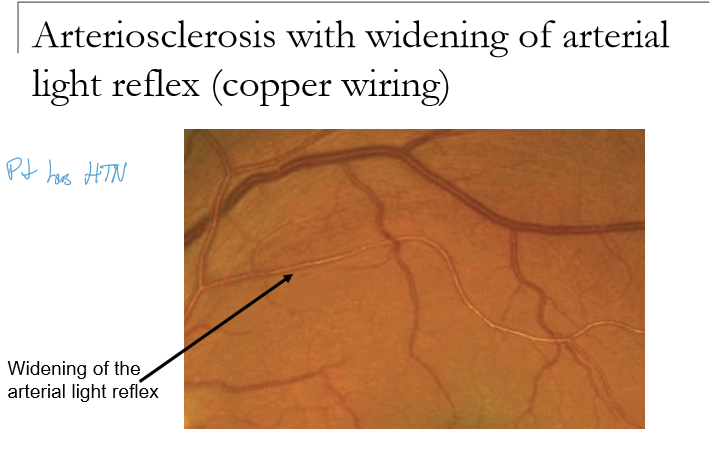
Arteriosclerosis (age-related or hypertension)
Vascular occlusion
Inflammation of the blood vessel walls (vasculitis or periphlebitis)
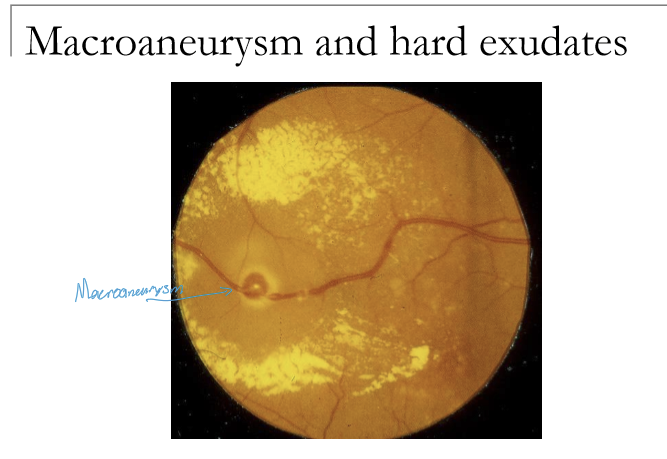
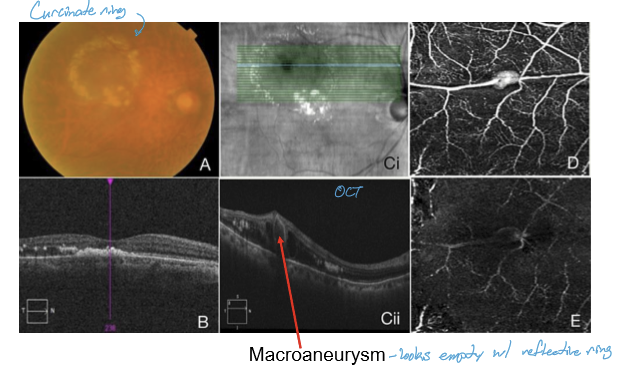
What is a retinal arterial macroaneurysm, and what is it associated with?
A dilation of a major retinal arterial branch. It is associated with arteriosclerosis, retinal emboli, can be congenital.
What are the typical patient demographics of retinal macroaneurysms?
Most common in ages 50–80.
~50% have systemic hypertension.
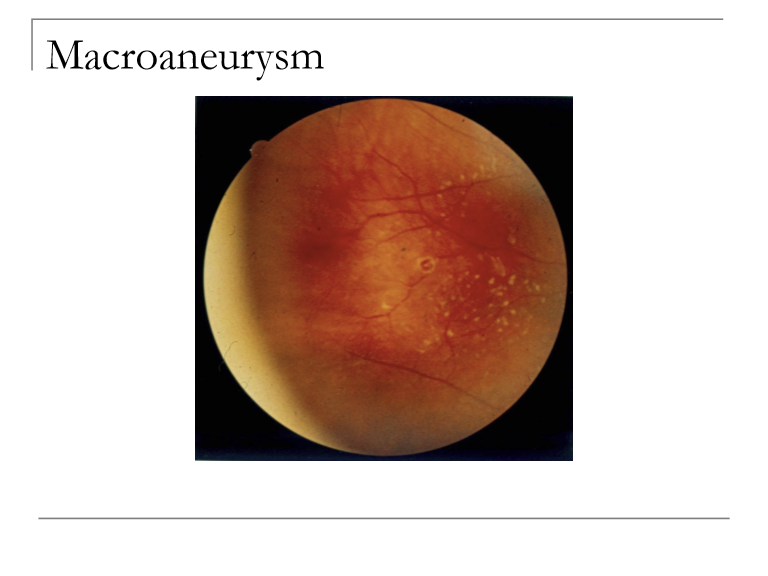
What ocular findings can be caused by retinal arterial macroaneurysms?
They can lead to edema, lipid exudation, or multilayered retinal hemorrhages (subretinal, intraretinal, or preretinal). Vision loss results from macular involvement or rupture.
HOw are macroaneurysms managed?
No exudation or heme= see every 6 months
Localized hemes, exudates= follow every 1-3 months
If threatening macula or risk of edema= refer
ALWAYS inform PCP regarding potential for HTN
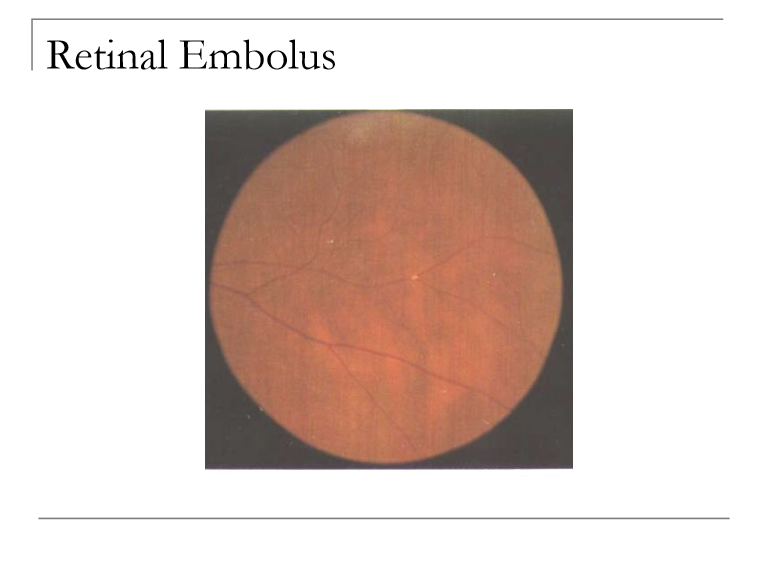
What are retinal emboli and what are the commonly from?
Material within blood vessels
Most commonly from carotid arteries, cardiac arteries, inected drugs
What does retinal emboli have a strong association with?
Cardiovascular disease
Do retinal emboli always cause vascular occlusion?
No. Retinal emboli may or may not cause an occlusion.
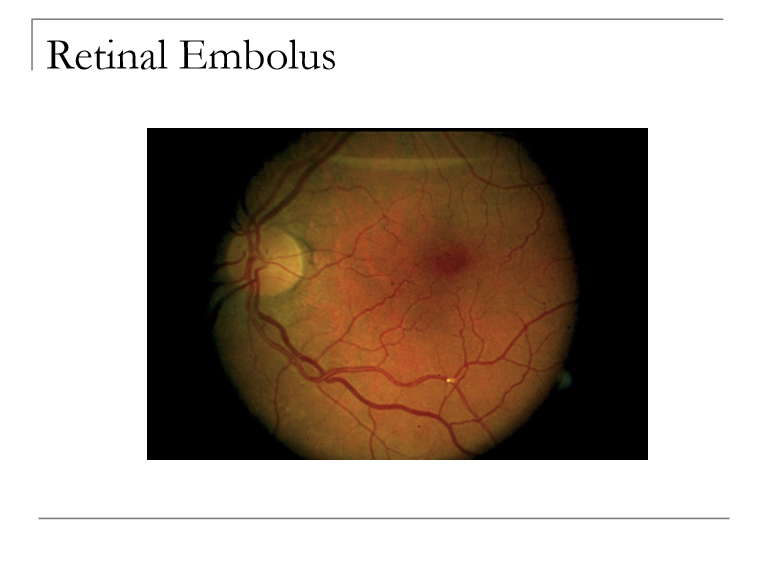
What can a retinal emboli consist of?
Cholesterol (holenhjorst plaque) : shiny yellow to orange
Calcium: gray-white (long-standing)
Platelets: dull white, long plugs
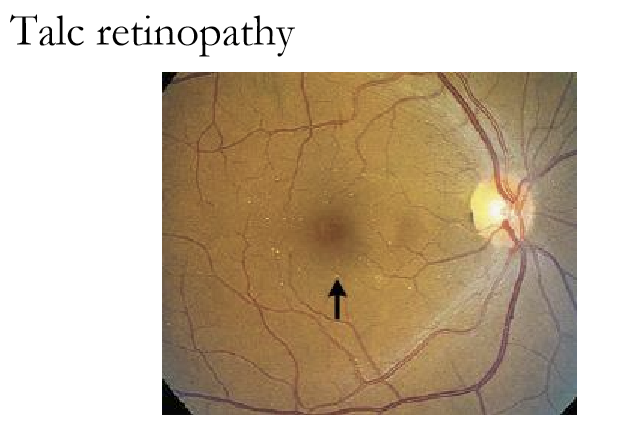
Talc (retinopathy): shiny, red-yellow, usually in intravenous drug users
What is the primary ocular concern when a retinal embolus is seen?
Concern is that the embolus has caused a retinal arterial occlusion, an ocular emergency due to the risk of permanent vision loss.
Patients with retinal emboli have a ~25% risk of stroke within 4 weeks.
What systemic conditions should be evaluated in patients with retinal emboli?
Assess for hypertension, hyperlipidemia, and possibly diabetes, all contributing to coronary artery disease, carotid artery disease, and other vascular events.
What is the recommended management if a retinal embolus is present without a retinal artery occlusion?
Urgent carotid and cardiac evaluation within 3-4 days.
Rationale: identify carotid stenosis, cardiac valve disease, or arrhythmias before a major vascular event occurs.
How should retinal emboli be managed if the patient has TIA or stroke‑like symptoms?
Treat as a medical emergency → immediate ER evaluation for stroke or acute carotid/cardiac pathology.
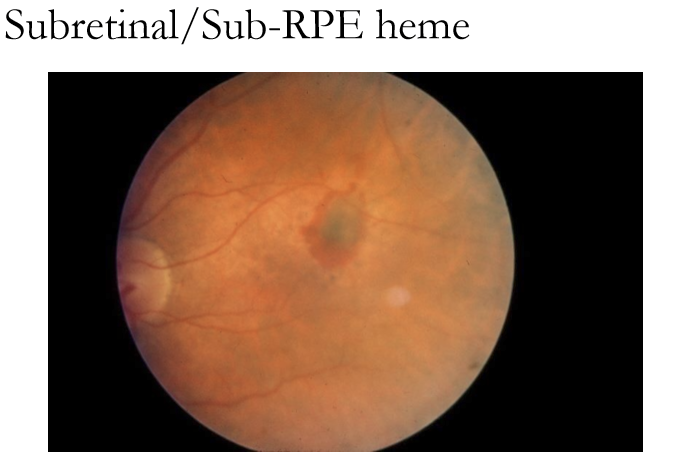
Where do sub‑RPE and subretinal hemorrhages occur anatomically, and what do they indicate?
They reflect deep retinal or RPE pathology:
Sub‑RPE: blood within the choroid/choriocapillaris beneath the RPE
Subretinal: blood between the RPE and sensory retina (retinal vessels may be seen overlying)
Both indicate involvement of deep vascular complexes, often from choroidal pathology.
What is the most common cause of sub‑RPE and subretinal hemorrhages?
Most commonly due to choroidal neovascularization (CNV). Less commonly arise from an extension of deep retinal hemorrhages.
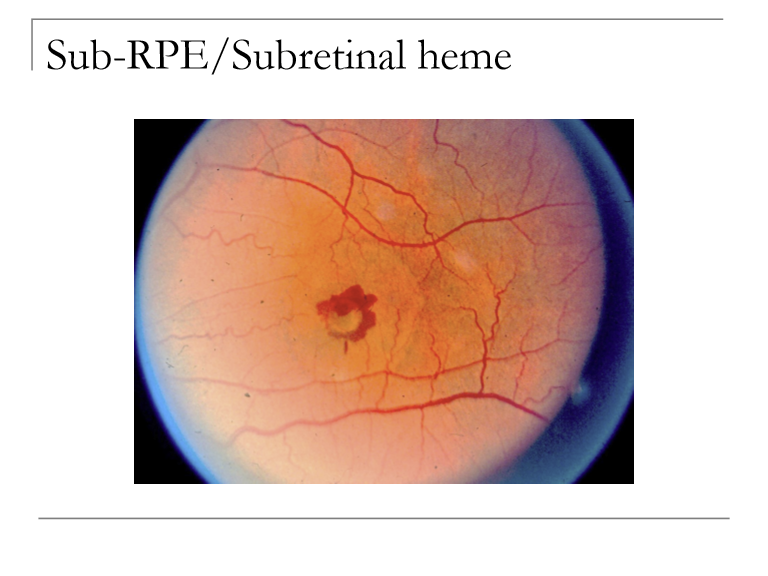
How can you clinically distinguish sub‑RPE from subretinal hemorrhages based on color?
Sub‑RPE heme: Gray‑green or dark appearance (blood under RPE pigment).
Subretinal heme: Dark red, sitting above the RPE where color is more visible.
What additional findings may accompany deep retinal hemorrhages over time?
May develop yellowish lipid exudation, which later becomes scar tissue and pigment mottling as blood and inflammatory products resolve.
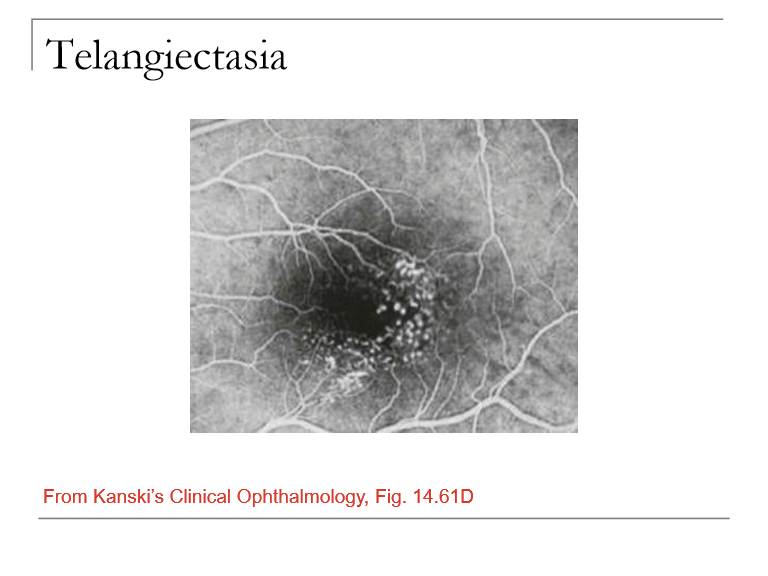
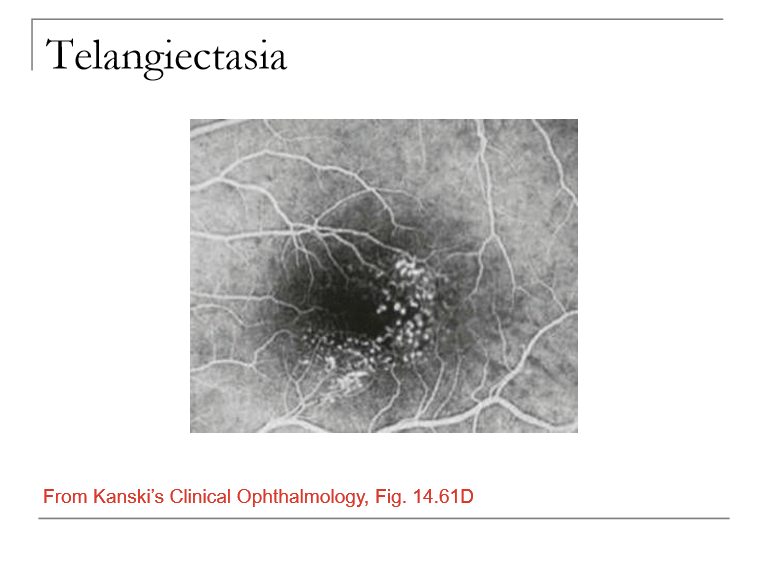
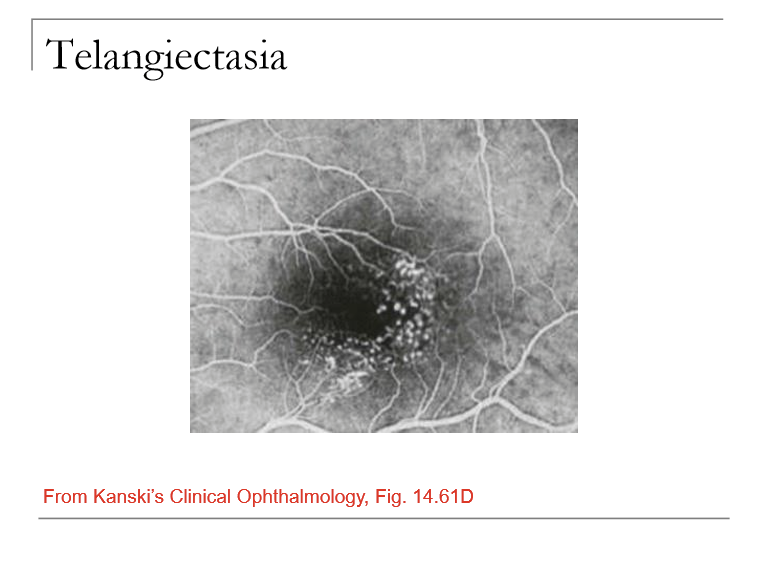
What is Idiopathic Juxtafoveal (Parafoveal) Retinal Telangiectasia and what vessels are affected?
A condition involving telangiectatic (dilated, incompetent) capillaries near the fovea/parafoveal region.
Characterized by aneurysms of small retinal capillaries affecting multiple retinal areas.
Is Mac Tel associated with systemic disease?
No. Idiopathic juxtafoveal telangiectasia is not necessarily linked to systemic disease and often occurs without hypertension, diabetes, or other vascular disorders.
What is the main visual threat in Mac Tel?
The telangiectatic vessels can leak into the macula, causing macular edema, reduced central vision, or distortion.
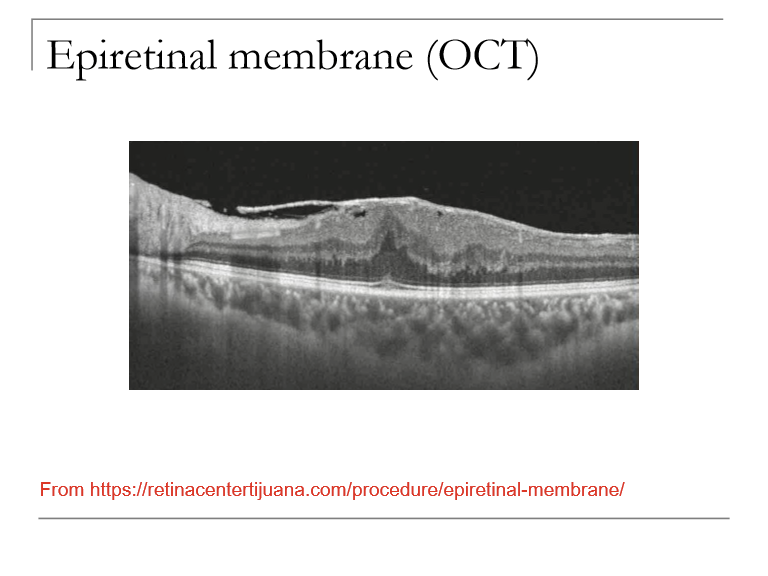
What is an epiretinal membrane (ERM), and what are its common alternative names?
ERM is a fibrocellular proliferation on the inner retinal surface, typically over the macula, causing retinal distortion or traction.
Also known as:
Preretinal membrane
Macular pucker
Surface‑wrinkling retinopathy
Cellophane retinopathy
Premacular fibroplasia
Preretinal gliosis
Preretinal macular fibrosis
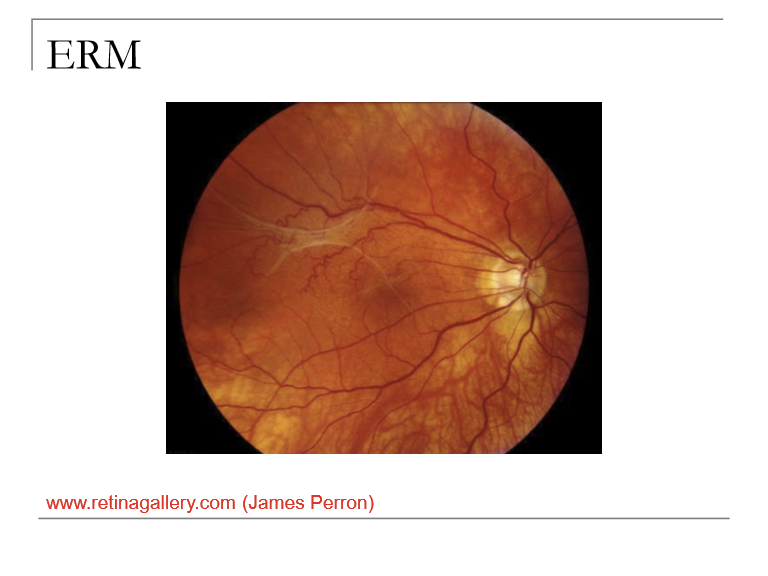
What is a potential underlying cause of epiretinal membrane formation?
ERM can arise from retinal vasculopathy (a nonspecific term for retinal vascular disease), which promotes migration/proliferation of glial cells on the retinal surface.