Ultrasound Guided Interventional Techniques (Ch. 18)
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
why use US for procedures?
high resolution, imaging frame rate, diagnostic accuracy
enhances transducer design (small footprint)
new technology: compound imaging and fusion technology (CT on US)
versatile needle guide attachments that offer multiple angle accessibility and accurate needle placement (shorter distance and least angle desired)
less costly and minimally invasive
continual real-time visualization of needle
various patient positions and procedural approaches can be used
physical presence of procedure team during entire procedure
portable
no use of radiation
shorter procedure time
informed consent
necessary for any procedure that is considered experimental, invasive, or involves substantial risk
patients’ agreement to allow something to happens after full disclosure of the facts needed to make the decision
by signing Informed Consent, the patient/patient’s representative indicates that:
patient has been informed about the procedure and its sequence
patient has been informed of all the risks and benefits of te procedure
potential complications
responsible alternatives to the procedure and their risks and benefits
patient consents to the procedure of treatment
for consent to be valid…
patient must be legal age and mentally competent
patient must offer consent voluntarily
patient must be adequately informed about the medical care being recommended
patient must not be persuaded
sterile set-up
usually established using a sterile drape that is free of germs
only sterile items are used in the sterile field
must be continually monitored
a sterile person can only touch what is sterile
unsterile persons cannot reach over or above a sterile field
confirm that it is sterile:
is the packaging expired?
is it dirty or wet?
has it been opened?
gowns are considered sterile on the sleeves and the front from the waist up
sterile gloves must be kept in sight and above waist level
persons in sterile gown/gloves must pass each other back to back
sterile materials must be kept dry
sterile field becomes wet it must be re-sterilized or discarded
things that are considered unsterile:
below the level of the table/waist, as well as the undersurface of the drape; any item that falls below this level is considered contaminated
the back of the gown and area below waist
1 inch border around the sterile field is not considered sterile
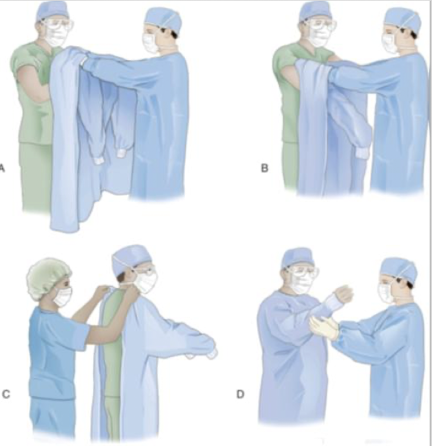
how to gown another person
sterile person picks up the gown by the neckband, holds it at arm’s length, and allows it to unfold
gown is held by the shoulder seams with the outside facing the sterile person
sterile gloves are protected by placing both hands under the back panel of the gown’s shoulder
arms are slipped into the sleeves in a downward motion, sliding the gown up to the mid-upper arms
nonsterile circulator pulls the gown up and fastens the back and waistband of the gown
gently pull the cuff back over the person’s hands, being careful that your gloved hands do not touch the bare hands
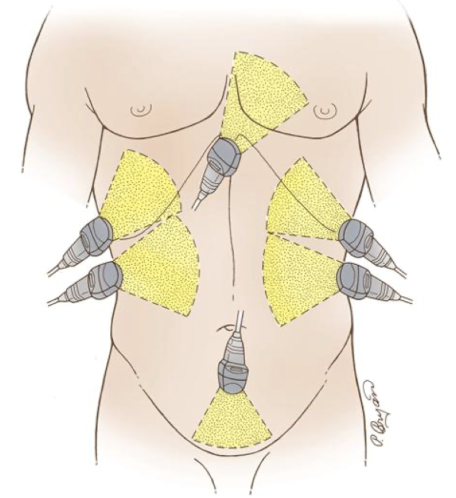
what procedures can be done with US guidance?
biopsies of various masses in the neck, chest, abdomen, retroperitoneum, pelvis, and MSK system
aspirations/drainage of abscess or fluid collections (percutaneous)
paracentesis and thoracentesis
peripheral, subclavian, or jugular line placement
IVs, joint injections
ablations
elastography
how to find the needle
visualization of needle is most important part of procedure
if needle is not visualized, transducer should be moved, not the needle
needle must be in the center of the transducer
TIP: the more perpendicular the sound beam is to the needle, the more sound will return → better reflection from the needle
providers have 2 techniques to introduce needles and devices into patients
free-hand
mechanically guided technique
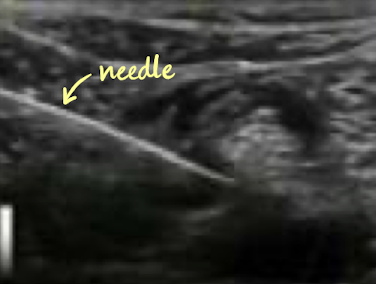
free-hand technique
MC used
advantage
good when accessing superficial structures
disadvantages
difficult to use during renal biopsy
potentially longer procedure time
challenging to access deep lesions

needle guides
mechanically guided and attaches to transducer
depicts a path on the US machine as a single line or two parallel lines
may offer choices of angles
keeps the needle aligned with the beam for continuous needle visualization

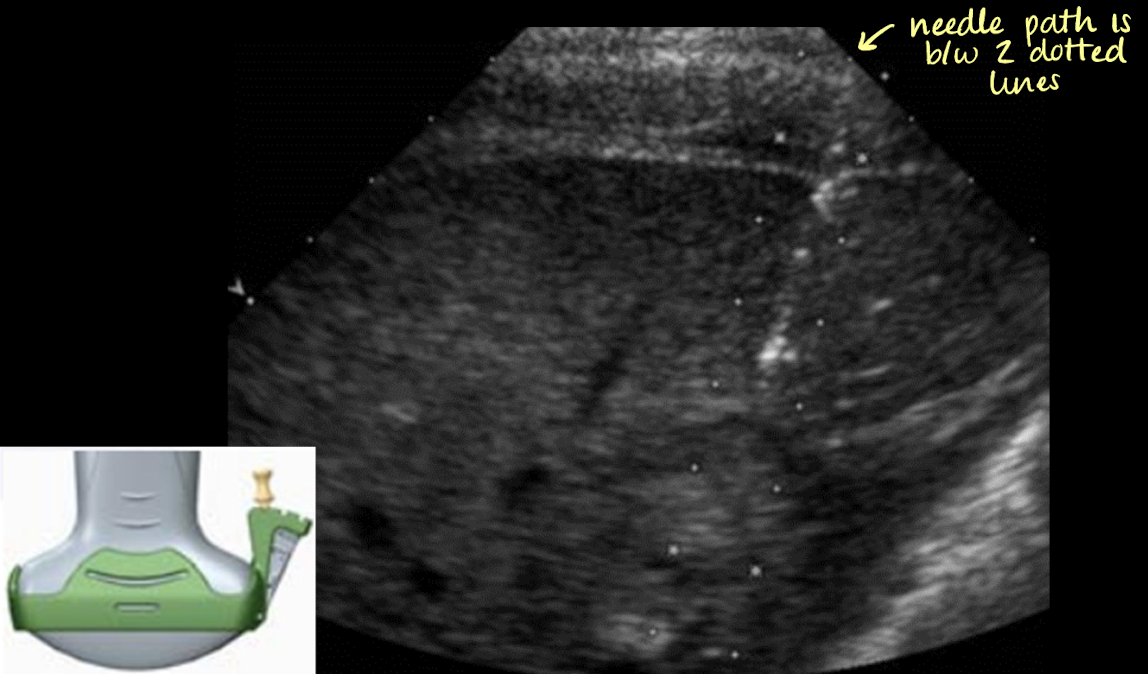
what technique is being used?
mechanically guided technique
ablations
radiofrequency, cryoablation, laser, microwave, and high intensity focused ultrasound (HIFU)
destroys cancerous cells tissue via cold or hot temperatures while maintaining the surrounding normal tissue
non-surgical patients
unresectable masses
during the procedure: as cells are destroyed, gas/microbubbles (nitrogen) is released
SONO:
hyperechoic echoes=confirmation of tx
elastography
liver and breast
eval. for fibrosis
evaluation of tissue stiffness
reduces the need for core biopsies
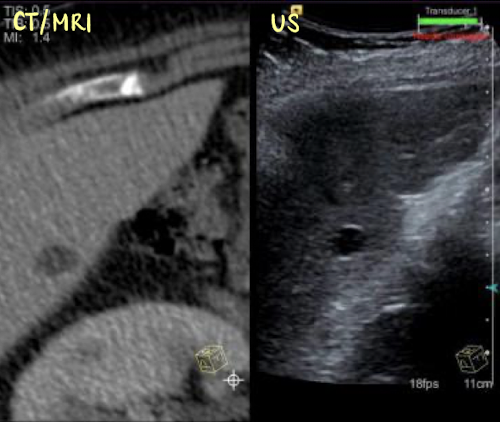
fusion imaging
involves important a CT or MRI scan directly onto the US machine
side by side images
superimposed/overlapping images
as the US machine moves, so does the other imported modality images
indications for a biopsy
confirm malignancy (MC)
need to differentiate metastatic vs second primary mass
determine the cause of mets in a patient with known primary malignancy
to differentiate recurrent tumor from therapy scarring
differentiate malignancy from inflammatory or infectious dz
determined lymphadenopathy from lymphoma
to characterize a benign mass
to obtain a sample of parenchyma in an organ to determine the progression of dz
abnormal lab values may warrant a biopsy
contraindications for a biopsy
lack of safe needle path
uncooperative patient
patients with a bleeding disorder/uncorrectable coagulopathy
ex. warfarin/Coumadin, heparin, aspirin therapy (increase risk of excessive bleeding during or after invasive procedure)
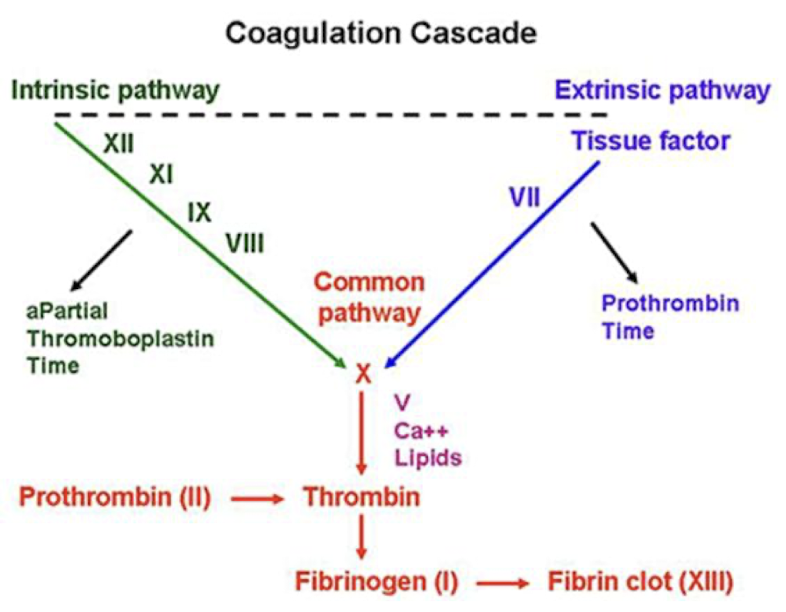
3 pathways in the blood clotting process
3 pathways: intrinsic, extrinsic, and common
two blood tests used to evaluate these pathways:
partial thromboplastin time (PTT)
measures how long it takes blood to clot and evaluates the intrinsic and common pathways
normal values are 25-35 seconds
prothrombin time (PT)
measures clotting in extrinsic pathway and helps determine bleeding or clotting risk during or after surgery
normal values are 11-13 seconds
because PT results can vary between laboratories, a standardized measurement called international normalized ratio (INR) was developed
0.8-1.1 (unitless)
if clotting values do not return to normal, patients may be given… (2)
fresh frozen plasma (FFP) or vitamin K to help improve blood clotting.
gauge (G) and length
the higher the number, the smaller the diameter
“20, 15,” or “20 × 15” = 20G needle and 15cm in length
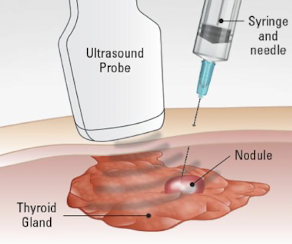
type of procedure: fine needle aspiration (FNA)
uses a 20-25G needle with cutting tip, such as Fransen, Chiba, or spinal needle
uses a thin needle to collect cells from a mass for cytology evaluation
if sample is too small, suction technique may be used:
a syringe and tubing are attached to the needle
this suction helps draw cells into the needle during sampling
reduces potential trauma to cells and decrease the amount of blood retrieves as well
FNA helps:
reduce trauma to cells
decrease the amount of blood retrieved
decrease background blood contamination
improve specimen quality for cytology
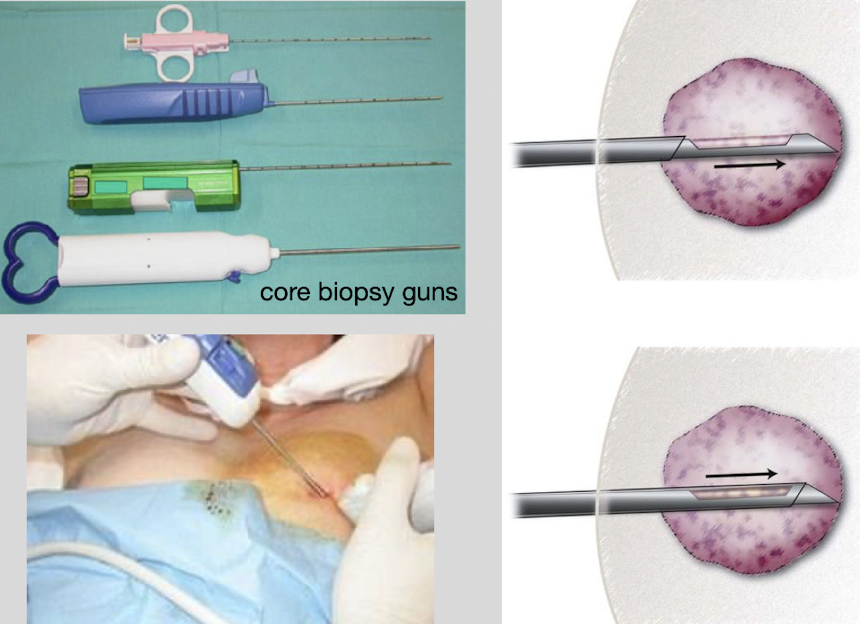
type of procedure: core biopsy
uses a 14-20G needle (larger than FNA)
uses a spring-loaded biopsy gun to obtain a core (small cylinder) of tissue for histologic analysis
when the biopsy gun is fired:
the cutting needle rapidly advances (“throws” forward),
cuts a tissue sample,
and stores the specimen in the “deposit slot” on the inner needle
“throw length” refers to the…
distance the needle advances when fired, and
length of the tissue specimen obtained
pay attention to how many “throws” (count them)
type of procedure: fluid or abscess collections
needle guide used, especially when…
the collection is small
difficult to access
multiloculated
near important structures
20-22G needle (for small fluid samples)
thicker fluid may require a lower G needle (small samples)
type of procedure: percutaneous drain placements
large abscesses or persistent fluid collections may require a percutaneous drainage catheter to remain in place for continuous drainage
pigtail catheter is MC type
the catheter is…
connected to a collection bulb or drainage canister
sutured to the skin (to keep it secure)
type of procedure: paracentesis and thoracentesis
paracentesis=drainage from peritoneal cavity (ascites)
ascites MC in RUQ and pelvis
thoracentesis=drainage from pleural space (pleural effusion)
lab orders
coagulation studies (PT/PTT/INR), platelet counts, and medication history (anticoagulants such as heparin or Coumadin) are reviewed to help reduce risk of bleeding complications during drainage procedures
20-22G needles used
thicker fluid may require a lower G needle (small samples)
large-volume paracentesis or thoracentesis require a centesis catheter (a 1-liter vacuum bottles connected to the catheter tubing)
prepared sterile tray is set up before procedure
transducer should be placed parallel to pt.’s skin (do not rock the probe)
cytopathology
some US departments work with cytopathologist during biopsy
on the spot evaluation/confirmation of diagnosable specimen
during the procedure:
usually 1-3 passes are performed
specimen is transferred onto sterile slides, then the slides are quickly stained in the US room
slide evaluation takes 3-5 minutes per pass or group of passes
benefits:
provide immediate confirmation that a specimen is diagnostic
increase the % of successful biopsies
helps minimize unnecessary passes
reduce overall procedure time

intraoperative ultrasound (IOUS)
real-time
used to facilitate surgery; aid in decision making; surgical planning
mobile US unit with specialized transducers that will fit through a surgical incision
uses a sterile cover
natural moisture used to couple transducer to organ of interest or warm saline us used
to sterilize the transducer:
soak in alcohol (30 minutes)
hydrogen peroxide gas (2 hours)
ethylene oxide gas (24 hours)
what is intraoperative US used for?
localization of lesions
determining lesion resectability
confirmation of blood flow
tumor thrombi and vascular invasion
relationship of lesions to vascular anatomy
surgical procedures of the brain, spinal cord, liver, GB, kidney, or pancreas
liver: the falciform ligament is resected and pulled down by the surgeon so the radiologist can scan the liver
kidney: sometimes removed from the renal fossa
role as sonographer: pre-procedure documentation
evaluate medical record for appropriate history, lab values, and other imaging studies
located and take images of the pathology of interest and best path approach
measure distance from skin to area of interest (to know length of cath. needed)
knowledge of how breathing affects movement of the mass
obtain informed consent
comfort/coach the patient and create the sterile field
set-up procedure workspace (trays, Dr. gloves, lab requisitions, proper lab tubes, patient labels, etc.)
have prior images on computer in procedure suite
radiology nurse monitors vital signs by ECG and pulse oximetry
role as sonographer: just before and during procedure documentation
“time out” (a pause before the procedure) to confirm the procedure, CORRECT patient, and patient understands what is going on (images can be taken as confirmation)
document by taking an image of the time the time-out took place
operate the US machine especially with free hand technique
focus on needle tip (SONO: echogenic dot)
document the number of samples (throws/passes) taken - FNA, progressive appearance of the location being drained, and any other images requests
be available for placement of prove cover, additional supplies that are needed, labeling of specimen, and gathering specimen
radiology nurse monitors vital signs by ECG and pulse oximetry
role as sonographer: post-procedure documentation
take after-procedure images (mass, fluid area, etc.) showing any change in shape or size of the location
evaluation of specimen (cloudy, bloody fluid, stinky, etc.)
accurate count of specimen (ex. 2 advances)
cleaning the US suite (sharps, trash)
sending specimens to labels with properly documented lab orders/requisitions
your initials, location specimen came from, date, and time
radiology nurse monitors vital signs by ECG and pulse oximetry
post-procedure care, discharge, and complications
ice packs may be provided
post procedural recovery time
vital signs obtained before discharging patient
minor complications:
post-procedural pain
hematoma
vasovagal reaction
severe complications (rare):
hemorrhage
pneumothorax
pancreatitis
infection
death
emergent procedures
assessing for blunt trauma via FAST (focused assessment with sonography for trauma) exam
perihepatic and hepatorenal space (RUQ)
perisplenic (LUQ)
pelvis: cul-de-sac (RLQ and LLQ)
pericardium
ectopic pregnancy
incarcerated or strangulated hernia
testicular torsion
intussusception
pyloric stenosis
appendicitis
avascular transplant
aortic dissection
pericardial tamponade (fluid fills pericardium → compression of rt ventricular wall)
ruptures AAA
pericardial effusion