PKPD Exam 4
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
Pristiq (desvenlafaxine)
80% Bioavailability
30% Plasma Binding
Primarily metabolised by conjugation (UGT), secondly by CYP3A4
Not affected by CYP2D6, unlike Venlafaxine
No Apparent food effect
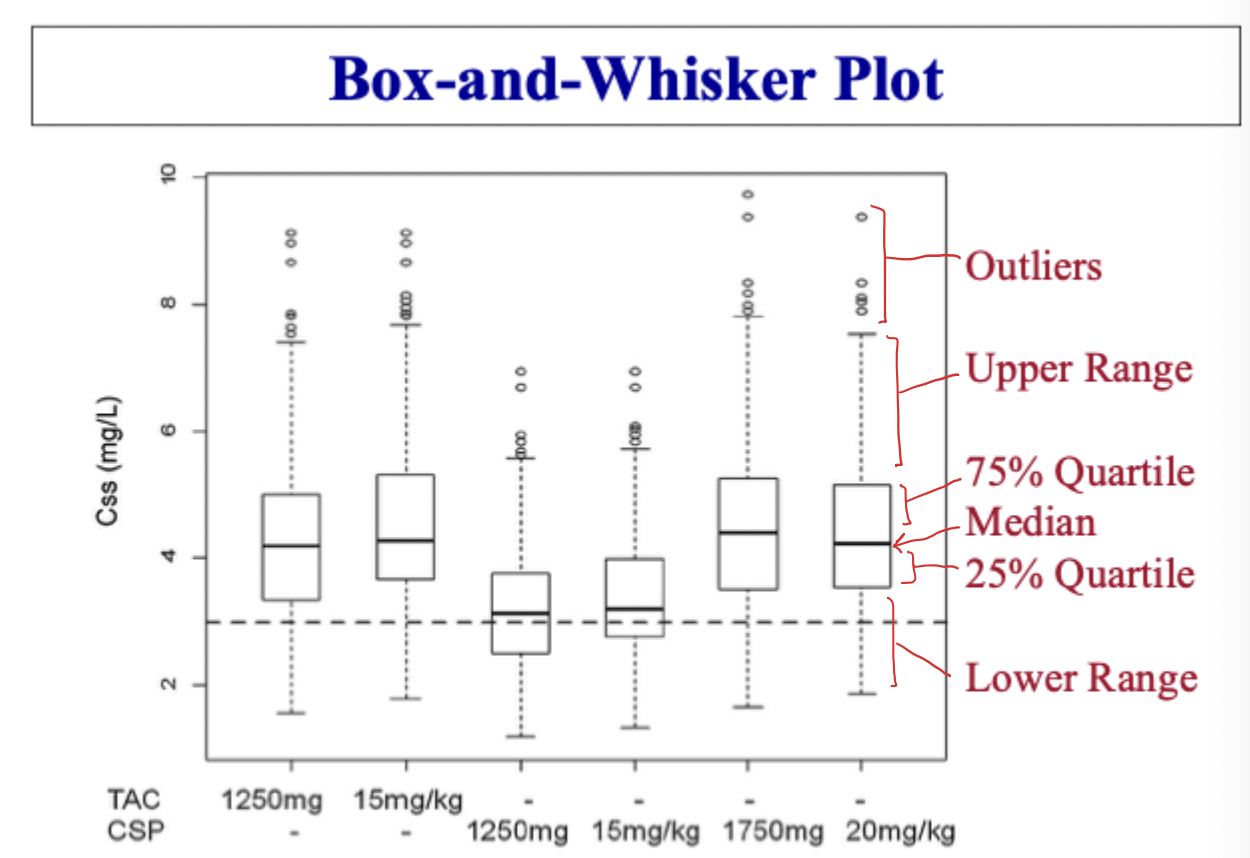
Box & Whisker Plot
Outliers
Upper & Lower Range
75% and 25% quartiles
Median
How can Bioavailability effect variatiability?
Greater variability in a group of subject when F is lower
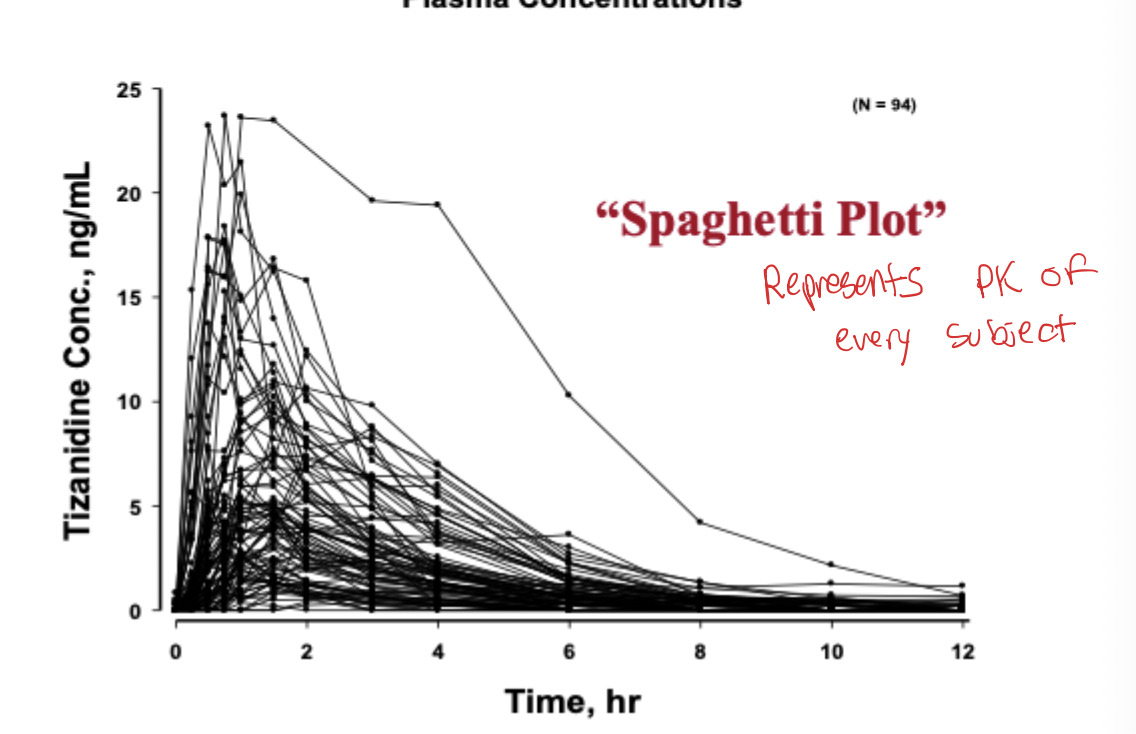
Spaghetti Plot
Shows the pharmacokinetics of every subject in a study
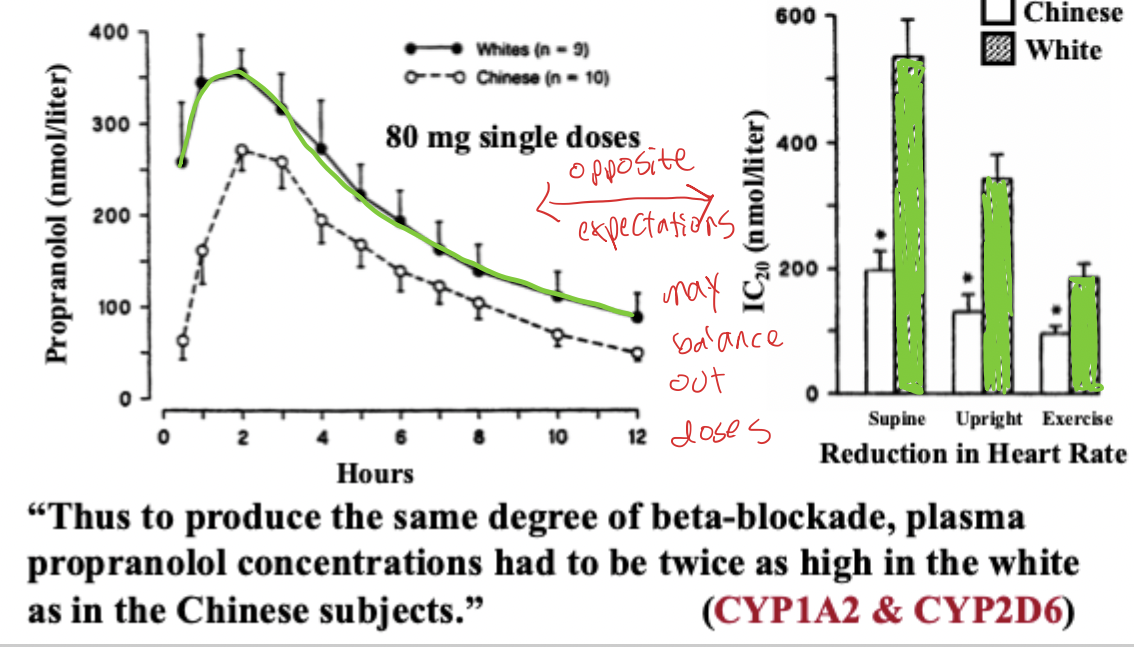
Racial Differences in Propranolol in Chinese vs American men
Chinese men had higher clearance and therefore lower AUC of Propranolol
However, Chinese men had a lower IC20, meaning they were more sensitive to propranolol and needed less to reduce heart rate
CYP2D6
Shows great genetic variability
Can cause an increase in exposure of drug, or decreased exposure of pro drug metabolite
Coefficient of Variation
CV = Standard Deviation / Mean
Physiological Function Trend with Increase in Age?
Decreasing about 1% per year
GFR, Renal flow, drug metabolism, etc..
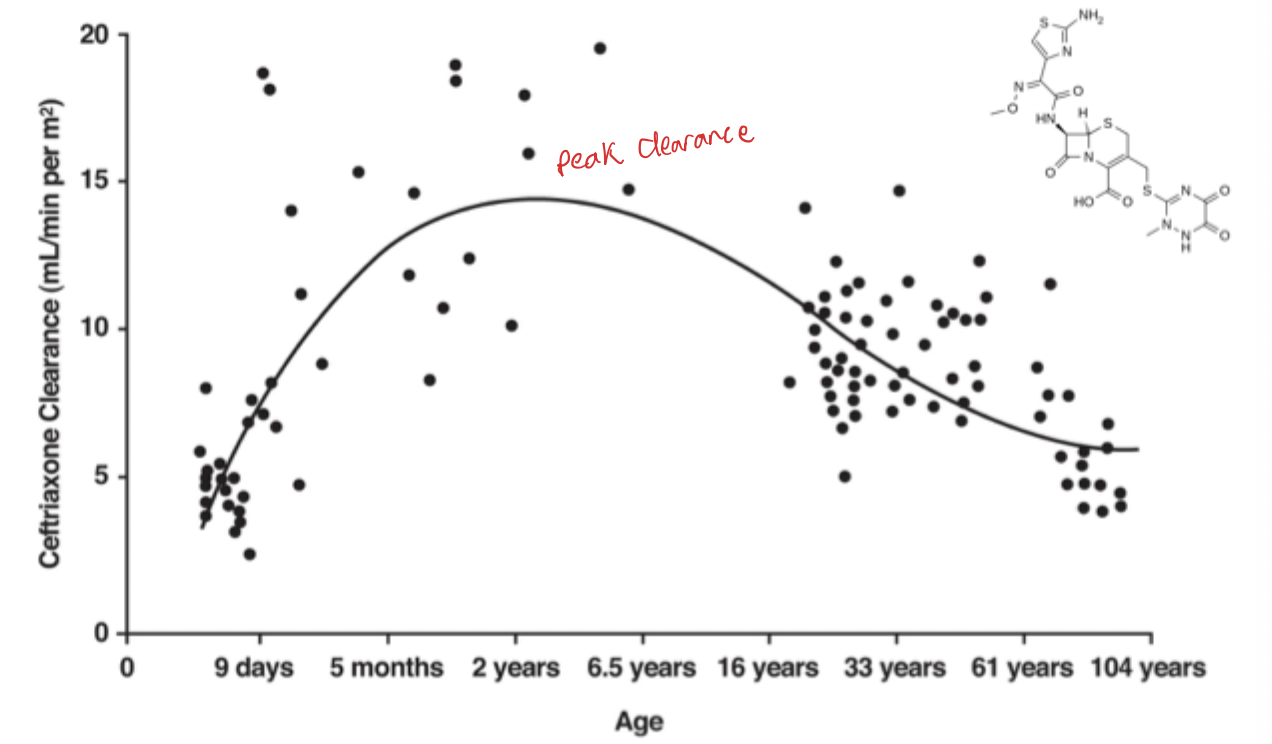
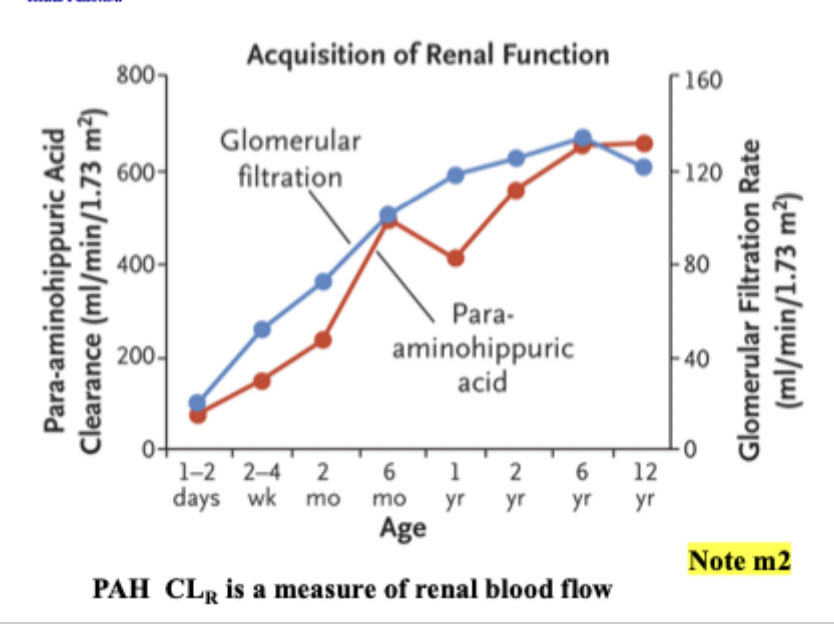
Renal Clearance with Age
Peaks around 2 years of age
V, Cl, EC50 Trend with Age
V tends to increase (more fat for lipophilic drugs)
Cl tends to decrease (and renal excretion)
Therefore, T1/2 tends to increase with age
EC50 can be higher or lower in the elderly, with no clear patterns
Lower EC50 seen in anesthetic and sedating drugs
Renal Blood Flow in Infants
Renal blood flow and clearance increases rapidly within first year of birth
However, infants still show lower clearance and greater sensitivity to other age groups
Allometric Scaling
Relates V and Cl to body weight
Cl = a * BW^(0.75)
a changes between drugs
0.75 ideal for drugs in human for Cl
a value of 1.0 is used for finding V
Enzymes that show higher activity in Females
CYP3A4 → ex. lovastatin, methylprednisolone (also had higher sensitivity)
Enzymes that show higher activity in Males
CYP2D6 → Metoprolol (almost 2x clearance)
CYP1A2 → Theophylline
Ketoconazole and Terfenadine
One of the strongest inhibitors of CYP3A4
Females had almost 2.5x more deaths from terfenadine compared to males
QTc prolongation, torsades des pointes
FDA requires all new drugs to undergo QT assessment with ECG’s
if QT change more than 10 = not passed
Caffeine during Pregnancy
CYP1A2 inhibited → higher AUC of caffeine in pregnant women
recommended not to drink caffeinated beverages
Effect of Pregnancy on PK
Somewhat unpredictable
Effect of Oral Contraceptives on PK
Can sometimes cause faster or slower metabolism of drugs
Ex. slower CYP1A2 metabolism of Tizanidine in women taking OC
Can increase metabolism of drugs that are metabolized by conjugation
Complexities in Obesity
higher BW = bigger liver = more clearance
higher BW = bigger Vd = high logP drugs can absorb into fat prolonging T1/2
Absolute clearance almost double but when normalized very similar to normal BW clearance
Levonorgestrel (Plan B) in Obese Women
Less effective in obese women → more rapid metabolism
Theophylline & Smoking
Smoking can increase clearance of theophylline through CYP1A2
Passive smoking also resulted in an increase in clearance
Thiocyanate & Smoking
Thiocyanate is a component metabolite of smoking
Smokers all had high levels of SCN-
Ex-smokers had major reduction in levels of SCN-
Non smokers had very low levels or none
Cotinine & Smoking
Primary metabolite of Nicotine
Smokers all had high levels of cotinine
Non smokers had very low levels of cotinine
Tizanidine & Smoking
Tizanidine is a CYP1A2 substrate
Smokers had a lower AUC of Tizanidine due to a higher clearance from CYP1A2 induction from smoking
Smoking and Drug Clearance correlation
Selective and unpredictable
Why does smoking cause enzyme induction?
Polycyclic Aromatic Hydrocarbons are most likely the cause
Carcinogenic
Nicotine is not the reason for induction
Nicotine Metabolite Ratio for CYP2A6 Activity
Nicotine is metabolized by CYP2A6 into Cotinine
Can use nicotine metabolize to determine patients CYP2A6 clearance activity
Those with low Cotinine plasma levels are usually slow metabolizers, and have higher quitting rates
Smoking & Oral Contraceptives
Smokers over 35+ are at a dramatically increased risk of CV diseases when using an OC
Congestive Heart Failure (CHF) and Renal Impairment
Clearance is reduced due too lower blood flow to liver
Vancomycin clearance is lower in both CHF and renal impairment due to being excreted mainly in the urine
Inflammation and Metabolism
TNF-a & IL-6 are both pro inflammatory cytokines
Increase in IL-6 (inflammation) results in decreased metabolism
Obese patients have higher than normal serum IL-6
Inflammation increases and falls during surgery
Thyroid Diseases on Metabolism
Hyperthyroidism
Increase in everything (clearance)
Hypothyroidism
Decrease in everything (clearance)
V not affected
Cystic Fibrosis
Increases Renal Clearance
Kidney size increases 1.5x normal
Increase in Hepatic Clearance
Erythromycin Breath Test
Erythromycin metabolism by CYP3A4 releases labeled CO2
CYP3A4 clearance can be determined from this
Women naturally have higher CYP3A4 clearance
During peal IL-6 (inflammation), erythromycin breath test shows decreased metabolism
Hepatic Disease
Liver cirrhosis, Liver Cholestasis, Liver Cancer
reduced blood flow, activity of hepatocytes, production of albumin
reduced bile flow → reduced clearance of biliary eliminated drugs
Child-Pugh Score
Class A → 10-15 points
Class B → 7 to 9 points
Class C → 5 to 6 points
Encephalopathy (mental function) → worse at higher points
Ascites → stomach fluid build up
Bilirubin → cleared by bile, so builds up in worser liver function
Albumin → produced by liver, lower levels in worser liver function
Prothrombin time → coagulation factors produced by liver, longer prothrombin time in worse liver function
Effect on Biliary & Renal Elimination
Liver disease → reduced formation & secretion of bile → decreased clearance
Cirrhotics have reduced renal plasma flow & GFR
Hepatic Clearance & Bioavailability
High ER drugs
blood flow (Q) limited
Inherently lower F which is sensitive to changes in fu & Clint
Low ER drugs
mainly influenced by changes in Fu & Clint
Inherently higher F which is less sensitive to changes in fu & Clint
Liver Cirrhosis effect on Absorption Rate
Patients are affected by gastritis & upper GI ulcers which can lead to delayed and unpredictable onset of action in cirrhotic patients
Delayed absorption has been shown for furosemide in cirrhotic patients due to impaired gastrointestinal motility
Liver Cirrhosis Effect on Protein Binding & Vd
Drugs that are highly bound to albumin or a1-acid glycoprotein have higher fraction unbound in patients with chronic liver disease
reduced synthesis of these proteins
Because of lower plasma binding, the Vd of certain drugs is larger in these patients
Drugs with high Vd are more sensitive to these changes in fraction unbound (fu)
Steady State Concentrations
Looking only at steady state concentration is not enough because an increase in fu and be “cancelled out” by a decrease in Clint
Oral → Cuss = dose / tau * Clint
IV → Cuss = fu * dose / tau * Q
REMEMBER THESE EQUATIONS NOT ON SHEET
5 Stages of Chronic Kidney Disease
Normal 125 mL/min
Stage 1 → 90 mL
Stage 2 → 60 - 89 mL
Stage 3 → 30 - 59 mL
Stage 4 → 15 - 29 mL
Stage 5 → 15 mL or less
Assessment of Renal Function
Renal function is estimated using creatinine clearance
Creatinine is a by product of muscle metabolism that is primarily eliminated by glomerular filtration
Women & elderly have lower muscle mass and lower CrCl
Cockcroft - Gault
Make sure to use right body weight
refer to equation sheet
Salazar & Corcoran Equation
Special Population → obesity
Use if actual body weight (ABW) is 30% greater than ideal body weight (IBW)
Schwartz Equation
Special population → children
Weight independent formula
Renal Impairment Effect on Protein Binding & Vd
Plasma binding of acidic drugs is decreased in renal dysfunction
Plasma binding of basic drugs unaffected
may be increased for some drugs because a1-acid glycoprotein is elevated in renal disease
Some drugs Vd may decrease due to fluid over load and an increase in fraction unbound in the tissue (decreased tissue binding)
ex. Digoxin → use Jusko equation to estimate
Non-Renal Metabolism Effects
Uremic toxins that accumulate in chronic renal failure can reduce drug metabolism activity (ex. CYP3A4, 2C9)
Glucuronide conjugates will accumulate, be hydrolyzed, and not cleared (reduced clearance)
Intact Nephron Hypothesis
Functions of all segments of a diseased nephron are affected equally
The loss of function is quantified by GFR
Renal clearance appears to vary in direct proportion to GFR/CrCl
T1/2 vs. CrCl & GFR Relationship
Fe = fraction of dose excreted unchanged in the urine
The higher the Fe, the more pronounced effect that renal failure has on drug PK
Dialysis
Removes wastes and excess water from blood in people with renal failure
Supplemental Dose equation
Optimization of Dosing Regimens
Dettli Rule 1 → elimination rate constant (kel) depends linearly on GFR
Drug dose is adjusted to renal function proportionally to Kel, dosing rate stays the same
Kunin Rule → Give normal first dose, then half dose every half life
Dettli Rule 2 → Normal dose given at prolonged interval
Drug Interaction Definitions
Perpetrator → drug, chemical, or food causing the interaction
Victim → drug affected by interaction
Enzymatic DDI
Inhibition
Decreased metabolism, increased AUC
Rapid onset due to direct effect on enzyme, no prior exposure needed
Induction
Increased metabolism, decreased AUC
Slow onset due to need of new enzyme synthesis, requires prior exposure
Types of Enzyme Inhibition
Competitive → reversible
graded effect, more perpetrator = more inhibition
Mechanism based → irreversible
Fm on Graded Effect
Fm = fraction of drug metabolized by the CYP inhibited
If Fm is closer to 1, then AUC is sensitive to changes in inhibitor concentration
If Fm is closer to 0, then AUC is not really effected by changes in inhibitor concentration due to a majority of the drug being metabolized by other pathways
Classifications of Inhibitors
Weak → 1.25 to 2 fold increase in AUC
Moderate → 2 to 5 fold increase in AUC
Strong → >5 fold increase in AUC
Time Course of Inhibition
Time course of maximum concentration = 5 times T1/2 of inhibitor plus 5 times T1/2 of drug
Effect of Inhibitors on Different Metabolizer Types
Poor Metabolizers → not sensitives, already at low activity not affected much by changes
Extensive Metabolizers → sensitive to changes in activity levels