Mobile and NICU
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
what does MICU stand for
medical intensive care unit
reasons as to why we would go see a NICU patient
indications for imaging- including but not limited to:
prematurity
line and/or tube placements
respiratory distress
congenital heart disease
lung lesions
abdominal pathologies
birth related injuries- fractures
what type of patients are MICU used for?
critically ill patients
what does SICU stand for?
surgical intensive care
what types of patients are in SICU
post surgery for long stay patients
what does IMU stand for
intermediate unit
what type of patients are in IMU
pt is closely monitored; step down unit from ICU
what type of patients are in PACU
after anesthesia
what type of patients are in NICU
neonates with life threatening issues or premature infants
what is the ED
emergency department (trauma bay or other ED imaging)
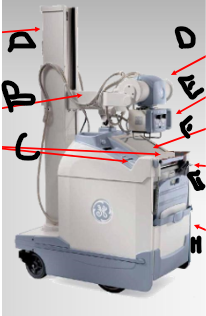
what is A
column
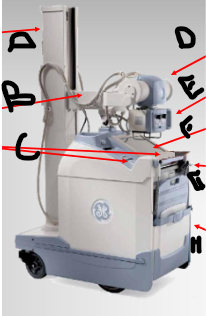
what is B
telescoping arm
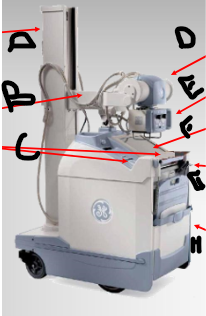
what is C
kVp/mAs settings
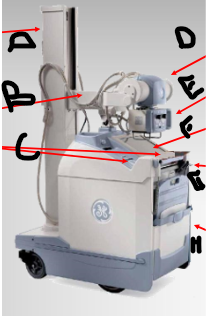
what is D
tube
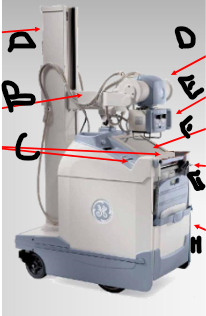
what is E
light box & collimators
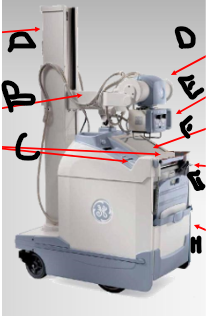
what is F
touchscreen computer
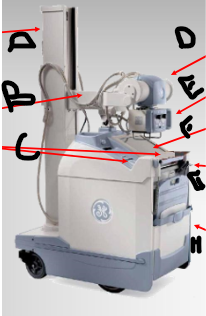
what is G
exposure switch
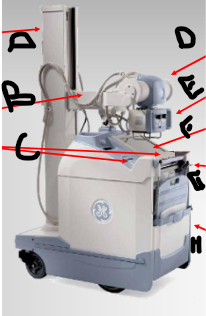
what is H
cassette or wireless image receptor
portable techniques
RH portables have flip book technique chart located in the bin with the detectors
variable kVp charts for portables!
use calipers!!
change kVp by 2 for every 1cm in body thickness
portable considerations
proper positioning
central ray alignment
shape distortion
grid
beam restriction
SID
artifacts
Beam restriction
1M- 39.4”
1.5M- 59”
2M- 78.7”
grid use for digital portable
RH: chest- greater than or equal to 30cm
extremities- greater than or equal to 10 cm (min 60 kVp)
abdomen (unless peds)- always use grid
information about portables
high frequency generators
technical factors utilized in radiographic room can be applied to mobile imaging
radiation safety
mobile radiography produces some of the highest occupational radiation exposures for radiographers
radiation safety- Time:
use proper techniques; limit repeat exposures
radiation safety- Distance:
occupational protection
patient protection
shielding
radiation safety- distance- occupational protection:
most effective means of protection (inverse square law)
stand min 6ft (2m); when possible right angle to pt/primary beam away from tube
radiation safety- distance- patient protection:
min SSD 12” (30cm) for mobile imaging (CFR21)
radiation safety- shielding- occupational protection:
-policy requires technologists and students to wear lead apron
lead apron/ thyroid shields min 0.5 mm Pb (NCRP 102)
-dosimeter outside of lead apron
-if contact isolation don lead apron before gown
radiation safety- shielding- patient protection:
-patient chielding: not required at RH
-others:
ask vistors and staff to temporarily leave the room
if they cannot leave then they need to be shielded
yell “x-ray” prior to breathing instruction
HIPPA
be mindful of others viewing request or computer screen on portable
don’t leave portable unattended
ask visitors to leave before asking hx and explaining procedures
portable maintenance
portable equipment should be cleaned at least every day
use gloves and Fresh Breeze TB
charge the portable when not in use
always log off when not in use
keep the portable stocked with IR covers
special considerations
isolation precautions
varying levels of consciousness
limited mobility or painful range of motion
spinal precautions on trauma patients
tubes, wires, lines and leads
what to do with isolation precautions:
follow precautions as indicated on the patient’s door
place the IR in a bag for isolation patients and anyone who is wet in bodily fluids
what to do with limited mobility or painful range of motion
ask MD/RN before ever removing any splints or immobilizers
if fracture present, use two people to hold/lift part and place IR carefully
use blankets, pillows or x-ray sponges to support the limb and/or IR (beware: artifacts)
what to do with spinal precautions on trauma patients
Never move collared patient without a nurse or physician present to hold the patient’s head
log roll
what to do with tubes, wires, lines and leads other devices
pull all lines away from the area of interest but do no disconnect i=or remove any
make notes in EPIC if there are IVs, name bracelets or other artifacts that you cannot remove or move away enough
MRI screening exceptions
stone protocol exceptions
during a code…
NEVER leave the detector under the patient during cardiac arrest
the charge of the defibrillator will cause malfunctions in the IR and possibly redirect the charge from the patient
chest tube placement is confirmed by:
portable chest x-ray performed to confirm placement
another name for chest tubes
thoracostomy (intrapleural) tubes
ET tube placement is confirmed by:
portable chest x-ray performed to confirm placement
PICC line placement is confirmed by:
portable chest x-ray performed to confirm placement
PICC line X-ray
-RH
patients are RPO 15 degrees, mark side down
must include should of insertion site and at least all of the mediastinum
SID 45”
angle of the RPO allows visualization of tip of PICC line away from spine
central line placement is confirmed by:
portable chest x-ray performed to confirm placement
NG tube placement (keofeed) is confirmed by:
portable chest x-ray or portable abdomen performed to confirm placement
for large bore NG tube:
most of the image should be chest with feeding tube visualized
top of IR at the level of the shoulders (Not higher)
if a portable abdomen is ordered include more of the abdomen with feeding tube visualized
CR at level 2” above crest
RH protocols line/tube placement
with any line or tube placement, if the line or tube needs to be advanced or pulled back, a new x-ray order is required to take another image to show the line or tube position
automatic verbal reports
automatic verbal reports are needed for…
PICC line placement
Feeding tube placement
NICU new central line placement
if the doctor request a verbal report on the order or at bedside
a neonate is a
newborn
premature is
born before the 37 week gestation
RH NICU mobile imaging
scrub hands for 30 second before entering
use hand sanitizer
use hand sanitizer between multiple patients
NICU precautions/preparation
equipment: #9 and #10 to obtain images (wipe them down)
digital detector: 9×11 housed in NICU
lead markers: disposable markers
make sure to shield nearby babies and NICU nurses
NICU IR placement
will be dependents on type of bed/isolette
IR placed in tray or directly under the patient
some beds have side measurements to air in centering the IR in the tray below
isolette
imaging is possible through the plastic
RN may lift the lid and tube would go under the lid (however- short SID)
open bed warmer
arm of heater may be moved for imaging
important to remember to place arm of heater back over baby immediately when finished exposure
Portable NICU chest positioning
IR portrait (9×11)
AP supine, nurse holds
CR at nipple line
tight collimation
40” SID
all surroundings shielded
yell “x-ray”
watch breathing for inspiration
portable NICU “babygram” positioning
IR (11×12 portrait)
AP supine0 nurse holds
CR at region of diaphragm
tight collimation
40” SID
ensure all surrounding are shieldedyell “x-ray”
watch breathing for inspiration
RH NICU PROTOCOL
NEVER REPEAT A NICU EXAM WITHOUT AUTHORIZATION FROM THE ORDERING PHYSICIAN
What is the no grid GCF
1
what is the 5:1 GCF
2
what is the 6:1 GCF
3
what is the 8:1 GCF
4
what is the 10:1 and 12:1 GCF
5
what is the 16:1 GCF
6
Grid rules
the tube must be perpendicular and centered to the grid in order to prevent
grid cutoff
elongation/distortion
the technique must be increased when using a grid
what type of tube is this?
chest tube
what type of tube is this?
ET tube
what type of tube is this?
PICC line
what type of tube is this?
central line

what type of tube is this?
NG tube
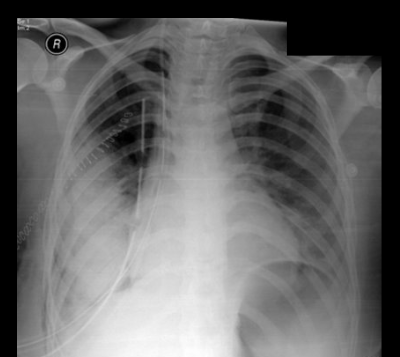
why is a chest tube placed?
to relieve air or fluid in pleural cavity space
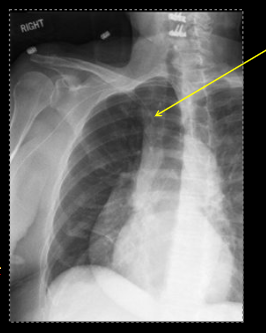
what is a pneumothorax?
air (seen higher)
what is pleural effusion?
fluid in the lungs (seen lower)
what is a hemothorax?
blood in the lungs (seen lower)
how much fluid has to be in the lungs to see it on an x-ray?
300mL
how much fluid needs to be in the lungs to see it on a lateral decub chest?
150mL
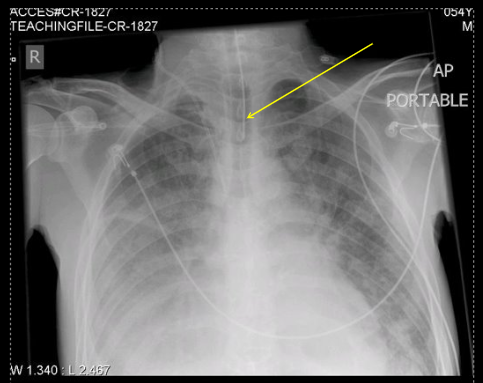
location on an ET tube
about 1-2 inch superior to the carina (not in esophagus)
most common mistake when placing an ET tube?
goes into the right bronchus because it is straighter and wider
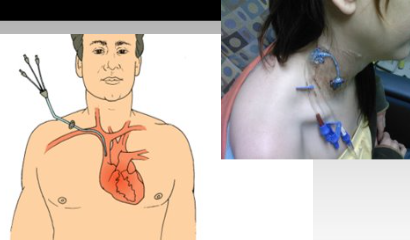
where is a PICC line placed?
peripheral line that goes in through right or left arm and goes into the heart
Distal tip ends at the SVC
can go into the cephalic, basilic or brachial
why do we oblique the pt for a PICC line x-ray?
to shift the mediastinum away to be able to visual the line
most common insertion site for a central line?
subclavian
central venous catheter
insertion of an NG tube
through the nose and end into the stomach junction