anemia
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
what is anemia
decrease in number of RBCs or too little hemoglobin
can also include a reduced Hgb binding capacity due to abnormal Hgb
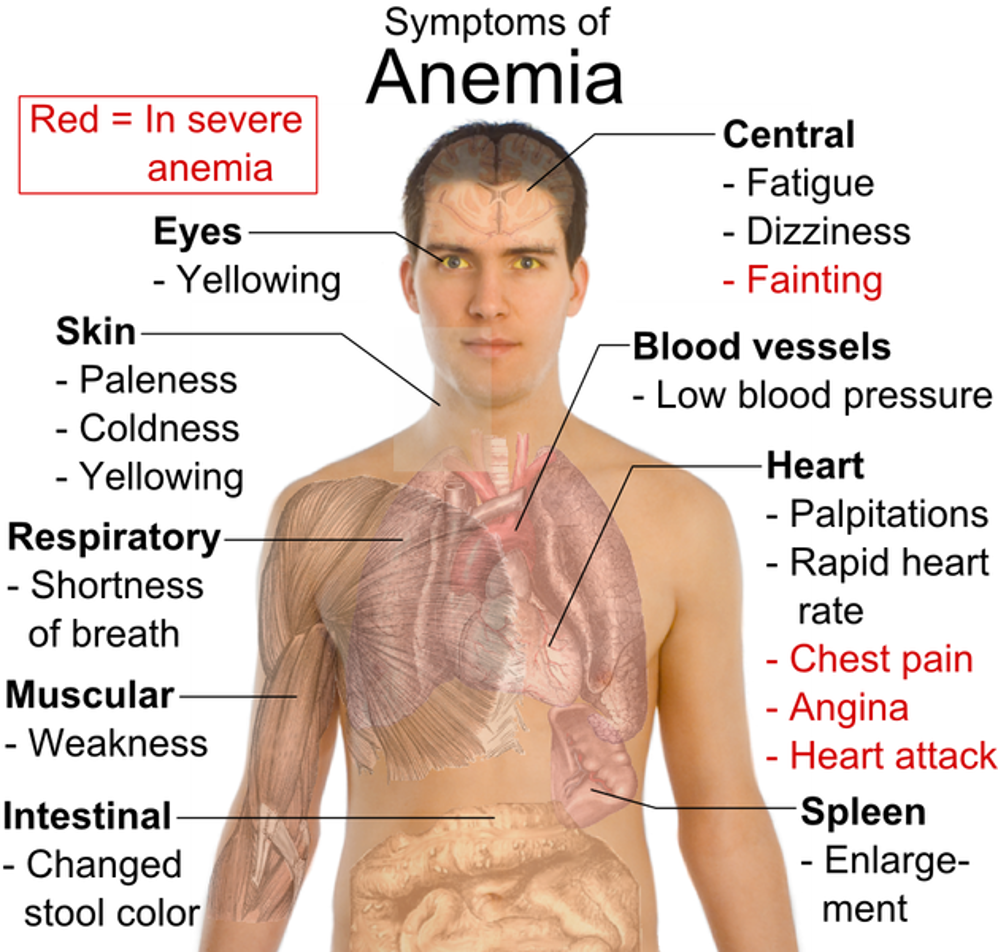
symtoms of anemia
hemoglobin
amount per volume of whole blood
hematocrit
volume of RBCs in unit of whole blood
red blood cell count
number of RBCs per unit of blood
mean corpuscular volume (MCV)
average volume of RBCs; microcytic, normocytic or macrocytic
mean corpuscular hemoglobin
amount of hemoglobin in cell; called hypochromic if low
mean corpuscular hemoglobin concentration (MCHC)
concentration of Hb per volume of cells
reticulocyte count
number of immature (new) cells
red blood cell distribution width (RDW)
greater variation shows greater variability in size of RBCs
iron deficiency anemia causes
90 % of IDA is caused by
Menstrual blood loss
GI blood loss
Pregnancy
Other causes
Poor iron absorption
Medications
Helicobacter pylori
GI diseases/surgery
Insufficient intake is uncommon in adults
♂ only 1-2 % of cases
iron tests
serum iron
total iron binding capacity
transferrin saturation
serum ferritin
serum iron
concentration of iron bound to transferrin
total iron binding capacity
Measures iron binding capacity of transferrin (will increase if iron is low)
transferrin saturation
Ratio of serum iron to TIBC; normal is 20 to 30% but will be lower with iron deficiency
serum ferritin
Measures iron stores; best indicator of iron deficiency
IDA labs
•CBC
microcytic
hypochromic
↓ MCV
•Fe Studies
Serum Iron- low
Serum Ferritin- low
TIBC- high
Transferrin Saturation- low
IDA factors affecting absorption
Best absorption via consumption of meat
Foods ↑ in Fe
blackstrap molasses
clams
raisin bran cereal
turkey (dark meat)
red meat
Absorption can be blocked by coffee, tea, egg yolk, milk, fiber, spinach
iron counseling (dose)
•Oral daily or 3 times weekly
•Best absorbed on empty stomach but may be better tolerated with food
•One form not more effective than another
•Patients may tolerate forms with less elemental iron better
•More iron will not correct anemia faster
•Iron is a pro-oxidant, so too much can be harmful
•Parenteral iron needed in some cases but risk of anaphylaxis
acid-reducing drugs and iron
•Acid-reducing drugs may decrease iron absorption
Acid-suppressing meds may still be needed for patient
Key is monitoring
iron and minerals/meds
Potential decreased absorption with minerals/meds
Ca, Mg, Al
tetracycline/doxycycline
take iron 1-2 hours before/4 hours after ideally
May need to separate differently for patient needs/practical regimen
mineral and med decreasing iron absorption
Ca, Mg, Al
tetracycline/doxycycline
response to iron Rx
•Hgb ↑≈ 1 gm/dL per week
•reassess if Hgb not ↑ by 2 g / dL after 3-4 weeks
•May need 6 to 12 months treatment for ferritin to return to normal
anemia of chronic disease underlying causes
infection cancer
autoimmune disorders
RA
SLE
inflammatory bowel disease
CKD
anemia of chronic disease
2nd most common form of anemia
normochromic normocytic
characteristically mild to moderate (Hgb- 9.5-8)
low retics
may be mixed with IDA
microcytes may be present
if mixed→anemia tends to be more severe
Key is treating underlying condition as much as possible
Fe status should be evaluated and Rxed if present
B12 deficiency causes
•80% of cases → Pernicious Anemia (lack intrinsic factor)
•10% of cases → achlorhydria
•B-12 is readily available in most diets and has a long storage time
•3-6 years to run out
B12 deficiency presentation
yellow pallor
neuro-findings
glove and stocking paresthesias, ↓ vibratory sensation
ataxia, spasticity, contractures
depression, psychosis, persecutory delusions
GI- sore beefy tongue and anorexia
tachycardia, palpitations, cardiomegaly, heart failure
B12 deficiency lab
•macrocytic anemia
•↑ MCV
•↓ serum B-12
•mild leukopenia and thrombocytopenia
•smear looks just like FA deficiency!!
treatment B12 (cyanobalamin)
•may be given orally, IN, or parenterally (IM/SQ)
•Parenteral –
most common
more reliable
may circumvent the need for a Schilling Test
•IN (Nascobalm)
may be used after initial parenteral treatment if no CNS involvement.
folate deficiency lab
•smear looks just like B-12 deficiency!!
•macrocytic
•↓ serum folate levels
•S/S similar to Fe def (and B12 if severe)
folate deficiency causes
•ETOH
•pregnancy
•malabsorption/ inadequate intake
•Drugs
Phenytoin
MTX
Colchicine
treatment folate
•Must also check B-12 level to avoid masking B12 deficiency!!
•1 mg/day po
•may need up to 5 mg/day in some cases of malabsorption
•Hgb will ↑ 2 wks after initiation of therapy and may normalize after 2-4 months
•may d/c if underlying deficiency is corrected
drug-induced hemolytic anemia
generally will happen quickly
drug-induced hemolytic anemia common symptoms
•Common symptoms:
Dyspnea/Fatigue
dark urine
pale or jaundiced
enlarged spleen
tachycardia/murmurs
•A number of meds have been implicated
drug induced hemolytic anemia treatment
•Removal of offending agent
•Transfusion considered if severe
•Possible use of glucocorticoids or IVIG
drug that can cause folate deficiency
phenytoin
methotrexate
colchicine