E Med exam 3 - Stroke TIA ICH
1/146
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
147 Terms
abrupt onset of a neurologic deficit that is attributable to a focal vascualr cause
stroke
reduction in blood flow that lasts longer than several secs. neuro sx manifest within secs
stroke
if cessation of flow lasts for more than a few mins, what occurs
infarction or death to brain tissue
when blood flow is quickly restored what can occur to the brain
brain tissue can recover fully and pts sx are only transient AKA TIA
all neuro signs and sx resolve within 24 hrs without evidence of brain infarction on imaging
TIA
if neuro signs and sx last for >24 hrs or brain infarction is seen on imaging what is this dz
stroke
when blood flow is interrupted to part of the brain this occurs
stroke
what happens when there is no blood supplying a part of the brain
oxygen and nutrients cannot be supplied and waste products can’t be removed. brain cells begin to quickly die.
depending on the region of the brain affected a stroke can cause
paralysis, speech impairment, loss of memory and reasoning ability, coma, or death
strokes occur more in what gender
males until age 55, then the risk is the same
what ethnicity is most at risk for strokes
AA, hispanic, and API pop
does fhx matter
yeah if your immediate fam had a stroke or TIA your risk goes up
pts with this other condition are at a greater risk of a stroke
DM
how to prevent strokes
lower BP, cholesterol, stop smoking
Leading cause of a stroke is
HTN
pathogenesis of HTN causing strokes
blood vessels damaged by high intraluminal pressure causing a narrowing, rupture, or leak. also causes blood clots to form in arteries
how can DM cause a stroke
free sugars get into blood vessel walls causing damage and accelerating atherosclerotic plaques
what is a hypertensive urgency
severe elevation in BP (>180/>120), NO evidence of acute target organ damage. pts are usually asx, or have HA, dizziness, mild SOB, nausea
mcc of hypertensive urgency
missing blood pressure meds. also can be from pain, anxiety, drug use (cocaine/amphetamines), meds like NSAIDs, steroids, decongestants, underlying kidney dz or undx HTN
how to tx a hypertensive urgency
adjust or restart PO meds (captopril, labetalol, amlodipine) to slowly lower BP over hours-days. rapid lowering is bad bc can cause ischemia
prognosis of HTN urgency
good, no immediate threat to organ fxn, though indicates a need for better long term BP management
what is a hypertensive emergency
severe BP elevation (>180/>120) WITH acute target organ damage.
what are target organ damage example sin a hypertensive emergency
encephalopathy, ICH/stroke, ACS, acute HF/pulm edema, AKI, aortic dissection, hypertensive retinopathy, seizures
how to tx hypertensive emergency
ICU admit and continue BP monitoring. use IV antihypertensives.
goal of hypertensive emergency treatment
dec MAP by 10-20% in the first hr. then dec another 5-15% over the next 23 hrs
what is the significance of MAP
provides a more accurate reflection of blood Q to tissues and organs.
nl range of MAP
70-100, 110 mmHg
abnl MAP levels
<60-65 suggests bad perfusion (HoTN), risking organ damage. if MAP >110 then = excessive P, risking CV damage
uses for MAP
used in intensive care to monitor pts with sepsis, stroke, or severe trauma
how to calculate MAP
(SBP+2(DBP))/ 3
IV first line drug tx for hypertensive emergency
nicardipine, labetalol, nitroprusside, nitroglycerin, esmolol
when is nicardipine indicated to tx HTN emergency
first line in many cases like stroke and general use
when is labetalol used to tx HTN emergency
good for most situations, including pregnancy
when is nitroprusside used in HTN emergency
rapid and potent. use w caution bc can cause cyanide tox
when is nitroglycerin used in HTN emergency
pref in ACS or pulm edema
when is esmolol used in HTN emergency
short acting, ideal for aortic dissection
tx route for HTN emergency
IV
first line meds for HTN urgency
lisinopril, amlodipine, labetalol, clonidine
how does hyperlipidemia contribute to a stroke
progression of atherosclerosis is directly related to cholesterol and LDL levels, and inversely to HDL. hi lipoprotein A is directly assoc with inc stroke risk and is used as a screening tool
how does cig smoking contribute to stroke risk
inc risk 2x. leads to hypercoagulable state and vascular damage
mini stroke/warning stroke
TIA
transient disruption of blood Q that results in focal neuro sx. stenosis or small emboli blocks vessels and tissue deprived of blood and oxygen and become symptomatic. body auto regulates and vasodilates or breaks up clots with endogenous tpa and blood Q returns and sx resolve
TIA
half of all strokes occur within how much time after a TIA
first 2 days after
how to eval stroke risk in 7 days after TIA
ABCD2 score
how to prevent stroke after TIA
aspirin and clopidogrel
what is the ABCD2 score
Age >60 (1)
BP > 140/90 (1)
Clinical features - u/l weakness (2), speech disturbance w/o weakness (1)
Duration of sx - > 10 min but < 59 min (1), >60 min (2)
Diabetes (1)
score <5 = 4%, 5 = 16%, 6 or more = 35%
why do we hospitalize TIA pts
facilitate early therapy and secondary prevention
what lab testing do we do on TIA pts
see full blood count, serum electrolytes and Cr, fasting blood glucose and lipids.
when is an EKG ordered for a stroke pt
within 48 hrs
what brain imaging study is indicated for TIA pts
CT or MRI in 48 hrs
what vascular imaging is used for TIA pts
carotid imaging, CT or MR angiography, or transcranial doppler w/i 48 hrs
how are strokes divided into
ischemic or hemorrhagic
what are the types of ischemic strokes
thrombotic or embolic
what is a thrombotic stroke
atherosclerotic clot forms within cerebral circulation.
what is an embolic stroke
clot forms elsewhere and travels to brain’s circulation
which type of strokes are more common
ischemic
what type of stroke poses higher mortality
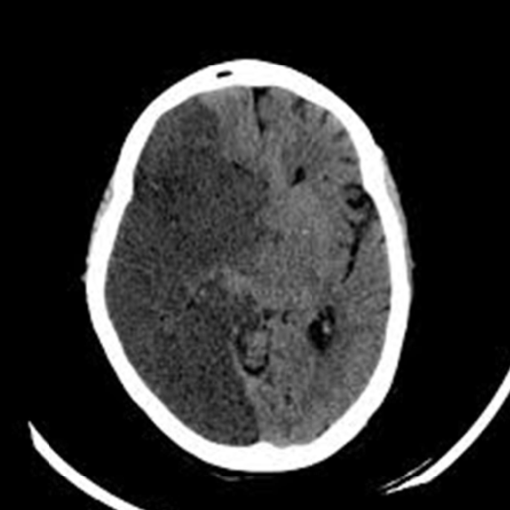
hemorrhagic
the result of the deficit in a stroke depends on
size of occlusion and the amount of collateral circulation the pt has to compensate for loss of blood Q
how does a cerebral ischemia lead to cell death and worsen the deficit
releases excitatory and other neuropeptides that may augment the flow of calcium ions in neuronal channels
mcc of cerebral embolism is
a fib
how does a fib cause cerebral embolism
atria of the heart beat weakly and fast, blood w/i the atria is not completely emptied. the stagnant blood forms clots in the atria which break off and enter circulation
how to reduce risk of stroke from a fib
daily use of anticoagulant meds like coumadin, pradaxa, xarelto, eliquis
cardiac sources of emboli in cardioembolic stroke
m/c, typically from left sided chambers/valves that form in myopathy or arrhythmia
artery to artery sources of emboli in cardioembolic stroke
from ruptured plaque in internal carotid arteries
paradoxical embolism source of emboli in cardioembolic stroke
vein to artery, usually occurs when venous thrombus from periphery enters the right side of the heart and is shunted via ASD/PFO or VSD to left circulation
other causes of cardioembolic stroke
a flutter, dilated cardiomyopathy or CHF with EF <30%, dec output = stasis and clot formation, MI, ETOH, genetic, infectious endocarditis, mitral valve stenosis or disease, atrial myxoma
persistent connection b/w the right and left atrium. embolus bypasses lungs via hole and enters left side of heart into circulation.
PFO
how to screen for PFO
echo (TEE is best)
high freq of PFO is found in what pop
YA with cryptogenic ischemic stroke
mcc fo stroke in young pop
cryptogenic ischemic stroke from PFO
how to tx PFO
ASA/ plavix, NOT closure unless the hole is very large or pt has recurrent embolic events
locations for ischemic strokes
lacunar infarct, anterior cerebral artery infarct (ACA), middle cerebral artery infarct (MCA), posterior cerebral artery infarct (PCA), vertebro-basilar arteries infarct
this infarct is a small lesion less than 5mm in diameter. found in short penetrating arterioles of basal ganglia, pons, cerebellum, internal capsule/ assoc with uncontrolled HTN, DM.
lacunar infarct
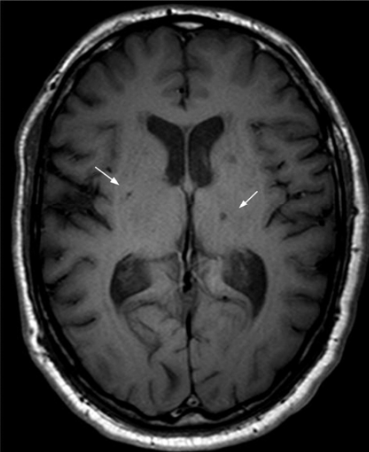
pt has pure contralateral motor deficits, pure c/l sensory deficits, ipsilateral ataxia, dysarthria with hand clumsiness.
lacunar infarct
prognosis of lacunar infarct
deficits stabilize withing 24-36 hrs and generally have good prognosis at small size
obstruction of carotid circulation causes what infarcts
ACA, MCA, ophthalmic artery or central retinal
pt has contralateral hemiparesis and hemisensory loss of the lower extremity. may be a contralateral grasp reflex, marked confusion, apraxia. urinary incontinence
anterior cerebral artery infarct
b/l ACA occlusions tend to lead to what sx
marked behavioral changes and memory loss
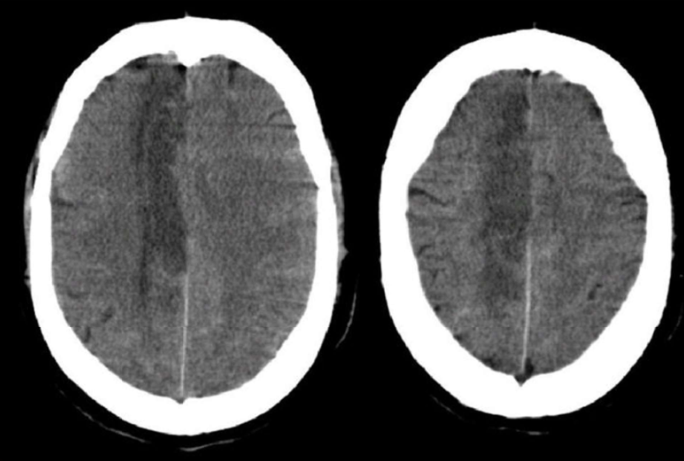
pt has contralateral hemiplegia, hemisensory loss, and homonymous hemianopia (b/l symmetric loss of vision in half the visual fields) w eyes deviated to side of lesion
MCA infarct
MCA infarct leads to a large risk for
hemispheric swelling, stupor, coma, confusion
anterior division of MCA infarct produces what sx
expressive aphasia (Broca’s), c/l paralysis and sensory loss to face and arm, lesser so the leg. these pts understand you but can’t communicate
posterior division of MCA infarct produces what sx
receptive aphasia (wernicke’s) and homonymous visual field defect. these pts can’t comprehend what you’re saying
inability to formulate or comprehend language
aphasia
lesions fo left frontal lobe, inability to express language, motor problem and not fluent, stutter and can’t formulate words
Broca’s aphasia
lesions of left superior temporal lobe, inability to understand language, fluent, “word salad”, use real words but continuous flow of nonsensical sentences
wernicke’s aphasia
this infarct leads to sudden painless visual loss with retinal pallor and a macular cherry red spot on fundoscopic exam. pts get sudden transient vision loss in one eye (amaurosis fugax) is a TIA in this arterial territory
ophthalmic artery infarct
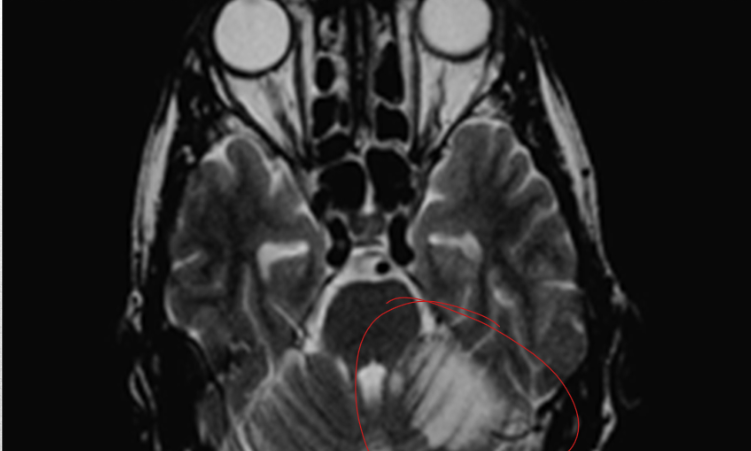
obstruction of the vertebrobasilar circulation causes these arteries to infarct
posterior cerebral artery, vertebral artery, basilar artery, cerebellar artery
this infarct leads to thalamic syn leading to c/l hemisensory disturbances followed by the development of spontaneous pain and hyperpathia (exaggerated levels of pain). pts usually have macular sparing homonymous hemianopia
PCA infarct
this infarct may be clinically silent bc circulation is maintained by the other vertebral artery
vertebral artery infarct, distally below level of anterior spinal and posterior inferior cerebellar arteries
when one of these arteries is occluded it causes sx like ipsilateral sensory loss of the face, limb ataxia and numbness, vertigo, nystagmus, and Horner’s syn (ptosis miosis anhidrosis)
posterior inferior cerebellar artery or vertebral artery
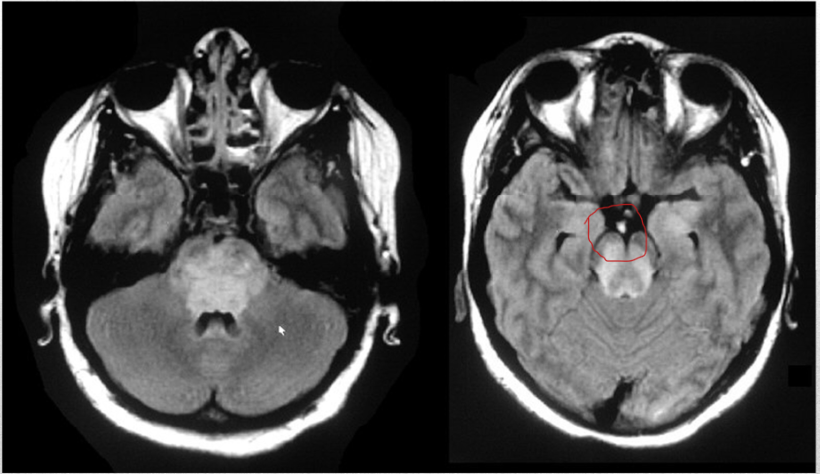
occlusion of this artery leads to coma with pinpoint pupils, flaccid quadriplegia, and sensory loss, and variable CN abnormalities
basilar artery infarct
occlusion of these arteries leads to vertigo, n/v, nystagmus, ipsilateral limb ataxia, and contralateral spinothalamic sensory loss of the limb. if massive infarction occurs then this can lead to coma, tonsillar herniation and death
cerebellar artery infarct
13 item scoring system that integrates neuro exam, language, and levels of consciousness that indicates severity of neuro dysfxn. score of 1-4 of minor stroke, 5-15 = moderate, 15-20 = moderately severe, >20 = severe
NIH stroke scale
what imaging should be preformed immediately before giving ASA or other antithrombotic agent to exclude cerebral hemorrhge
non contrast head CT
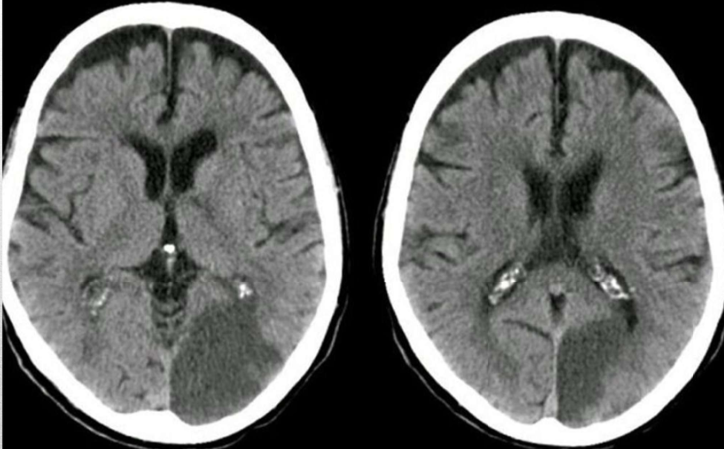
bc a CT is insensitive to acute ischemic strokes in the first 6-12 hours this imaging is then indicated
MRI with diffusion weighted sequences
what is the usefulness of an MRI in a stroke pt
defines the distribution and extent of infarction as well as exclude tumor or other differential considerations.
if pts present within 6 hrs of stroke onset what imaging is used and why
CTa of head and neck. identify large vessel occlusions amenable to endovascular therapy
regardless of timing of presentation imaging of the cervical vasculature needs to be done to identify the source of stroke using what imaging
CTa, MRa, carotid duplex US, conventional catheter angiography
what labs do you order in a stroke pt
CBC, ESR, CMP, coagulation profile, lipid profile, HgA1c, protein C/S; antithrombin abnl (inc risk of clot), homocysteine level, APLS labs - anticardiolipin, lupus anticoagulant (recurrent clot formation)
how to tx stroke
main goal is to dissolve the clot. give IV TPA within 3 hours of onset of stroke sx. can give in 4.5 hrs if meets criteria and not over 80, diabetic with previous stroke, or severe disability. improves recovery and dec long term disability