Applanation Tonometry
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
Describe the Imbert-Fick principle
When a flat surface with a defined area is pressed against the surface of a sphere (applanation) with a given internal pressure
Equilibrium is reached when the force exerted is balanced by the internal pressure
Equation Imbert Fick principle
The force required to flatten the surface of a sphere (W) Is equal to product of the pressure inside the sphere (P) and the area is applanated (A)
> W = P x A
what does the equation assume (W = P x A)
only true assuming cornea is thin , dry , perfectly elastic and flexible
and only force acting on the surface should be the pressure of the applanating surface
GAT uses the Imbert Fick principle but takes 2 other conditions into account - What are they ?
Surface tension (S) of the tear film which attracts the tonometer prism towards the cornea
Corneal rigidity (B) which resists applanation
What did Goldmann and Schmidt determine ?
if area being applanated was 3.06mm2 these two forces cancel out
W + S = (P xA) -B
Consent before GAT
Explain test to px beforehand
Obtain informed consent
Ask about sensitivity to anaesthetic drops
Anaesthetics
inform px drops will sting at first → this should dissipate quickly
Add a drop to each eye
After a minute add second drop to each eye → should not feel second drop if you’ve correctly inserted first drop
(drops act fast)
Slit lamp set up for GAT
need to place GAT on stage
Stage and GAT need to be secure → clicks in place
insert and align probe with white line on carrier
What do we do if conceal astigmatism greater than 3.00D
An error of 1mmHg for every 4.00D of corneal astigmatism
can use keratometer
What to do if astigmatism is WTR or ATR
move to the red line on the carrier
What to do if astigmatism is oblique ?
needs to be 43 degrees from FLATTEST meridian
Keratoconus px etc
What is the slit lamp set up for GAT
Mag 10-16x
Angle 45-60
WIDEST beam
Cobalt Blue Filter + Wratten
High illumination
Fluorescein instillation
FI need to be instilled safely
makes mire easier to see
Aim not to put too much as this will affect quality of mires → wait for the fluorescein to wash out
Patient instructions during GAT
ask px to keep STILL as possible
need to keep head right up against forehead rest
ensure slit lamp is at right height for px prior to GAT
ask them to look straight ahead and encourage them not to blink
readings can be higher in anxious px - reassure px
Applanating
set tonometer to expected result
gently move slit lamp forward
LOOKING AROUND SIDE of slit lamp until applanation occurred
will see tonometer probe head move back when applanated
What type of probe is the GAT probe ?
Biprism
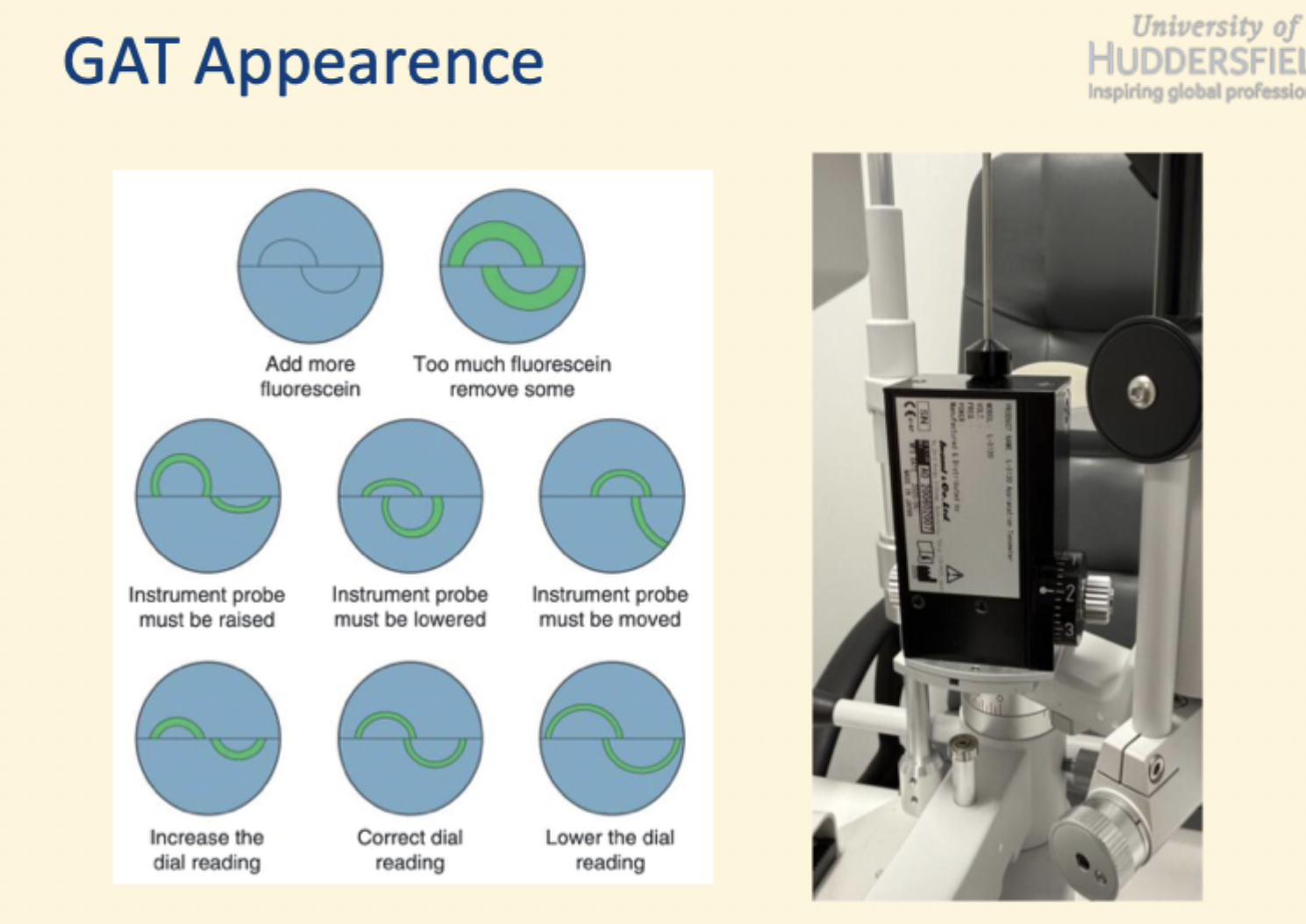
GAT appearance when to adjust
What to do post GAT
Check corneal integrity after GAT → optic section
ensure any staining not affecting stroma
How to record GAT
Need to record :
> Techniques
> IOP measurements (each eye)
> TIME
E.g .GAT R 21, L22 @3:00pm
How to calibrate GAT
metal thing
check at 0,20 and 60
should be calibrating once a month
Perkins - which px
similar to GAT but different patient setup
useful for px that are unable to use a slit lamp
domiciliary px
its handheld, portable and has head rest
What is Pachymetry
Green word → Pachos-thick and “metry” to measure
is the term used for measurement of corneal thickness
When to perform Pachmyetry
Patients with ocular hypertension
When IOP measured
Refractive surgery → what type is most suitable for px
screening + monitoring of
> Corneal oedema
> Corneal dystrophies
> Kerataconus
CCT and ocular hypertension
Application based on Imbert Ficks law which assumes cornea is a perfect flexible, dry sphere which is thin
increase in tissue in thicker cornea makes it less compliant and leads to overestimation of IOP
thinner cornea leads to underestimation of IOP
Ocular Hypertension Treatment study published
OHTS published that CCT important independent risk factor for progression from ocular hypertension to early glaucoma
With the Goldman Tonometer what does it assume Corneal Centre Thickness to be ?
> 520μm
What do other tonometers assume CCT?
545 or 550 μm
If CCT higher than that assumed by tonometer device will OVERESTIMATE the px IOP
If CTT lower than that assumed by tonometer the device will UNDERESTIMATE px IOP
What are the different types of Pachymetry ?
> Ultrasound Pacymetry
> Ultrasound Biomicroscopy
> Optical Pachymetry
> OCT
> Schemipflug imaging
What is a Tongue -P
Uses Schemipflug Camera
calculates a compensated IOP measure
Recording
Techniques
CCT measures of each eye
Time (time of day can affect CCT)
- > E.g GAT R 555μm L 560 μm @ 3:00pm