Lecture 3: Regulation of osmolarity by regulation of H2O reabsorption (ADH), regulation of volume by regulation of Na+ reabsorption (RAA, ANP, and BNP)
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
what’s the other name for ADH
vasopressin
AQP2 is regulated by
ADH
water reabsorption is
solute-free. it dilutes the plasma, decreasing Posm toward normal
when water is added to ECF, why does plasma volume not change significantly?
constant shift between ECF and ICF (which holds 2/3 of total body water)
what are the regulators of ADH release
increased osmolarity (most important)
decreased arterial pressure (arterial baroreceptor input)
low blood volume
effect of alcohol on ADH release
inhibits ADH release (increased urination b/c water isn’t being reabsorbed)
vasoconstrictor effect on vascular smooth muscle is only at
high levels of ADH
effect on kidneys is at
all levels of ADH
ADH controls kidney/CD h2o reabsorption via
high affinity V2 receptor, meaning strong effect at low levels of ADH
ADH acts as a vasoconstrictor on vascular smooth muscle via
low affinity V1 receptor
ADH secretion is most sensitive to which change (plasma osmolarity, volume, pressure)?
osmolarity
explain what happens with high plasma Osm and urine concentration
high plasma Osm
high ADH
high water reabsorption in CD
high solute free water reabsorption
dilutes plasma osm toward normal
excretion of highly concentrated urine
explain what happens with low plasma Osm and urine concentration
low plasma Osm
low ADH
low water reabsorption in CD
high solute-free water excretion
concentrates plasma Osm toward normal
excretion of a highly dilute urine occurs
where is ADH secreted
hypothalamic neurons in the posterior pituitary
what is the primary sensory input for ADH secretion
osmoreceptors in the hypothalamus
where are arterial baroreceptors located
aortic arch and carotid arteries
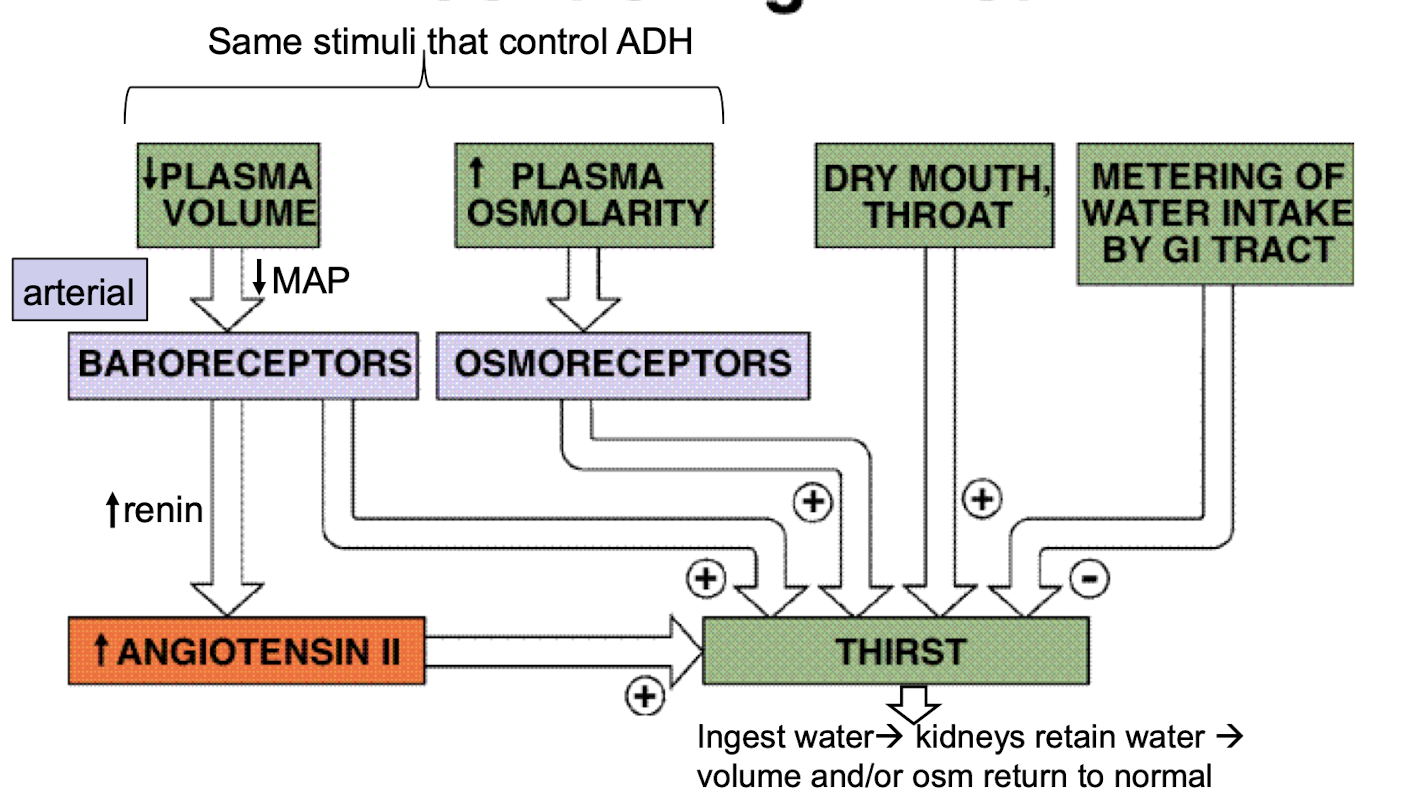
how is thirst mechanism regulated
decreased plasma volume → decreased MAP → arterial baroreceptors → increased renin → increased angiotensin II → thirst
increased plasma osmolarity → osmoreceptors → thirst
Na+ excretion equation

regulation of ECF volume occurs via
changes in Na+ excretion which cause changes in H2O excretion (because H2O follows Na+)
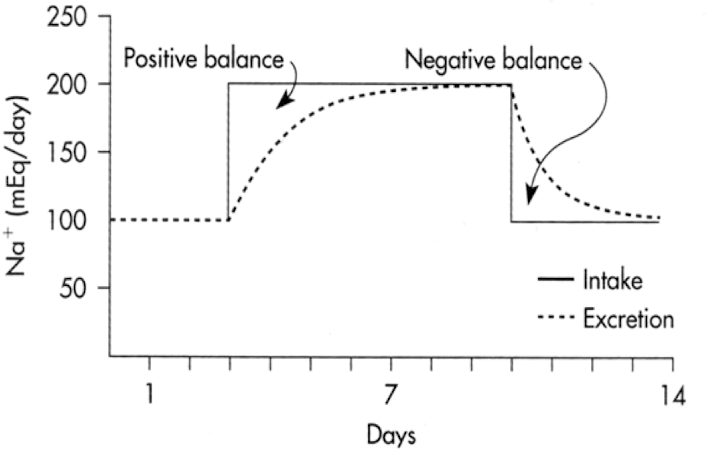
what is the relationship between Na and ECF volume
increased NaCl load → increased volume as measured by body weight (initial response)
regulation of Na+ excretion occurs in response to changes in
blood pressure via an arterial baroreceptor-mediated response
how is Na+ reabsorption regulated on proximal tubule
increased by angiotensin II
how is Na+ reabsorption regulated on distal tubule
increased by angiotensin II
how is Na+ reabsorption regulated on collecting duct
increased by aldosterone
explain mechanism of renin secretion via extrarenal control
increased sympathetic activity → increased renin secretion by juxtaglomerular cells
explain mechanism of renin secretion via intrarenal control
decrease pressure in afferent arteriole → intrarenal baroreceptors on juxtaglomerular cells respond → increased renin secretion
explain mechanism of renin secretion via NaCl delivery
constriction of afferent arterioles → low GFR → low NaCl delivery to macula densa cells → altered paracrine factors (e.g., decreased ATP and adenosine, increased prostaglandins) → increased renin release
renin-angiotensin-aldosterone (RAA) system
action of aldosterone on late distal tubule/cortical collecting duct cell
aldosterone combines with a cytoplasmic receptor
initiates transcription in nucleus
increased ROMK (Renal Outer Medullary K+) channel and increased ENaC (epithelial sodium channels) on apical membrane
increased Na/K pump on basolateral membrane
result is increased Na+ reabsorption and K+ secretion
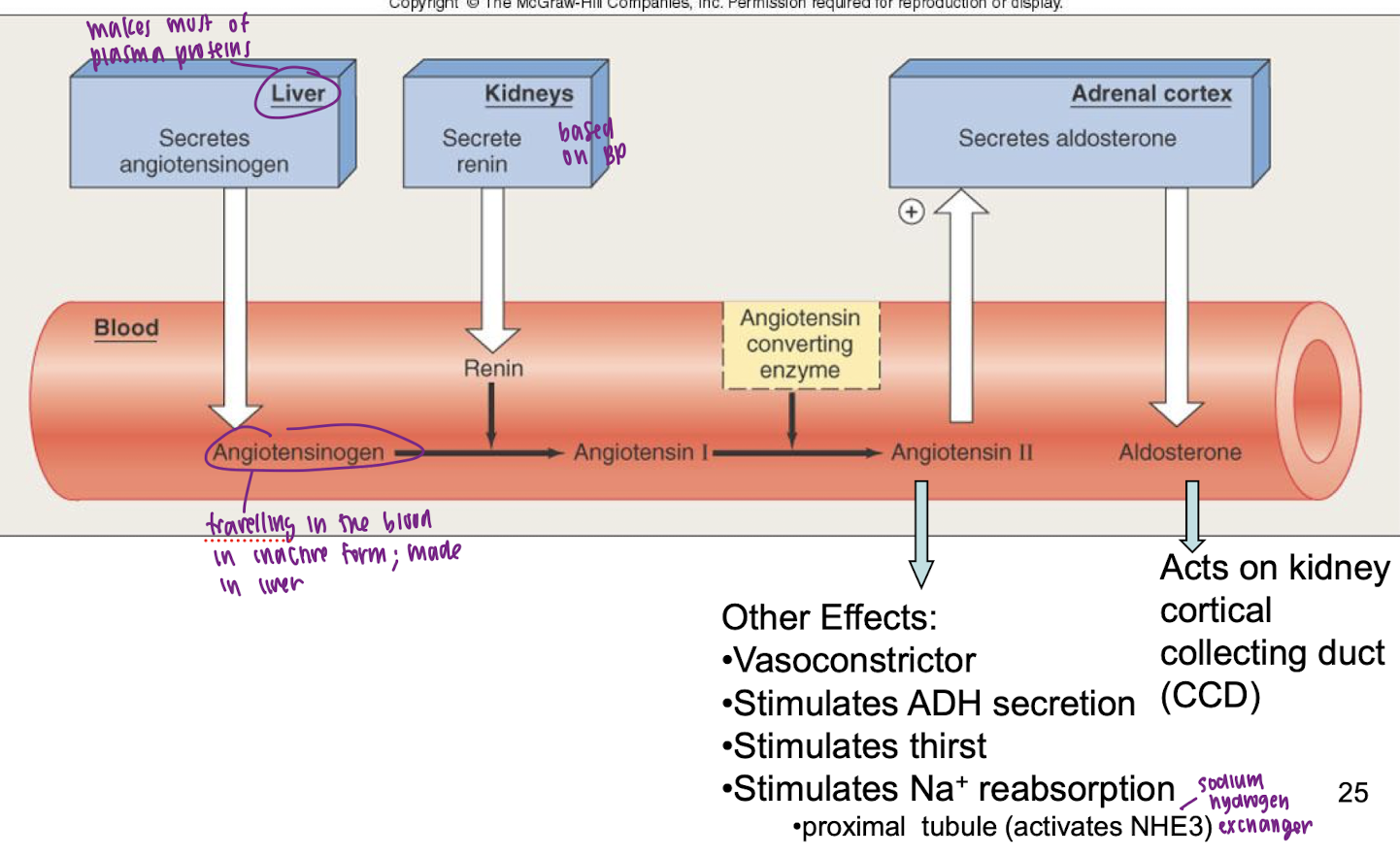
renin
hormone (enzyme) released from kidney and is the rate limiting step in the conversion of angiotensinogen to angiotensin II in the plasma
angiotensin II
peptide generated in the plasma and tissue compartments; stimulates aldosterone secretion, Na reabsorption (proximal tubule via NHE3, Na+/H+ exchanger), thirst, ADH secretion, and vascoconstriction
aldosterone
steroid hormone released from adrenal gland; stimulates Na+ reabsorption in the cortical CD of kidneys (by activating ENaC and Na+/K+ ATPases)
does blood volume have to drop for pressure to drop?
No. Heart attack or failure → decreased SV and MAP… however blood volume is unchanged
ECF osmolarity is regulated by
primarily controlling water excretion via alterations in ADH secretion
ECF volume is regulated by
altering the reabsorption and excretion of BOTH Na+ and H2O via RAA and ADH changes
what increases ANP secretion
increased atrial distension
what increases BNP secretion
increased ventricular distension
what happens after increased ANP and BNP
increased GFR → decreased renin → decreased Ang II → decreased aldo and ADH → reduced Na+ and H2O reabsorption → increased sodium and water excretion → volume decreases toward normal
ANP change is NOT due to ________, it is due to __________
increased MAP, it is due to increased VR and EDV, which are often caused by increased volume