8/9 - retinal vaso-occlusive disease starting with CVOS
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
What is the typical etiology of CRVO?
thrombus
What blood work should you order for retinal vascular occlusions?
1. blood pressure
2. FBS or HbA1C
3. lipid profile
4. platelet count
5. CBC with differential
6. ESR or C-reactive protein
7. other coagulation tests
what is usually preceded before a CRVO?
transient blurring of vision
What disease is the number one cause of a CRVO?
HTN
Which type are majority of CRVO?
non-ischemic/incomplete - 70-75%
what can severe hypoxia lead to?
retinal neovascularization → unlikely because not enough circulation
What devastating effect can iris neovascularization cause?
(90-day or 100-day) neovascular glaucoma that causes the entire eye/vision to be lost
When does neovascular glaucoma following CRVO usually occur?
3-5 months after (90 or 100 day glaucoma)
~8% (~17% in ischemic CRVO)
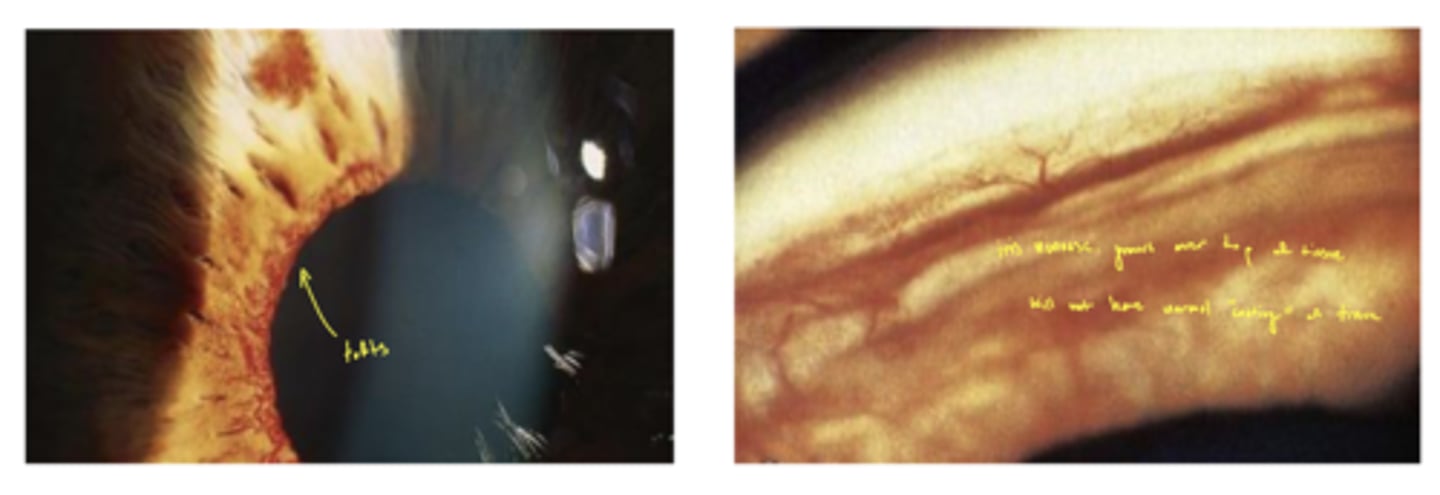
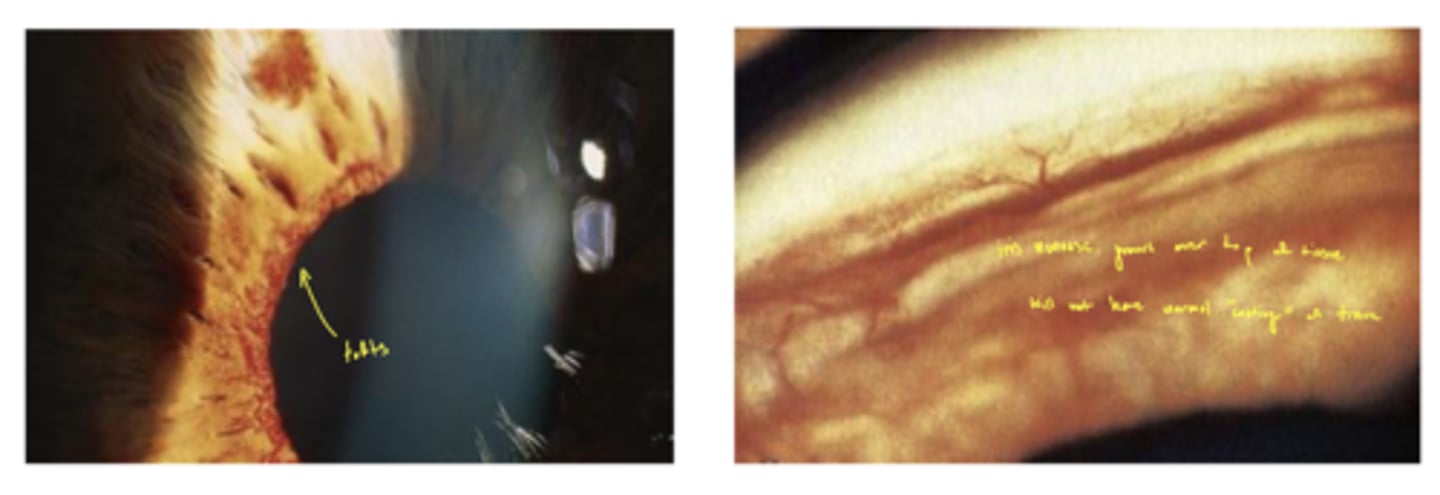
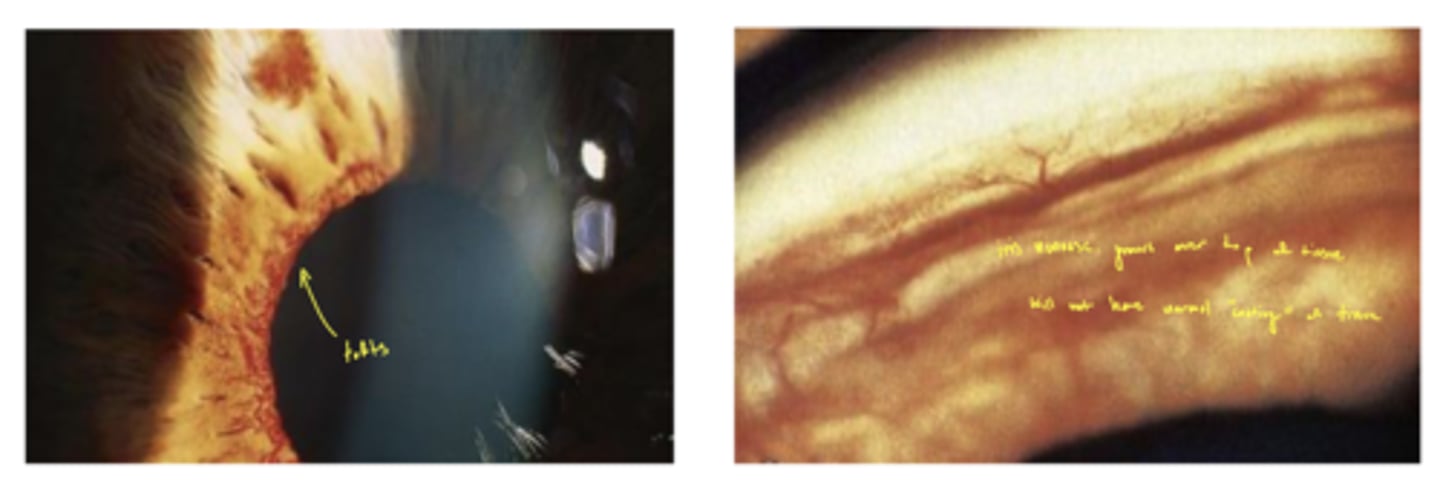
What are the vessels on the iris called during neovascular glaucoma?
tufts (in the left image)
What is the main cause of a CRVO?
thrombus
What are the causes of a CRVO?
thrombus
anything creating pressure on central retinal vein → glaucoma, tumor, FB
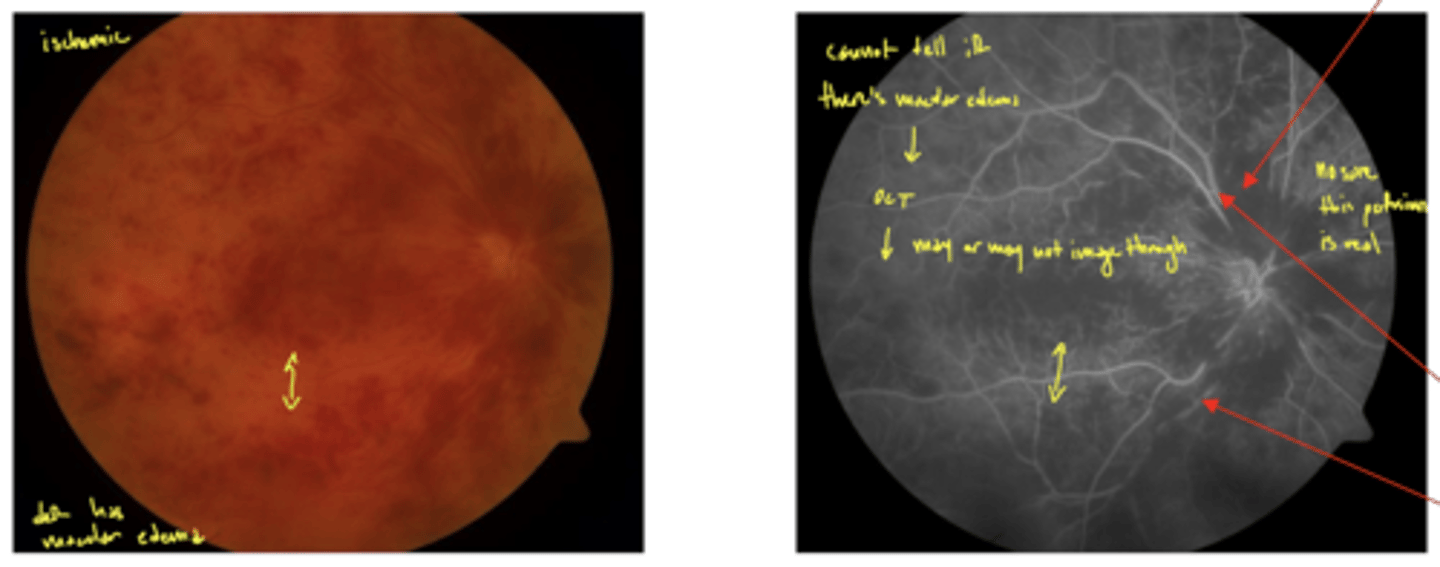
What is the only definitive way to tell the difference between non-ischemic and ischemic venous occlusions?
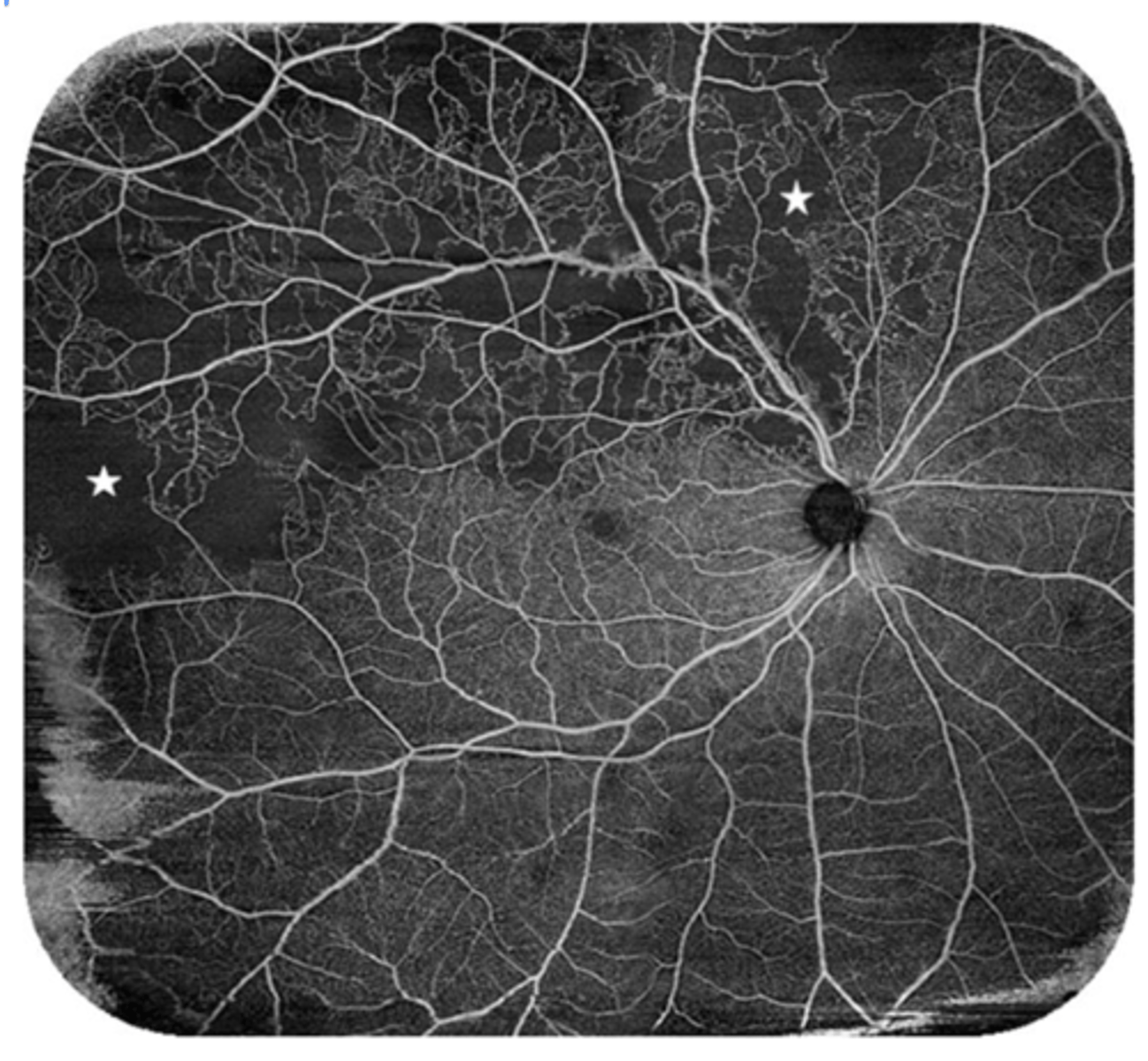
FANG → hard to do early because too much blood it covers everything
may need to use OCT to see if there's macular edema
image - ischemic CRVO that shows FANG (low perfusion)
Ischemic CRVO has lost at least how much retinal perfusion?
at least 10 DD
what are the 2 classifications of a CRVO?
1. nonischemic retinopathy (venous stasis retinopathy or incomplete CRVO)
2. ischemic retinopathy (hemorrhagic or complete CRVO)
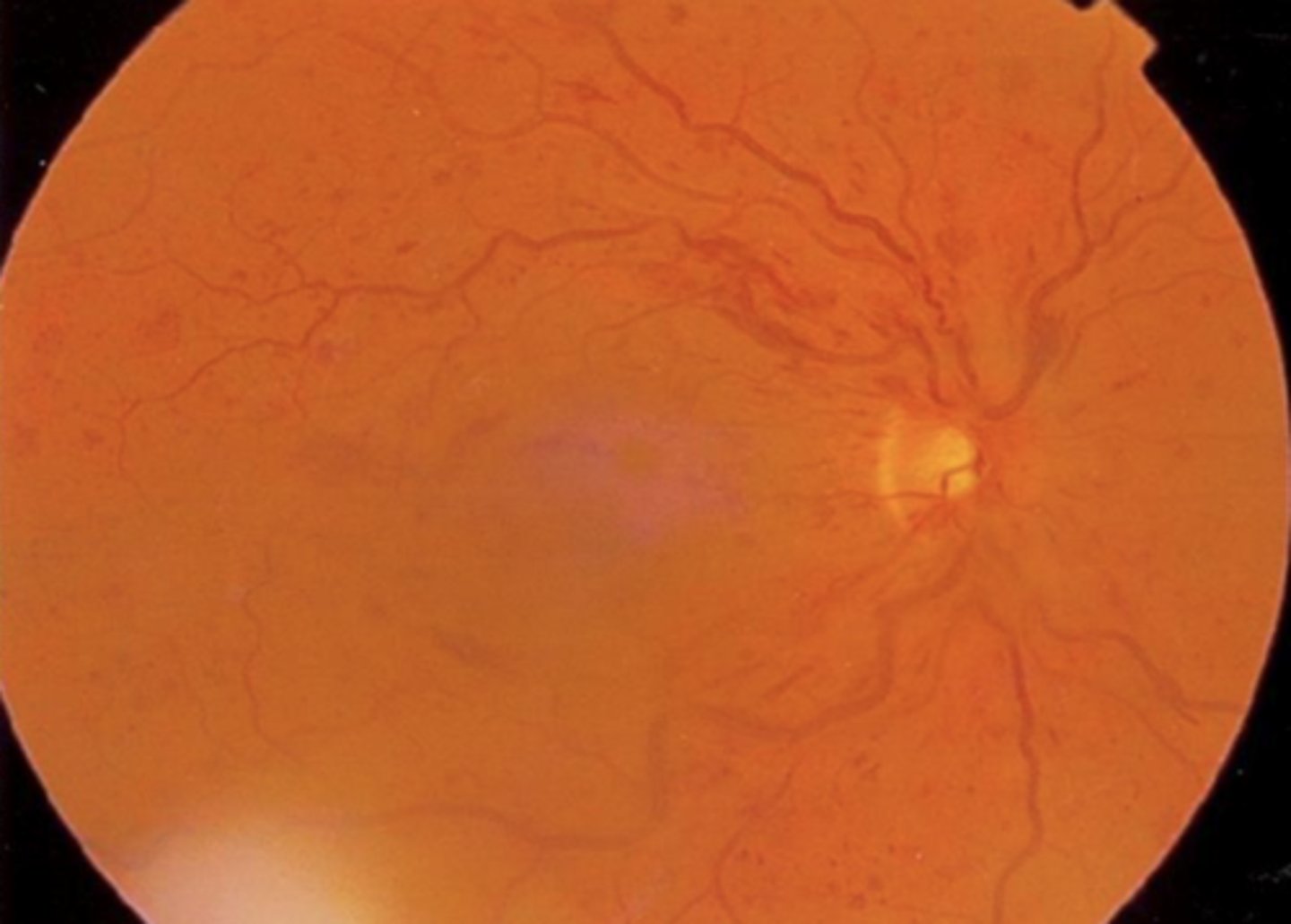
What are the characteristics of non-ischemic CRVO?
1. dot-blot and flame-shaped hemes
2. intraretinal edema
3. various degrees of macular + ONH edema
What are the characteristics of ischemic CRVO?
1. more dot-blot + flame hemes
2. CWS
3. significant macular + ONH edema
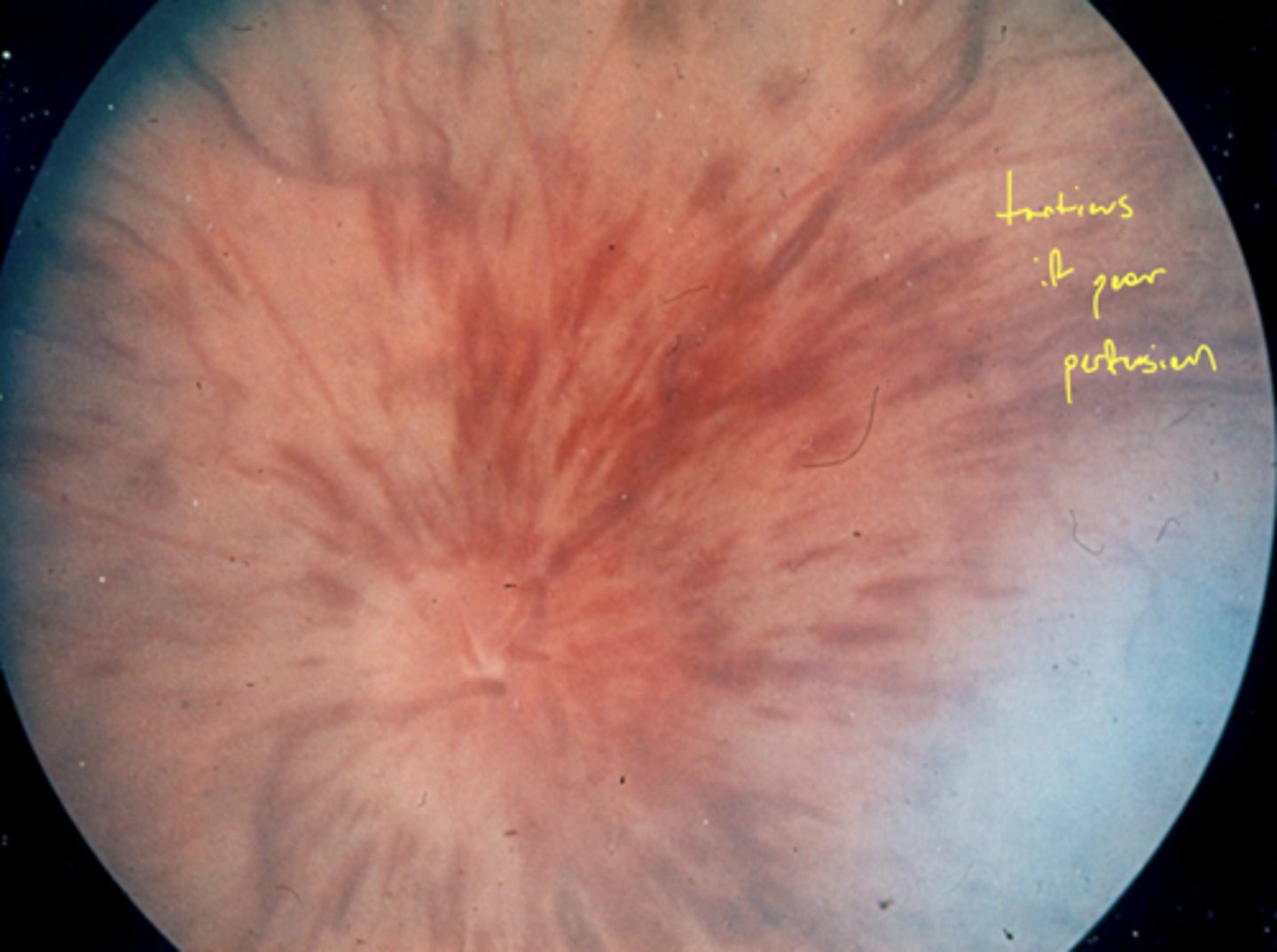
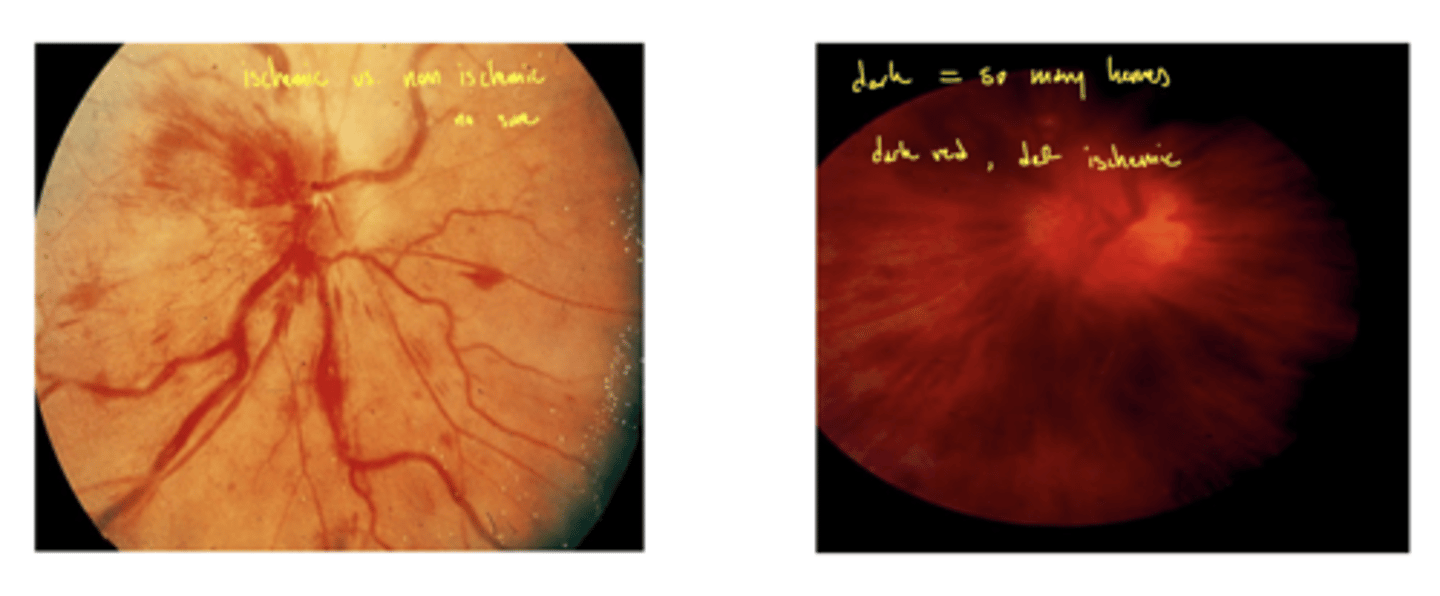
What fundus characteristic makes you sure the CRVO was ischemic?
dark blood red fundus
left - not sure which type
right - must be ischemic
What does CRVO look like on OCTA?
dark areas = non-perfusion (capillary dropout)
Which type of CRVO is more likely to develop neovascular glaucoma (NVG)?
ischemic CRVO
what is the pathology of iris neovascularization formation?
1. new vessels grow at iris because little or no viable capillary tissue in retina
2. iris has a lot of viable vascular tissue
3. new vessels sprout and vessels obstruct (described as coating) TM → ↑ IOP
4. iris neovascularization starts around pupil and grows toward the angle, lays on top of the iris tissue
What are the post-CRVO findings?
1. ONH shunt/collateral
2. retinal collaterals
3. vascular sheathing
4. vascular tortuosity
What is the management of CRVO?
1. refer to retina → patient should be seen in 1 day (bc of macular edema)
2. perform FANG
3. refer for systemic vascular workup in 3-5 days
How many anti-VEGF injections does the average DME or CRVO patient receive?
7-8 injections
how to tell if neovascularization or collaterals?
collaterals cross the horizontal raphe
neovascularization DOESN'T
What did the central vein occlusion study (CVOS) show?
1. laser photocoagulation does not work for macular edema due to CRVO (group M)
2. prophylactic PRP did not prevent NVI in CRVO (group N) - wait until NVI to do PRP
3. if an eye has such extensive intraretinal hemorrhages and you cannot see the macula → assume ischemic CRVO (group I)
group M = macular
group N = neovasc.
group I = indeterminate
what is the management for macular edema in CRVO?
although CVOS says to monitor → optometrists REFER since the advent of anti-VEGF medications
anti-VEGF treat the macular edema
What is the treatment for CRVO with retinal neovascularization from CVOS?
anti-VEGF meds ± PRP
what is the tx for CRVO with iris neovascularization from CVOS?
PRP ± anti-VEGF meds
what were the results for group M in CVOS?
macular grid photocoagulation ↓ macular edema but didn't improve VA in eyes with reduced vision caused by macular edema
what were the results for group N in CVOS?
prophylactic PRP did not prevent iris neovascularization → safe to wait for early iris neovascularization development and then do PRP
what were the results for group I in CVOS?
eyes with extensive intraretinal hemorrhage act as if they are ischemic or nonperfused
What did the SCORE study show for CRVO?
intravitreal steroids work for CRVO macular edema → can be used as treatment despite high side effects
not used anymore since the dawn of anti-VEGF treatment
what did the CRUISE study show for CRVO?
intravitreal anti-VEGF became standard of care for macular edema in CRVO
Does anti-VEGF work better for BRVO or CRVO?
BRVO
what is the ophthalmologic management for CRVO?
1. anti-VEGF for long-term
2. anticoagulants in acute phase
3. PRP → ↓ retina hypoxia → ↓ vasoproliferative stimulus → ↓ iris neovascularization
what is a hemicentral retinal vein occlusion (also called altitudinal BRVO)?
only 1 hemisphere of the retina is affected → superior or inferior to the horizontal raphe
what are the characteristics of a hemicentral retinal vein occlusion?
same as CRVO and BRVO but affect 1 hemisphere of retina:
1. dot-blot and flame shaped hemes
2. retinal neovascularization
3. macular edema

When does retinal neovascularization develop in a hemi-retinal vein occlusion?
3-6 months
What is the management for a hemiretinal vein occlusion?
same as CRVO:
1. refer to retina + patient should be seen in 1-2 days (bc of macular edema)
2. refer for systemic vascular workup in 3-5 days
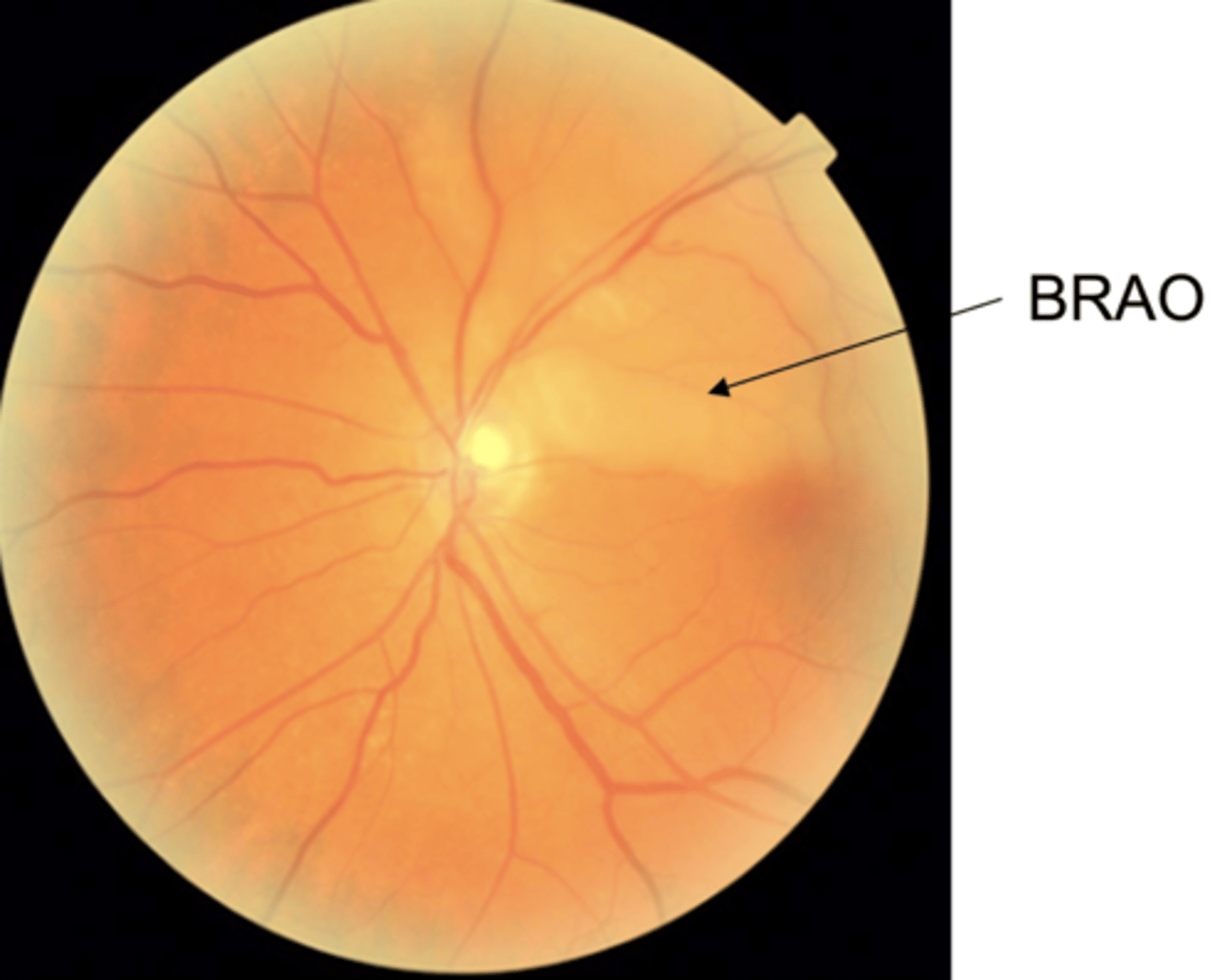
What causes a BRAO?
emboli dislodged from vasculature elsewhere in body; typically the heart or the carotids
what are the emboli in a BRAO comprised of?
1. cholesterol
2. calcium
3. crystals of a drug (iv drug use/abuse)
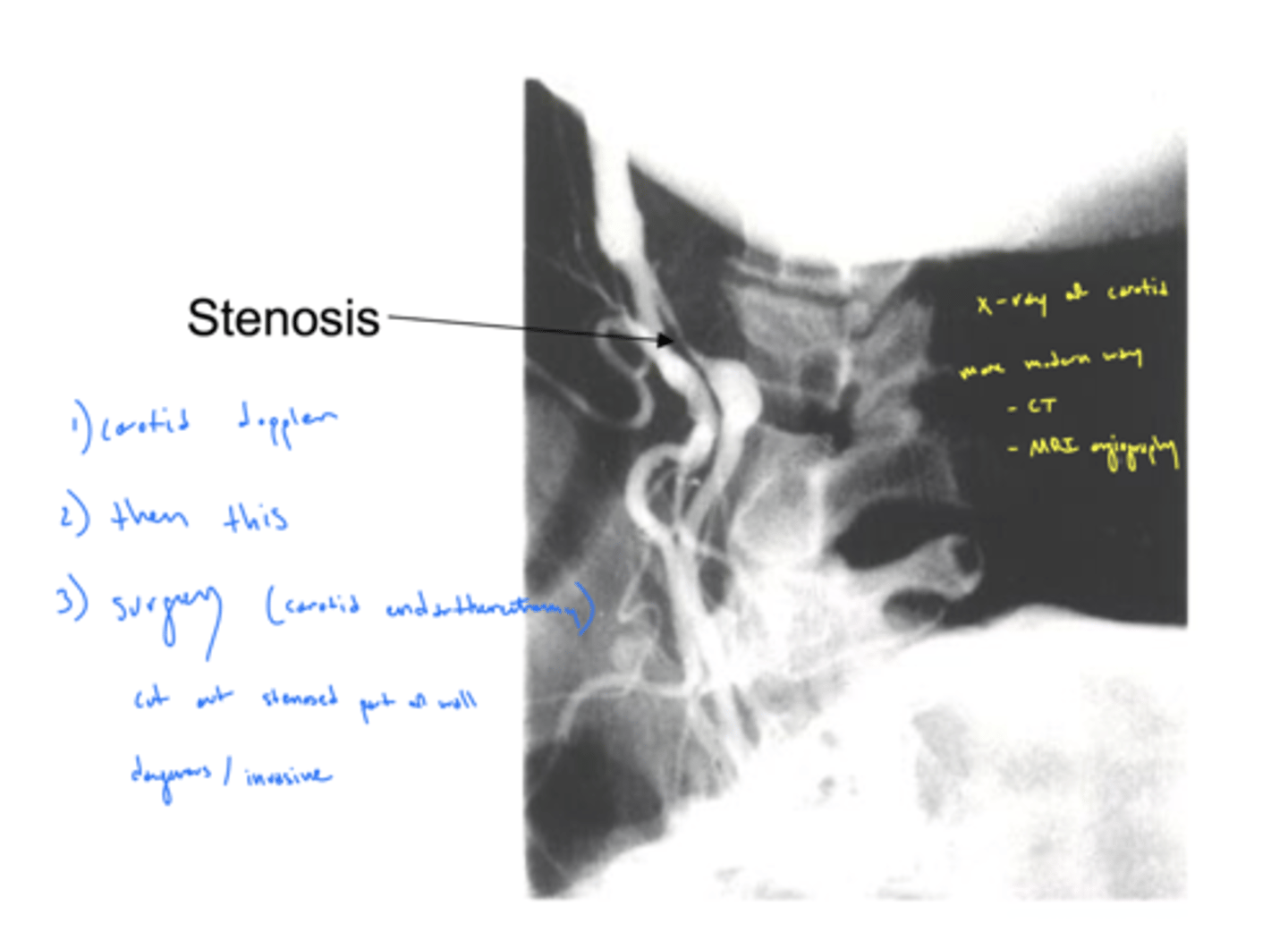
how to evaluate the patency of carotid arteries?
stethoscope (carotid bruit) → blood flow creates friction as move across materials deposited in vessel walls
listen for turbulent blood flow (have patient hold their breath)
What symptom is BRAO often associated with?
amaurosis fugax (transient monocular blindness)
Why are BRAO an emergency?
rapid anoxia of inner retina
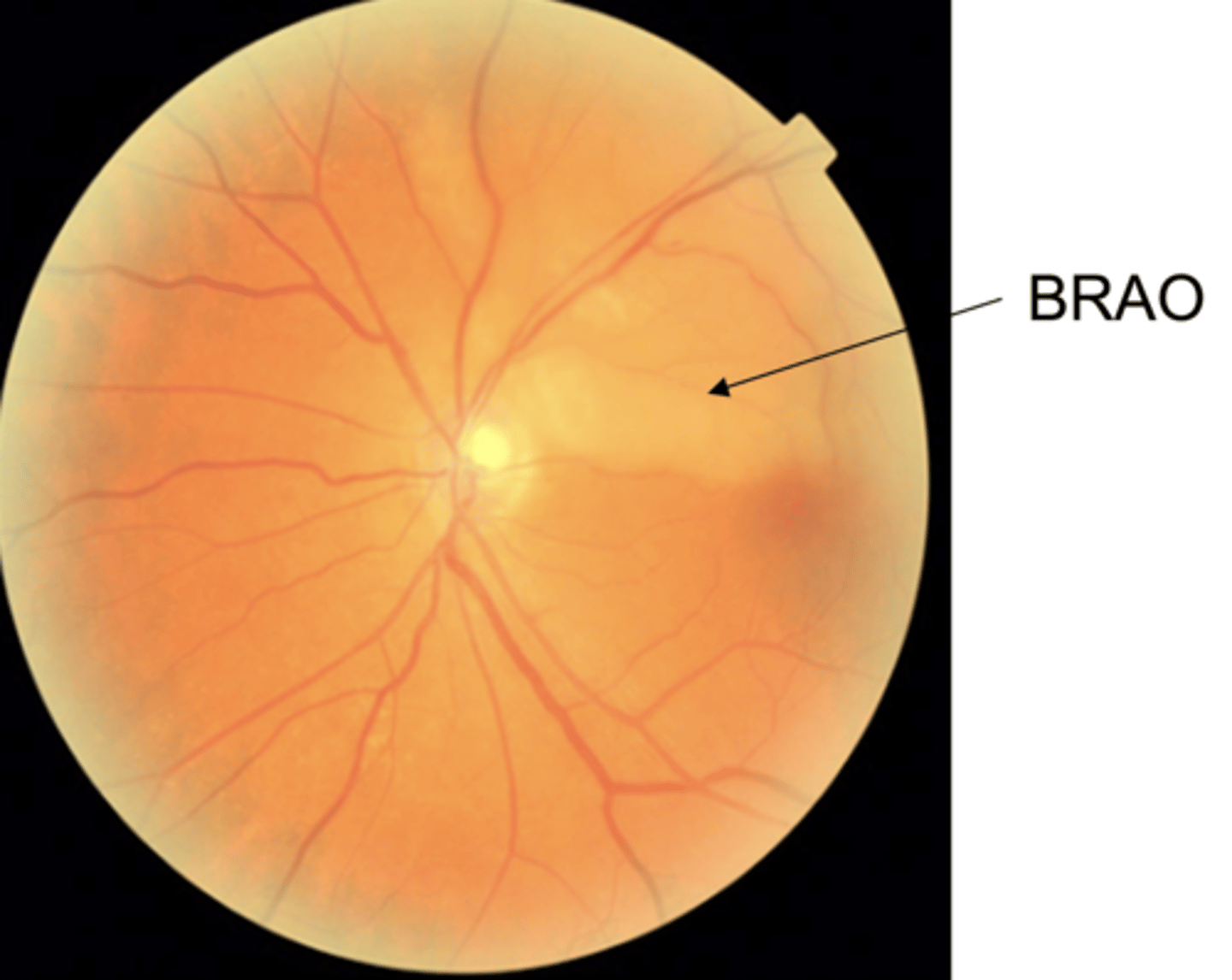
cause anoxia that causes loss of inner retinal layers (NFL, GCL, IPL, INL) - retinal tissue changes from hazy to white in a few hours
image would be considered hemicentral technically
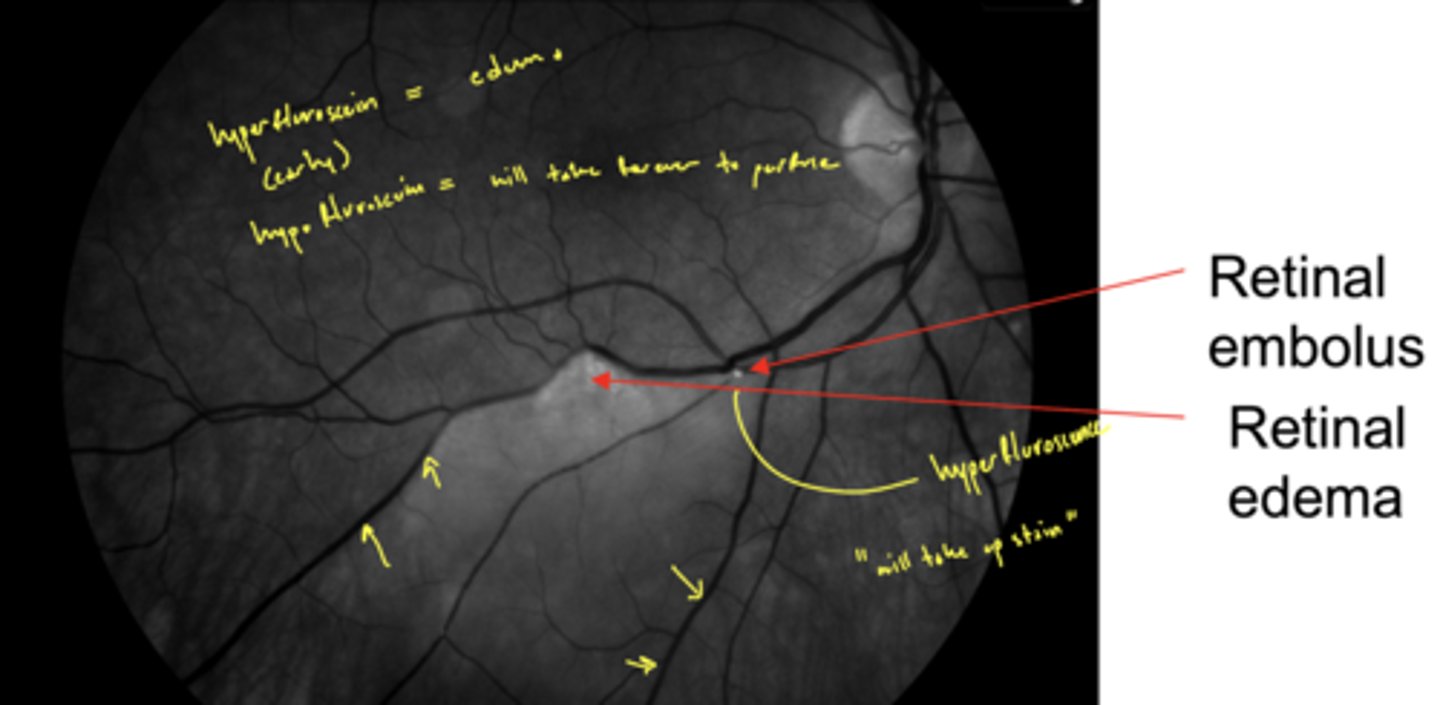
What does a BRAO look like on FANG?
hyperfluorescence (from edema) early on as occluded blood vessel leaks
then eventually hypofluorescence
What is the most commonly affected area in a BRAO?
superior temporal
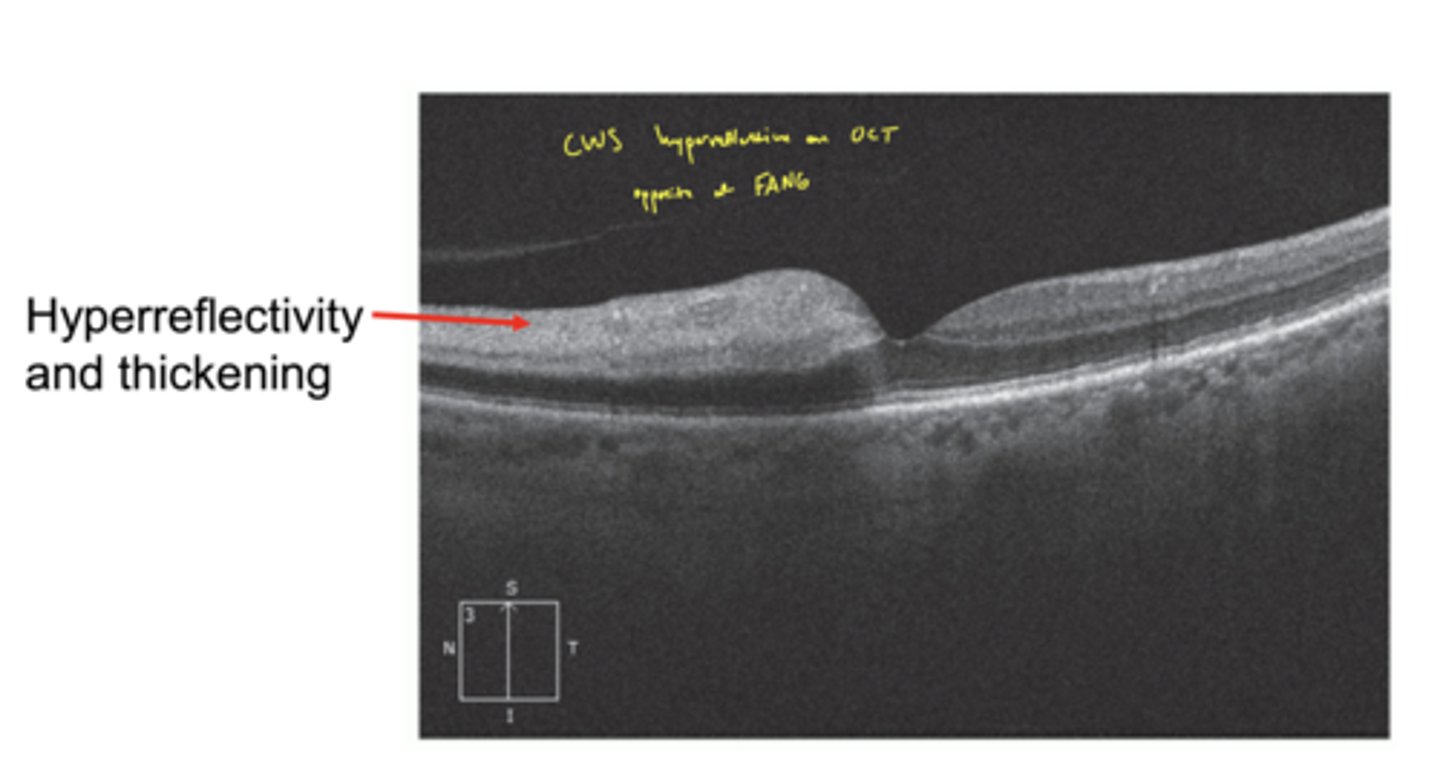
What does BRAO look like on OCT?
hyperreflectivity and thickening
think CWS on OCT
What is the management for a BRAO?
1. send to ER
2. get systemic (carotid and cardio) workup
What is the threshold for treatment of a BRAO before vision loss is lost (cannot be restored)?
>4 hours restoration of vision is unlikely
What causes a CRAO?
emboli lodges in CRA as it passes through the lamina
What does a CRAO cause?
sudden (in seconds) painless loss of entire vision
Why does a CRAO cause loss of entire visual field if the fovea still has a blood supply?
relay from fovea to ONH is dead
may be a loss of a direct pupillary response
fovea is still getting blood from the choroid
When may a patient with a CRAO still have a small island of vision left?
if they have a cilioretinal artery
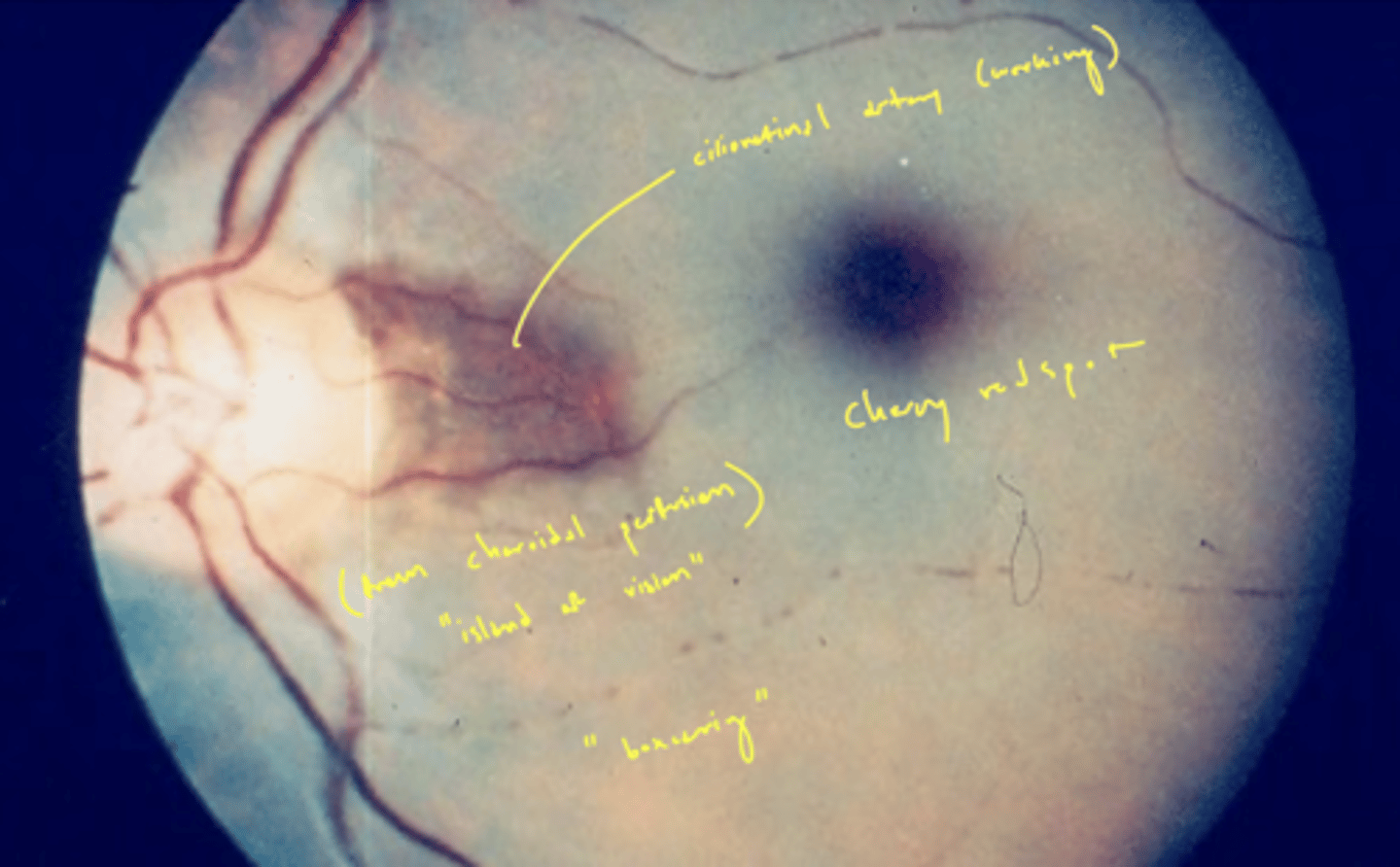
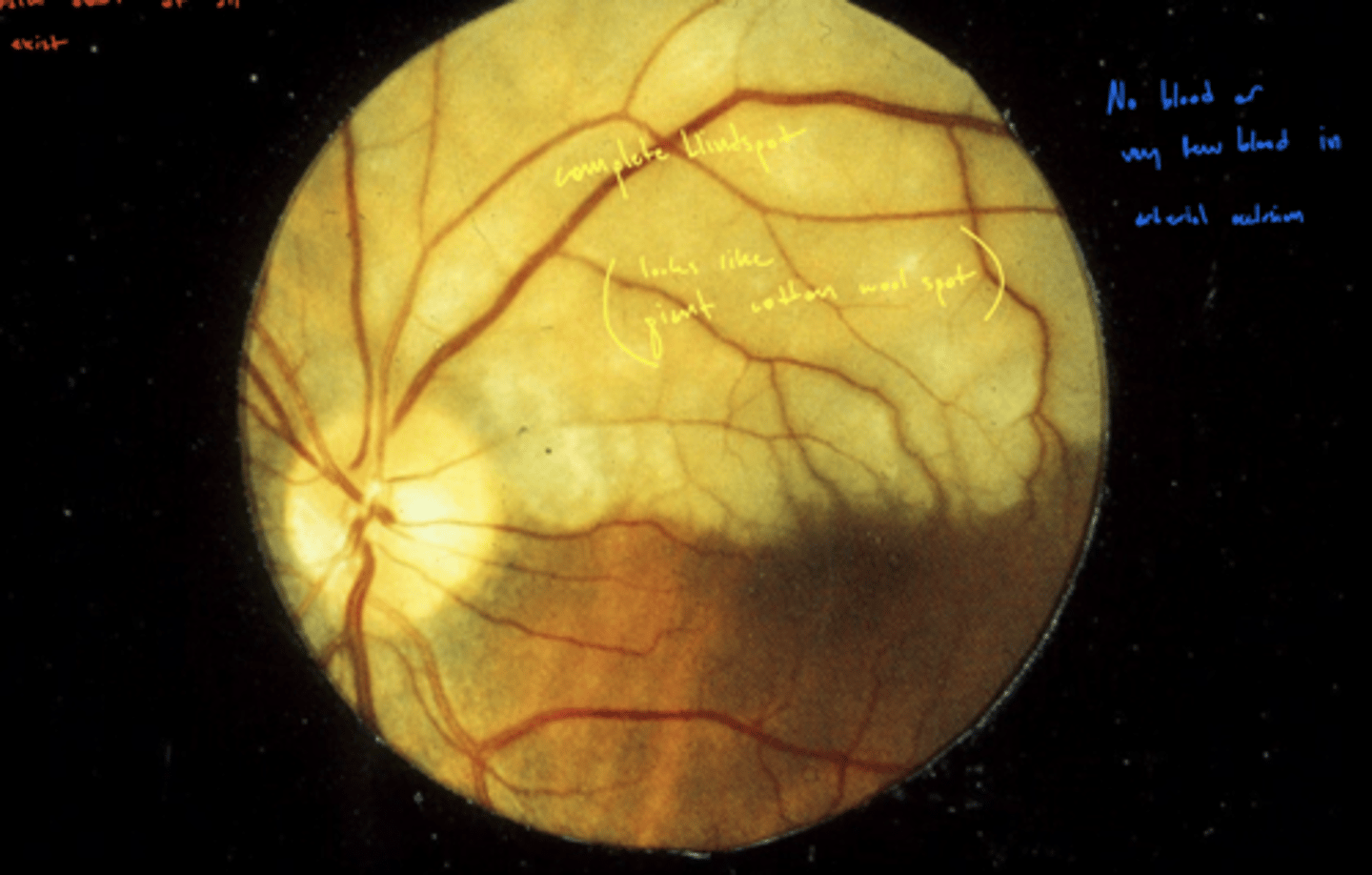
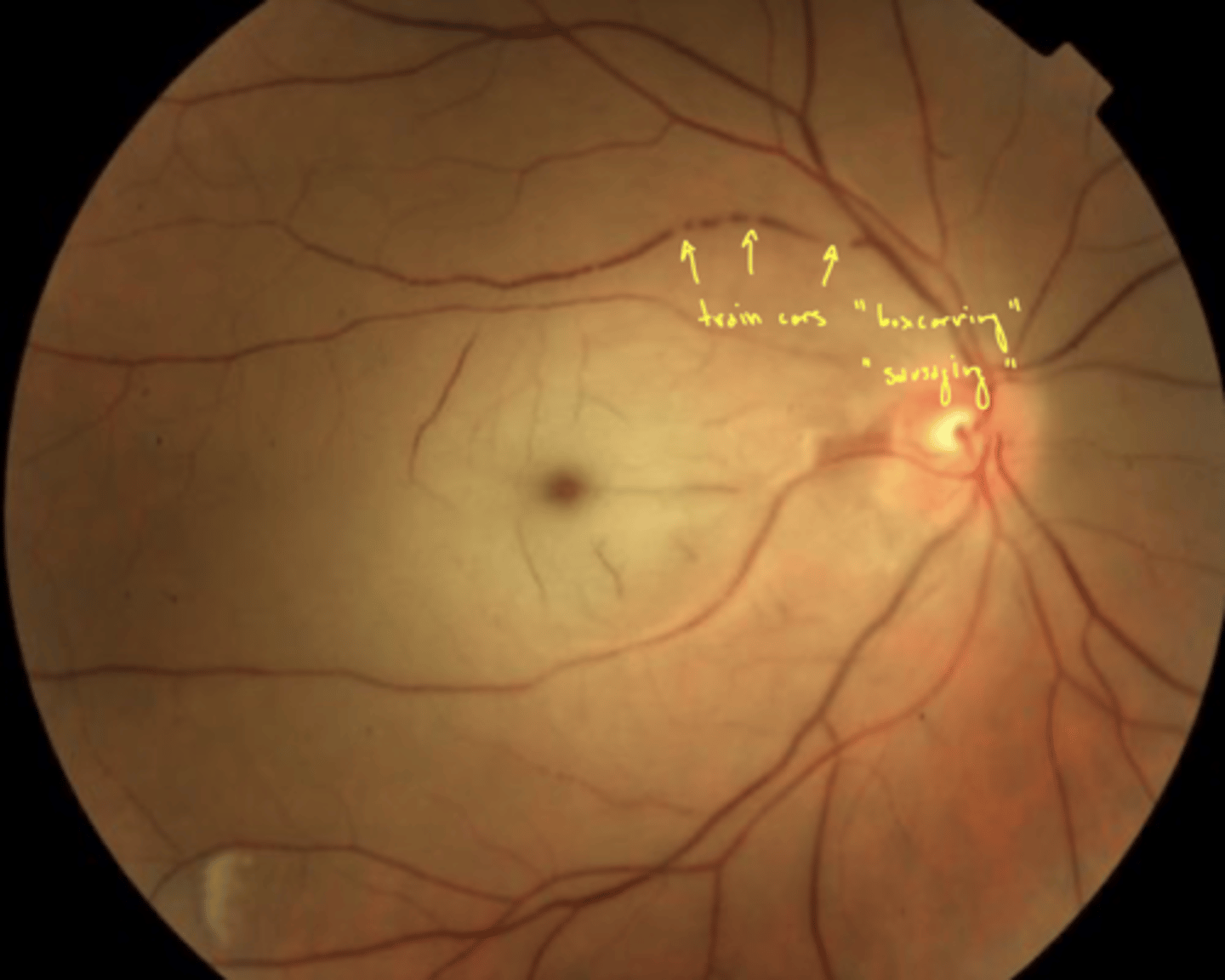
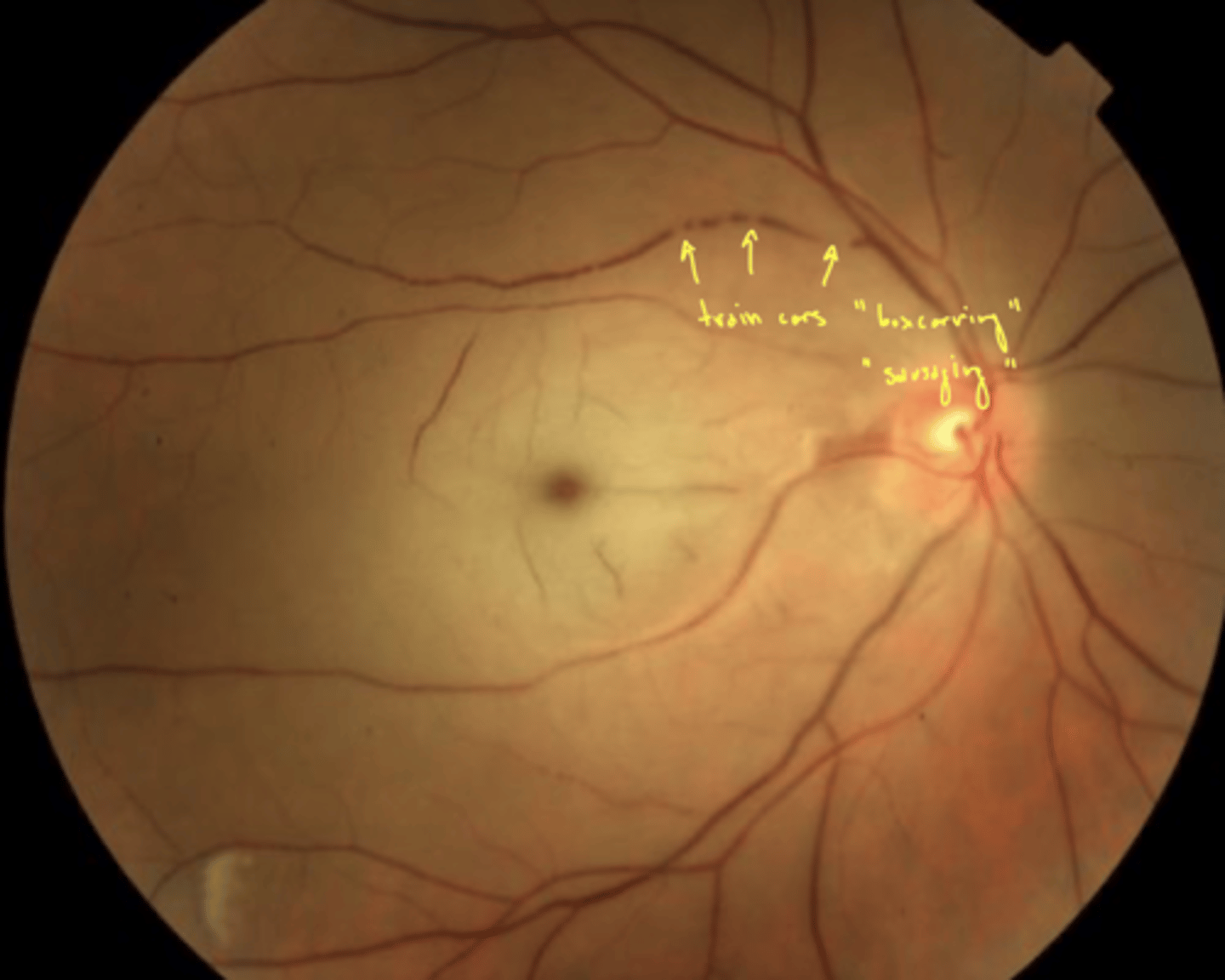
what happens to the retinal vasculature and retinal tissue during a CRAO?
1. retinal arteries narrow and retinal tissue is hazy
2. retinal tissue turns white and fovea appear as cherry red spot
3. veins appear boxcarring
4. glial tissue replaces infarcted retina
what causes the fovea to appear as a cherry red spot?
retinal tissue is white → no blood supply
fovea is still red because blood supply from choroid unaffected
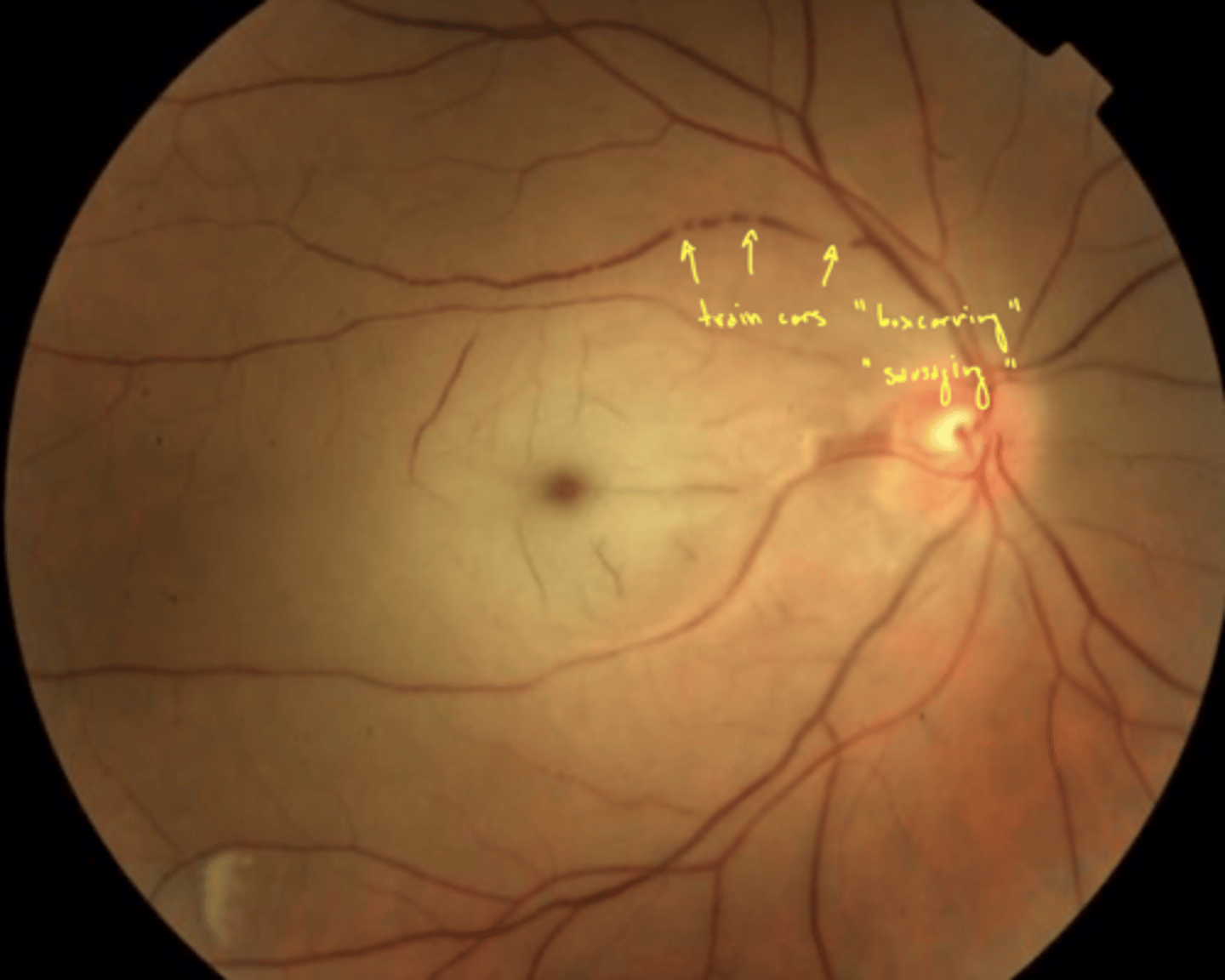
what is boxcarring?
veins become distended (swollen due to pressure) → segmented appearance (sausage links)
arrow in image
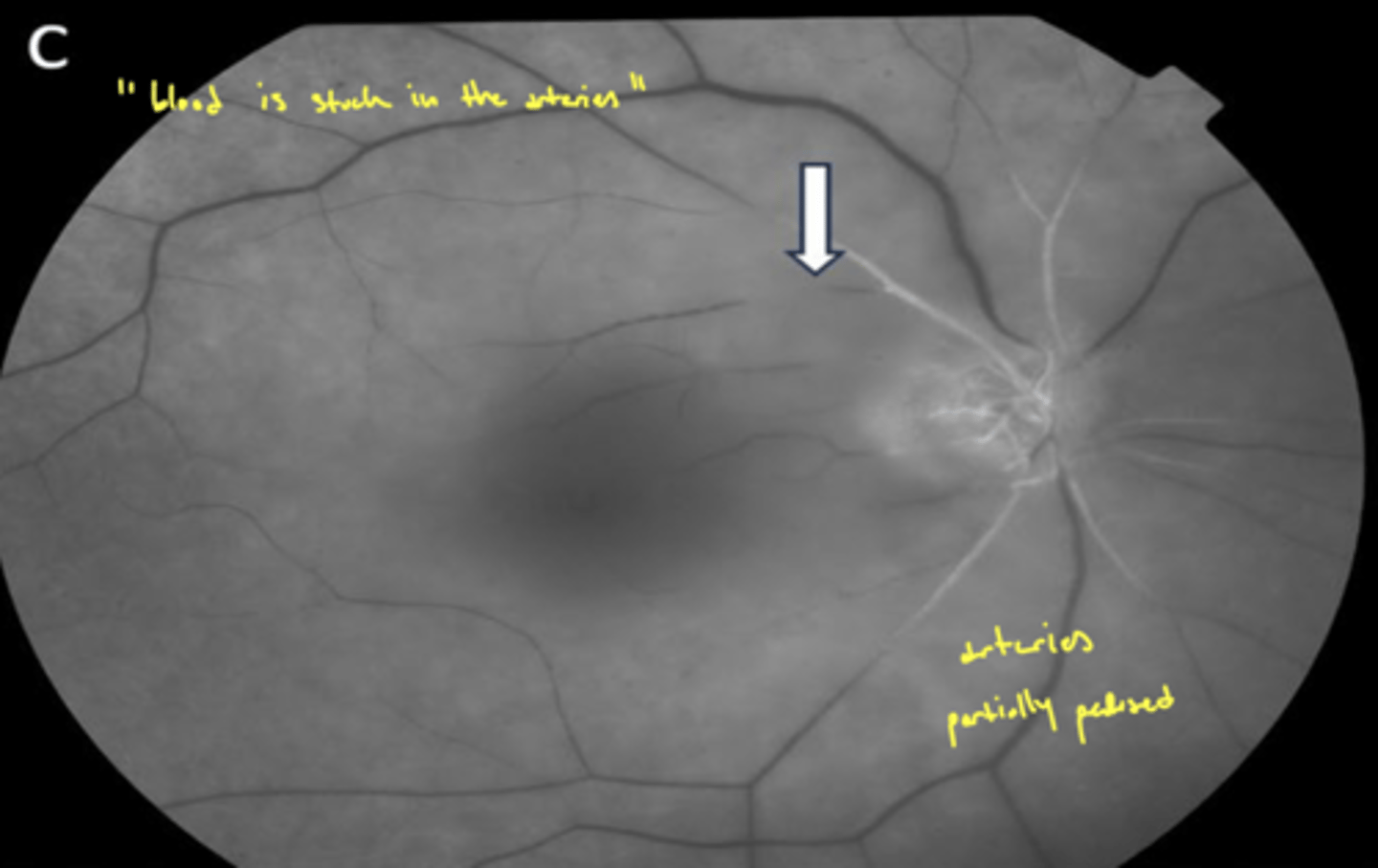
What will a CRAO look like on FANG?
"blood is stuck in arteries"
What do you do in office while waiting for EMTs to arrive for a CRAO/BRAO?
1. give acetazolamide (oral) or 2 gt of timoptic (timolol) to decrease IOP
2. digital massage - unlodge embolus
Fogt "none of this crap works"
what are the managements of a retinal artery occlusion?
1. call 911 → occlusion reversible within 1-2 hrs
2. decrease IOP using meds and digital massage sometimes by removal of AH (paracentesis)
3. inhale carbogen to dilate vessels
4. hyperbaric oxygen
5. make sure patient gets systemic vascular workup
Fogt "none of this crap works"
What is the pathophysiology of hypertension retinopathy (stages)?
first stage = generalized arteriolar narrowing (autoregulation)
second stage = thickening (lipids) of blood vessels walls - increases arteriolar light reflex
third stage = exudative stage (blood:retinal barrier breaks down)
What is hypertensive retinopathy the number one cause of (2)
1. venous occlusion
2. macroaneurysm
What blood pressure is considered hypertensive crisis?
>180 / >110
if either systolic or diastolic were to be higher, regardless of the other value → worse stage

What is the management for hypertension and hypertensive retinopathy?
done in this order
1. control through diet (low saturated and low trans fat), exercise
2. then medication
How can hypertension and hypertensive retinopathy be controlled through diet? What are the recommendation?
1. low saturated fats
2. salt restriction
3. alcohol in moderation
4. increase potassium intake
What is the blood pressure goal for patients ≥60 years old with no diabetes or kidney disease?
<150/90
What is the blood pressure goal for patients ≥60 years old with diabetes or kidney disease?
<140/90
What is the blood pressure goal for patients <60 years old?
<140/90
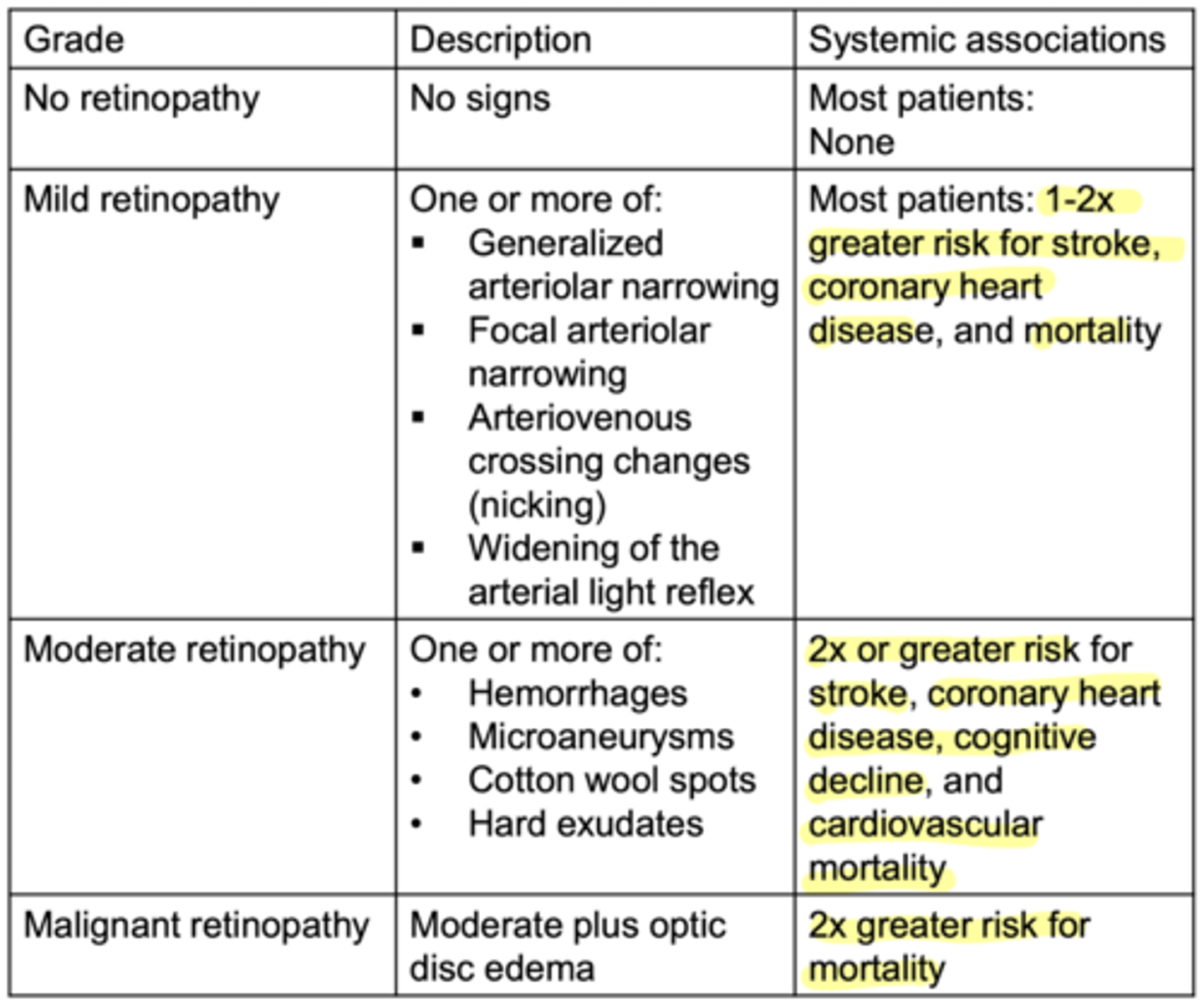
what are changes to the retina caused by mild hypertension (mild hypertensive retinopathy)?
1. narrowing of arteries
2. A/V crossing changes
3. artery sheath changes (widening of light reflex, nicking, or arteriolar narrowing)
4. tortuosity
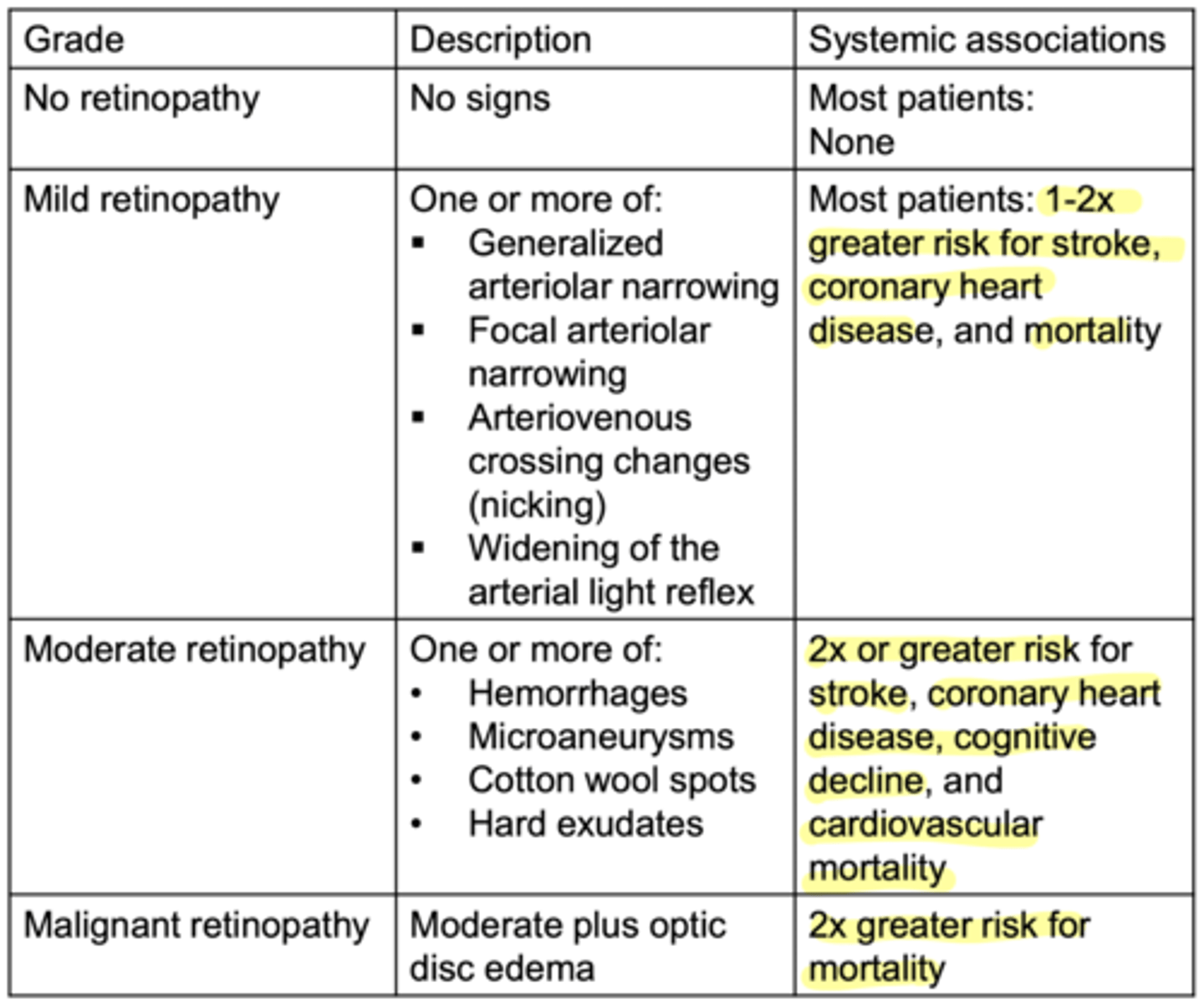
What are the changes to the retina caused by moderate hypertensive retinopathy?
everything from mild
1. vascular leakage
2. vascular occlusion
3. microaneurysms (like diabetes)
What are the changes to the retina cause by malignant hypertensive retinopathy?
everything from mild/moderate
1. optic nerve head edema
What should the normal AV ratio be?
artery should be 2/3 diameter of vein
exam will ask you to differentiate between artery and vein, arteries are usually smaller
What would be an abnormal AV ratio?
<2/3 narrowing from potentially autoregulatory changes - if pressure is too high, vessel constricts to increase resistance and reduce flow
What is a normal arteriolar light reflex?
1/3
What is an abnormal arteriolar light reflex?
>1/3 caused by thickening and material deposition in blood vessel wall
what are advanced changes to retina caused by chronic HTN?
1. CWS
2. flame hemes
3. intraretinal macular + ONH edema
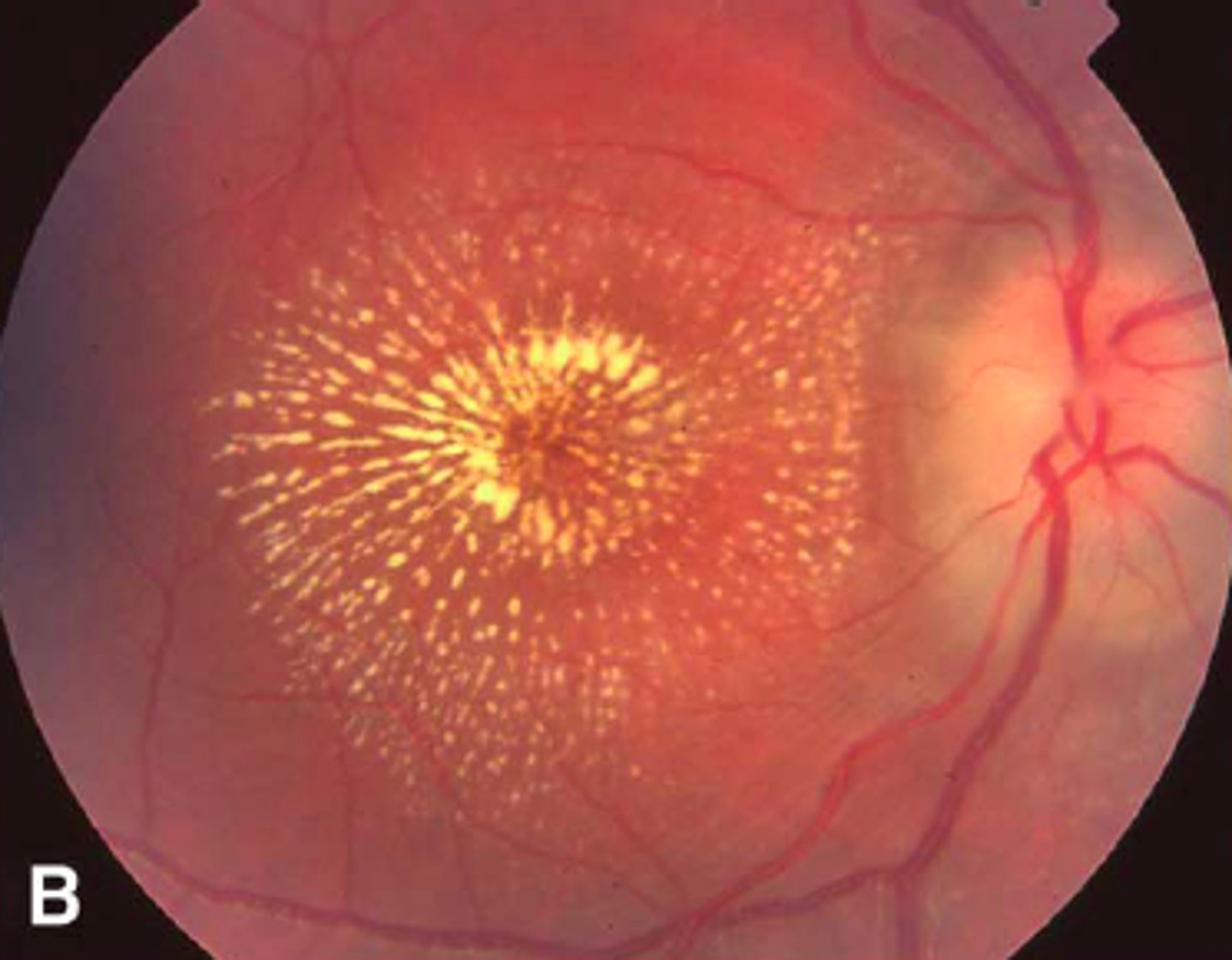
4. macular star hard exudates
what is macular star hard exudates?
circle of hard exudates around macula → indicates macular edema
image - bit extreme of an example
How does controlling blood pressure change hypertensive retinopathy?
regress moderate and malignant changes → mild will stay (but will progress much slower)
What is the management for hypertensive retinopathy (overall)?
1. control blood pressure (exercise, diet, meds)
2. refer if macular or ONH edema
What is the management for mild hypertensive retinopathy without edema/neovascularization?
1. check BP in office
2. refer to PCP within 2w
3. diet and exercise
remember metabolic disorders (like DM) can cause faster progression
What is the management for moderate hypertensive retinopathy without edema/neovascularization?
same as mild (assuming no macular edema)
1. check BP in office
2. refer to PCP within 2w
3. diet and exercise
remember metabolic disorders (like DM) can cause faster progression
What is the management for severe/malignant hypertensive retinopathy without edema/neovascularization?
send to emergency room for systemic health
Do any of the signs of hypertensive retinopathy regress after treatment?
everything (moderate/malignant) but mild signs
what causes mild hypertensive retinopathy to progress from mild to moderate?
chronic problems
what does moderate hypertensive retinopathy have a strong association with?
1. stroke
2. coronary heart disease
3. death
what does malignant hypertensive retinopathy have a strong association with?
death
What is NOT considered arteriosclerotic retinopathy?
ANY vascular leakage or occlusion → d/t to involution or age-related
what does this mean?
basically age related occlusion or leakage never rise to the arteriosclerotic retinopathy grading
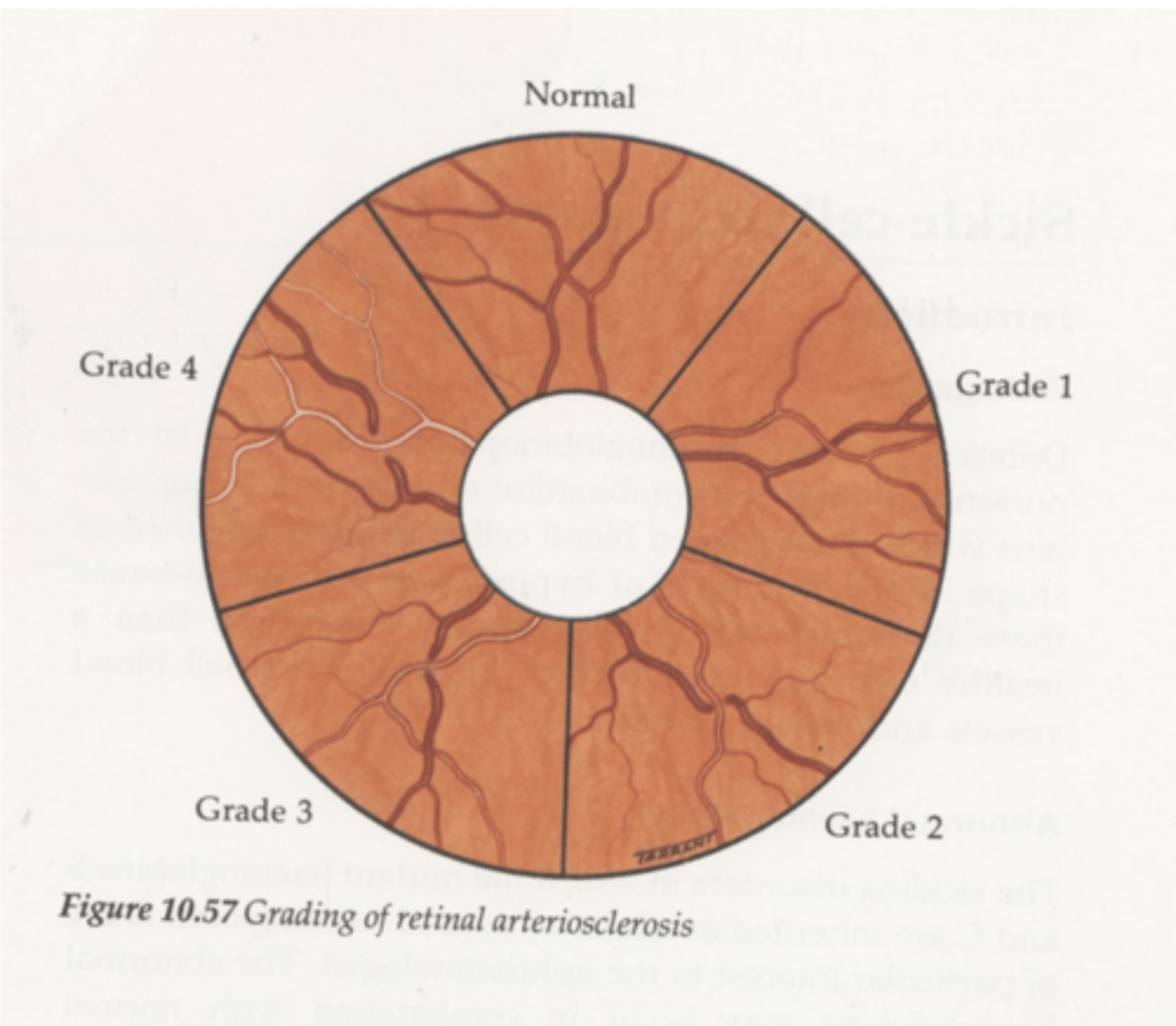
What does grade 1 arteriosclerotic retinopathy look like?
narrowing of arteries
widening of light reflex d/t thickening of walls
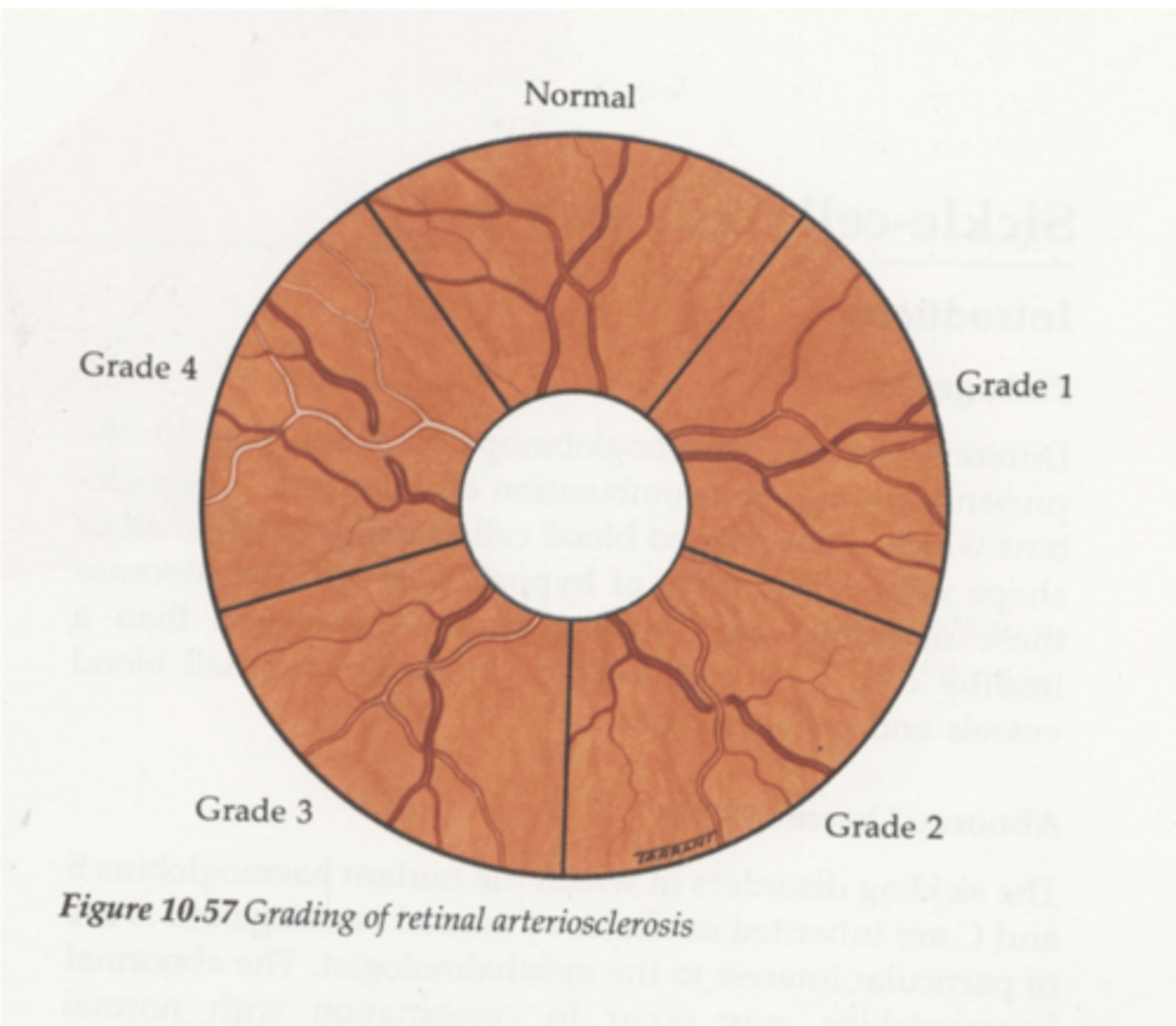
What does grade 2 arteriosclerotic retinopathy look like?
crossing changes (nicking + banking)
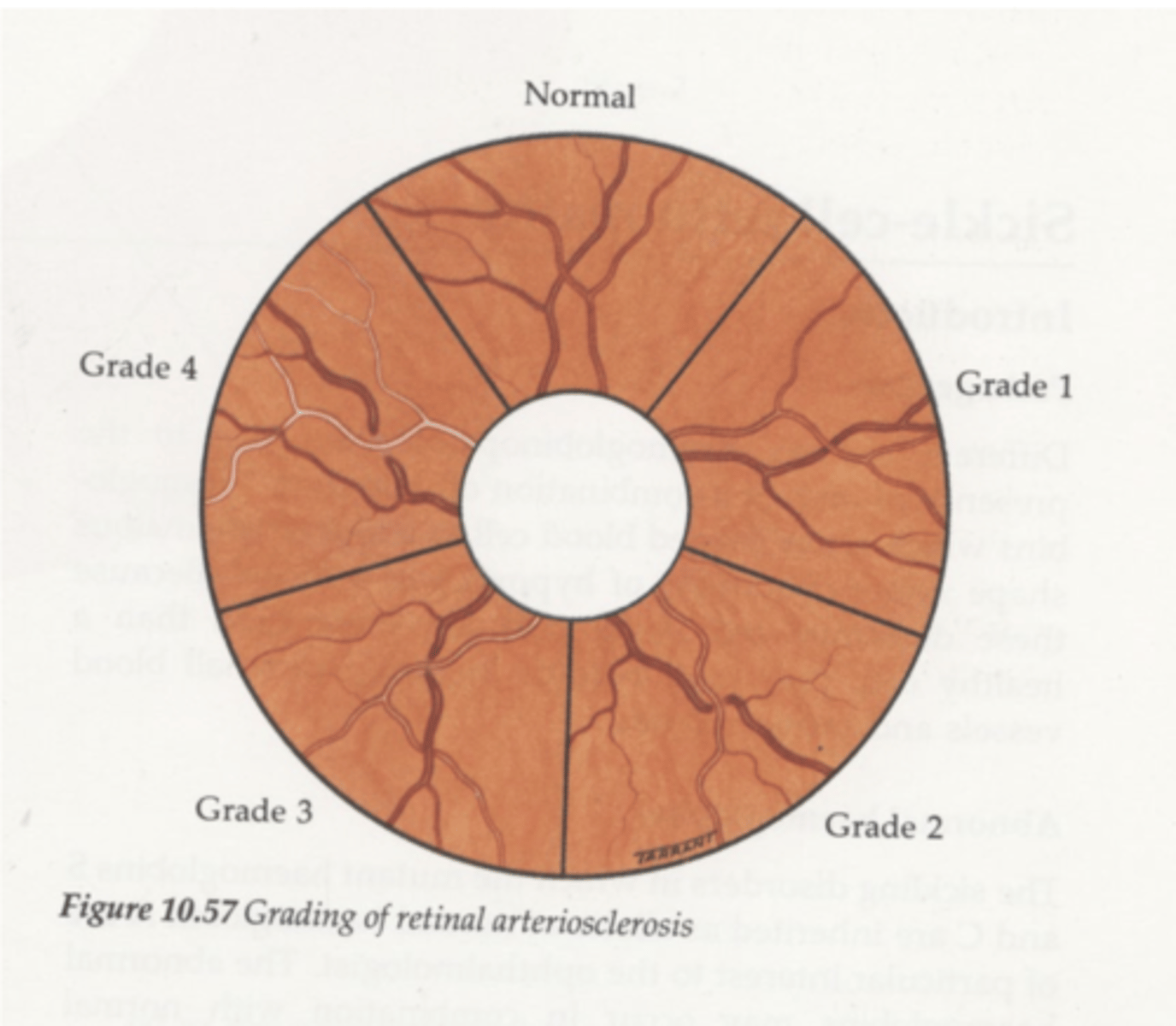
What does grade 3 arteriosclerotic retinopathy look like?
1. more extensive crossing changes
2. copper wiring
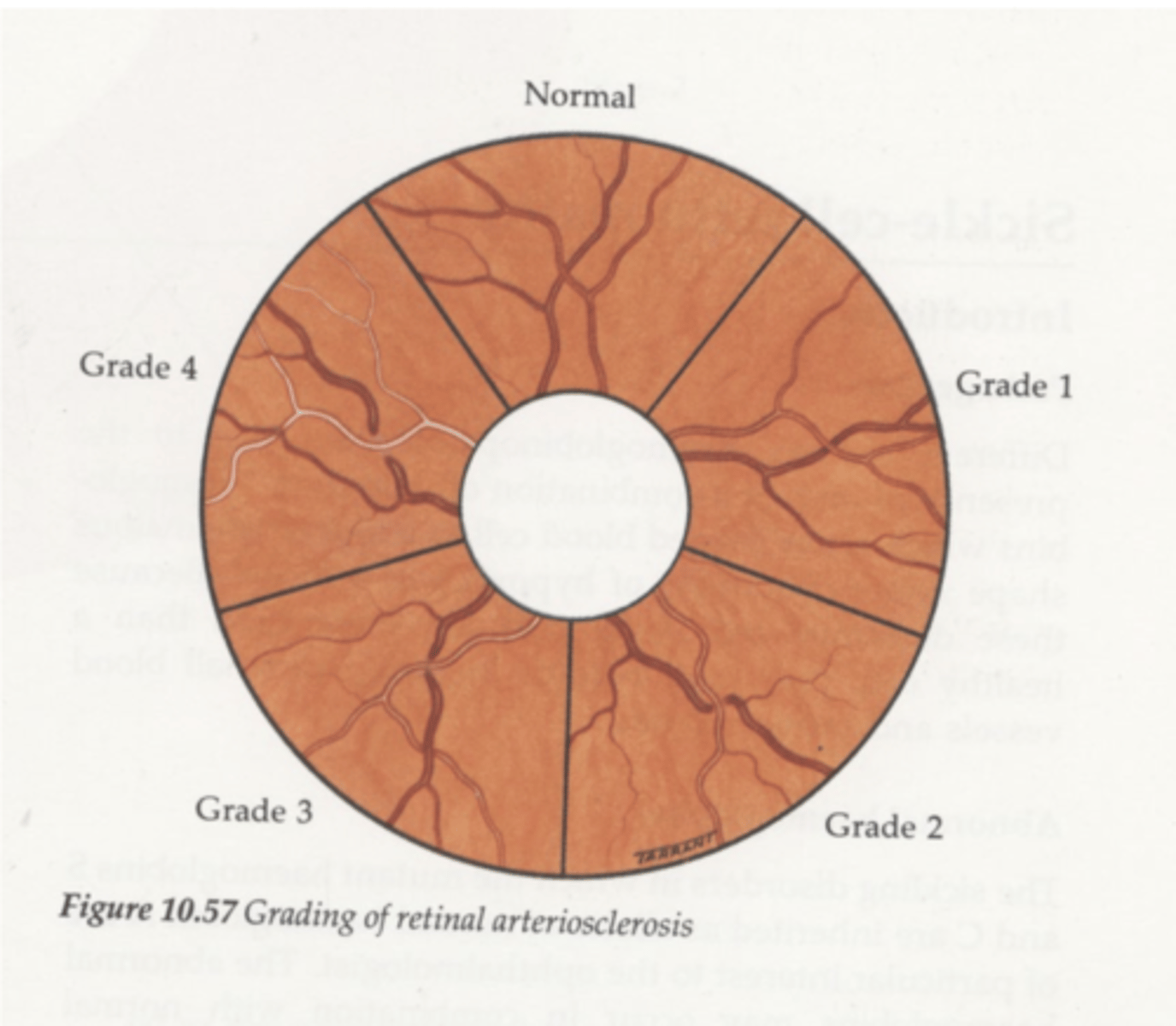
What does grade 4 arteriosclerotic retinopathy look like?
silver wiring d/t cholesterol, fibrin and calcium deposition