Module 11 - Single Ventricle
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
Define a single ventricle.
Only one ventricle is of adequate size due to hypoplasia of AV valve or ventricle.
List some conditions that a single ventricle repair is required.
Tricuspid atresia (blocked TV)
Hypoplastic left heart syndrome
Double inlet LV (L-loop with double inlet)
Severe Ebstein’s
Unbalanced AVSD
Describe Fontan flow.
Passive flow to the lungs, single ventricle systemically pumps.
Describe the classic Fontan procedure.
Anastomose RA appendage to PA
Close connection from RA-RV and IAS
Describe hemodynamic consequences of the classic Fontan repair.
RA dilation
Blood stasis
Arrhythmias
Describe stage 1 of the modified Fontan repair. When is this repair done and why?
Stage 1 (BDG shunt) at 4-6 months. Done after PA pressure drops.
Anastomosis of SVC to RPA
Close MPA
Remove IAS (ASD)
IVC still connected to RA
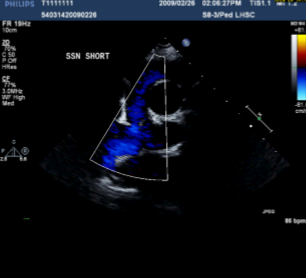
Describe the findings of this image.
Anastomosis between SVC and RPA → BDG shunt
Define the BDG shunt.
Bidirectional Glenn shunt. Connects the SVC to the RPA.
Describe stage 2 of the modified Fontan repair. When is this repair done and why?
Stage 2 at 2 years old.
Fenestration between conduit and RA
Connection between IVC and pulmonary arteries
Close fenestration via catheter
Explain why a fenestration is necessary between a conduit and RA.
If pressure in the pulmonary arteries increases during surgery or before healing, the fenestration allows a R-L shunt. This maintains CO until it can be repaired.
How is an intracardiac vs extracardiac conduit baffles be differentiated on echo?
Difficult to differentiate.
Both are seen posterior to the atria.
Both have low velocity biphasic forward flow.
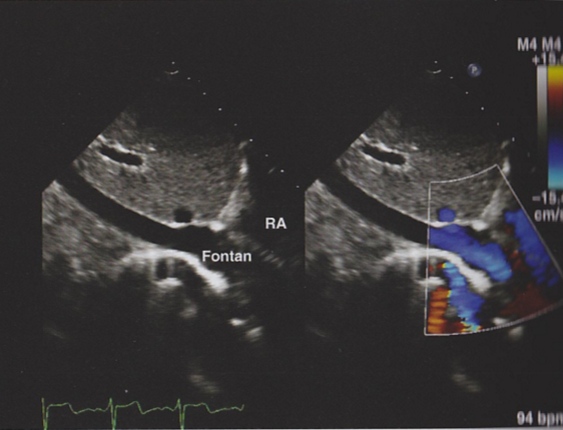
Describe the findings in this image.
Extracardiac conduit seen traveling behind the RA. Good forward flow.
A newborn patient is showing signs of cyanosis. Upon echo, pulmonary atresia with an intact IVS is found. What is the recommended treatment?
Cannot wait 4-6 months for BDG shunt.
Ductal dependent lesion but cant keep on prostaglandins that long.
BT shunt.
Describe a BT shunt.
RSA to RPA shunt to provide BF to lungs
Remove the BT shunt when Glenn performed at 4-6 months
What is the expected velocity through a T shunt?
High velocity because there is a large PG (systemic-pulmonary).
Describe the Norwood procedure. When is this repair done and why.
Norwood procedure at newborn period. Done for hypoplastic left heart syndrome.
Stage 1
MPA disconnected from branch PAs
Combine Ao and MPA to create neo-Ao
BT shunt to supply lungs
Stage 2 - Glenn repair at 4-6 months
Stage 3 - Fontan completion at 2 years
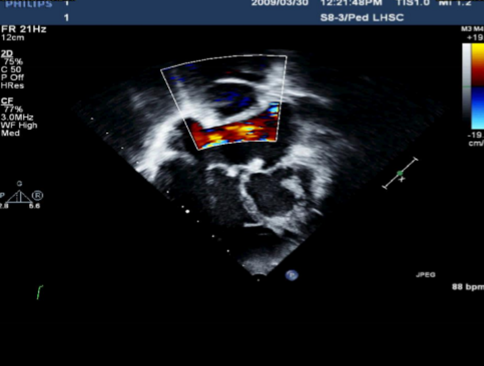
Describe the findings of this image.
No fenestration between extracardiac conduit and atrias.
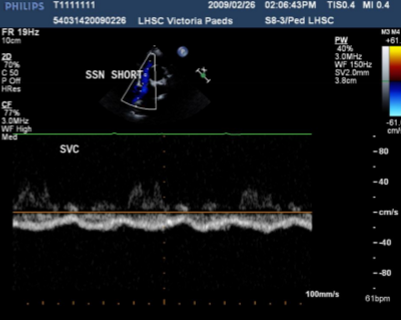
Describe the findings of this image.
Biphasic low velocity flow in a Glenn shunt.
Connection between RPA and SVC.