Cardiology
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|

29 Terms
What is the cardiac complication of Hunter-Hurler Syndrome?
valvular insufficiency, heart failure, hypertension
What is the cardiac complication of Duschene's?
Cardiomyopathy, heart failure
What is the cardiac complication of pompe disease?
Short PR, cardiomegaly, heart failure, arrhythmias
What is the cardiac complication of Kawasaki disease?
coronary artery anurysm, myocardial infarction, myocarditis
What is the cardiac complication of Marfan syndrome?
Aortic root dilatation, mitral and aortic insuffieciency, aortic dissection
What is the cardiac complication of JRA?
Pericarditis
What is the cardiac complication of SLE?
Pericarditis, Libman-Sacks endocarditis, congenital heart block
What is the cardiac complication of lyme disease?
arrhythmias, myocarditis, heart failure
What is the cardiac complication of Grave's disease?
tachycardia, arrhythmias, heart failrue
What is the cardiac complication of tuberous sclerosis?
cardiac rhabdomyoma
What is the cardiac complication of neurofibromatosis?
pulmonic stenosis, coarctation of the aorta
What is the cardiac complication of T21?
AVSD
What is the cardiac complication of Noonan syndrome?
Pulmonary stenosis
What is the cardiac complication of Turner's syndrome?
Bicuspid aortic valve, aortic arch abnomalities incluidng caorctation of aorta
What is the cardiac complication of 22q11 deletion?
Conotruncal abnormalities including TOF, PDA, interrupted aortic arch (type B)
What is the heart murmur associated with an ASD?
Systolic murmur, usually softer I or II, best heard at LUSB, with fixed S2 split. May be assoicated with heaves (RV hypertrophy)
- There could be no murmur initially, because the murmur is actually from pulmonary overflow
What is the murmur associated with pulmonary stenosis?
LUSB, louder/harsher, can radiate to the back, wide split S2 with quieter P2 component of the S2 sound
List qualities and common types of innocent murmurs?
Soft, vibratory/musical, no other symptoms, normal split S2, systolilc, often positional
eg.
- Still's murmur: age 2-7, systolic, louder when lying down, quieter with valsalva
- Venous hum: age 2-7, systolic continuous murmur at sternocleido junction R>L, quieter when turning head away and chin up, louder when sitting up
- Peripheral pulmonary stenosis: 0-6 months, blowing quality, radiated to the lungs and axillae, not positional
**If you suspect innocent murmur in a baby at DC exam, can just follow
What are the criteira for cardiology referral for a murmur?
- any murmur at birth or day 1 of life
- Cardiac symptoms
- Marfan features
- FHx of sudden cardiac death, or congenital heart disease in a first degree family member
- suspected genetic condition eg. T21
- request from family with good reason
What does a VSD murmur sound like?
Perimemberanous VSD will give you A holosystolic murmur best heard at the LLSB (tricuspid valve position) (flow murmurs are also best heard in this position)
Muscular VSD will give you early systolic murmur because the muscle contracts and closes the hole as systole continues
VSD murmurs are harsher sounding than innocent vibratory murmurs. They tend to show up around day 2 of life on the discharge exam. You tend to present with CHF symptoms around 4-6 weeks of life as pulm pressures drop and L-->R shunting increases.
What are the criteira for SBE prophylaxis?
- unrepaired cyanotic heart lesions
- partially repaired heart lesions with residual flow around prosthetic materials or partially repaired cyanotic lesions including palliative shunts
- Any repair using prosthetic materials for 6 months after surgery
- any valve replacement (bio prosthetic or mechanical)
- Any previous IE
- Heart transplant pts who develop valvulopathies
for what procedures should you consider SBE prophylaxis?
Anything involving manipulation of gingiva
Airway surgeries including T&A or bronch with biopsies
If you are going through infected skin
What is the JONES criteria?
ARF can present with several different clinical findings within one to five weeks (usually two to three weeks) of a group A streptococcal (GAS) infection
However, in low resource countries, people can present late with symptoms of established rheumatic heart disease due to lack of access to care
For initial presentation you need 1 major + 2 minor OR 2 major
For recurrent presentations you need 2 major OR 1 major + 2 minor OR 3 minor
MAJOR CRITERIA
- polyarthritis
- carditis (clinical or subclinical)
- Erythemia marginatum
- chorea
- subcutanous nodules
MINOR CRITERIA
- polyarthralgia
- fever over 38.5
- ESR > 60 or CRP >30
- prolonged PR interval for age (unless already meeting carditis criteria)
What is the prophylaxis for rheumatic fever?
PEN G 0.6-1.2 million units Q3-4 weeks is used for secondary prevention
- If carditis and residual heart defect - for 10 years or until age 40 whichever is longer
- If carditis, no residual heart disease - for 10 years or until age 21 (whichever longer)
- if no carditis, 5 years or age 21
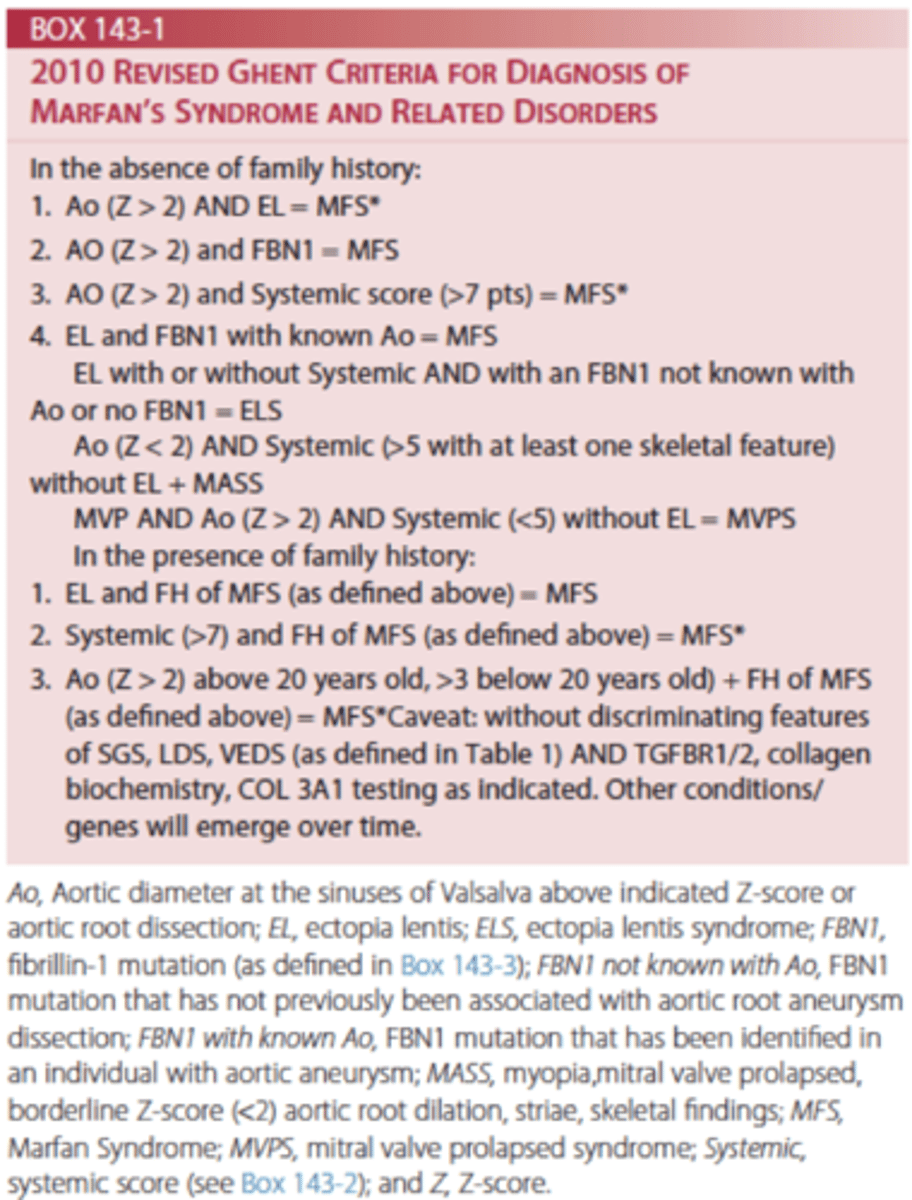
How do you diagnose Marfan's?
Modieifed Ghent criteira
Hall mark features include aortic root dilatation, ectopia lentis
Systemic features (part of the scoring)
- wrist sign, thumb sign (arachtodactlyl)
- pectus cranatum
- hindfoot deformity
- pneumothorax
- protrusio ecitabuli (hip Xray)
- increased wingspan to heigh >1.05
- scoliosis or kyphosis
- reduced elblow extension
- skin striae
- myopia over 3
- mitral valve prolapse
- facial features (high arch, teeth crowding, downslanting palpebral fissures, reterognathia, enophthalmus, dolicocephaly)
- dural ectasia (imaging)
What is mainstay of unrepaired VSD management as a pediatrician?
1) Monitoring for signs of heart failure including Growth failure, Dyspnea/work of breathing
2) Monitor for other complications
Depending on the location of the VSD may be at risk of aortic valve prolapse
3) Management of heart failure if present:
- Diuretics (lasix +/- spiro)
- Support growth eg. Hypercaloric feeds
- Vaccinations, RSV prophylaxis if hemodynamically significant
4) Criteria for surgical repair (if needed usually around 6 months of age)
- Clinical heart failure
- Aortic valve prolapse (with the pressure across the VSD the leaflet can get sucked into the VSD causing prolapse)
What is the management of tet spells?
Presents as cyanosis (look for central not peripheral) maybe pre/syncope
Treatment
- Get them settled
- Position to increase SVR with legs to chest it also increases return to heart
- Bolus fluids
- Morphine - reduce pain/anxiety
- Beta blockers eg. Propranolol to decrease HR which will increase SV
- Phenylephrine or epinephrine (to increase SVR)
What are the cut offs for CCHD screen?
Pass = >95% and <3% pre/post difference
Fail = <90%
Yellow zone/borderline = 90-94% or >3% pre/post difference, you repeat x2 q1h but if persistently borderline then it is a fail (so if you get borderline 3 times then it is a fail)
What do you do with a failed CCHD screen?
- contact physician (us!)
- consider 4 limb BP, ECG, CXR
- If suspected cardiac pathology consider cardiology consult