Exam 2 - Adult Psychopathology
1/159
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
160 Terms
Suicide attempts and suicidal thoughts are relatively common among individuals living with
Anxiety disorders, depression, PTSD
Who is more likely to die by suicide: men or women?
Men
Which of the following social factors are key components of Joiner’s interpersonal theory of suicide?
Perceived burdensomeness
What is one key treatment goal that is focused on heavily during DBT for suicidal individuals?
Developing skills to regulate and tolerate emotions
Suicide definition
intentional, direct, conscious taking of one’s own life
Up to what percentage of people who contemplate suicide have a psychological diagnosis?
90%
Suicidal ideation is an official symptom of what disorder classified in the DSM?
Major Depressive Disorder (MDD)
Components of suicidality (3)
Suicidal thoughts/ideation, suicidal intent (desire), suicidal behavior (plan/attempt)
Spectrum of Suicidal Ideation (lower risk → higher risk)
1) Occasional thoughts about mortality/death w/ no ideation
2) Passive Suicidal Ideation (thoughts)
3) Active (Starting to think about a method/form plan)
4) Clear plan articulated to act
NSSI
Non-suicidal self-injury; direct/deliberate destruction of body tissues in the absence of any intent to die (e.g. cutting/burning)
Prevalence of NSSI? What group is prevalence highest in?
17-23% / Adolescents, especially female
Epidemiology of Suicide (U.S.)
Over 1.4 million adults make an attempt each year; rates have been increasing among all ages/gender/ethnic groups
What part of model explains why not every person attempts?
Gap between desire and behavior; capacity that builds pain tolerance is where we see difference
Globally, more than ___ people die to suicide every year
720,000
What percentage of suicides occur in low or middle income countries?
77%
Suicide Risk Factors (6)
Previous intent or attempt, substance use, depression, hopelessness, social isolation, easy access to lethal methods
Suicide Protective Factors (5)
Clear reasons for living, social support, strong emotion regulation and problem-solving skills, openness and access to treatment for mental health, restricted access to lethal means of suicide
Suicide rates for young people are at their highest since the 2000s. Why? (5)
Social media, substance use, bullying, difficulty accessing treatment, historical controversies around antidepressants for teens (concern of increase in thinking)
Suicide rates for older adult men are very high. Why? (Factors of increased risk)
Bereavement, declining physical health, social isolation, financial difficulties
Suicide Multipath Model: Psychological Domain
Joiner’s interpersonal model, focused on social connections
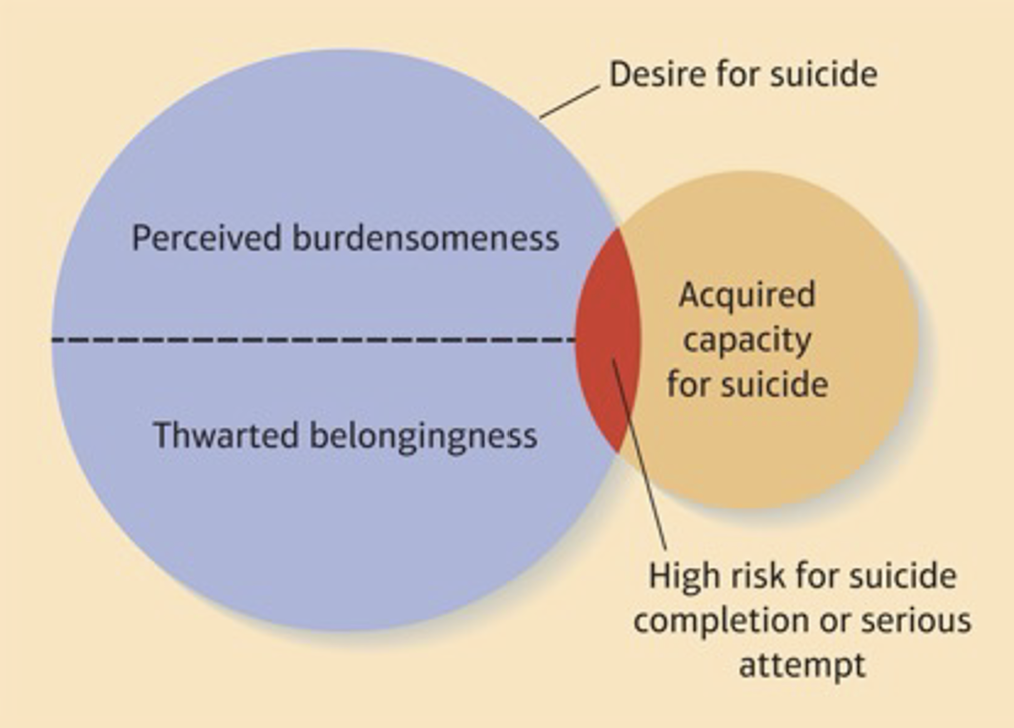
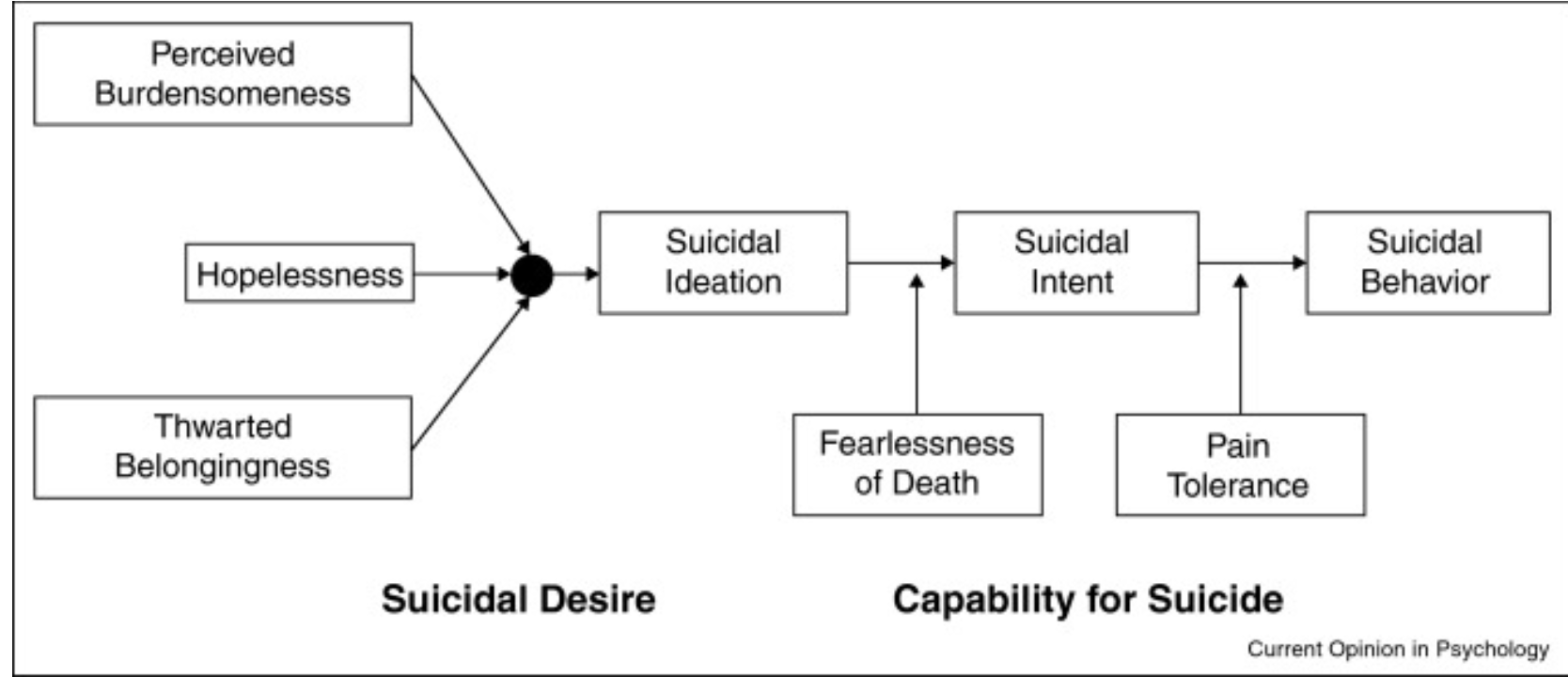
Joiner’s interpersonal model (3 components)
Perceived Burdensomeness: Feeling that others would be better without you, contributes to suicidal ideation & intent
Thwarted Belonginess: lack of connection with others, feeling the need to belong is not met
Acquired Capacity: Habituation to pain, fearlessness about death, prior suicidal behavior, contributes to attempt/death
Phrase someone experiencing perceived burdensomeness might say:
“People in my life would be better off if I was gone”
Phrase someone experiencing thwarted belongingness might say
“These days I feel disconnected from other people”
What component(s) of Joiner’s interpersonal model contribute to suicidal ideation & intent?
Perceived burdensomeness and thwarted belongingness
What component(s) of Joiner’s interpersonal model contribute to suicidal attempt or death?
Acquire capacity
Suicide Multipath Model: Social (Protective & Risk)
Protective: stable marriage/relationship makes suicide less likely; for women - having children
Risk: Divorced/separated/widowed; death of spouse associated with 50% higher suicide rate in men
Suicide: Leading cause
Firearms
Men make up 79% of all U.S. suicides. Why?
Means men choose to use makes them more likely to die (lethal)
Who experiences more suicidal ideation: men or women?
Women
Safety Planning / What is it? What level of risk is this effective for?
A brief, collaborative intervention to reduce suicide risk, builds a personalized step-by-step plan; moderate level of risk
Components of suicide risk safety planning (5)
(1) Recognize warning signs (2) Identify coping strategies (3) Identify supportive social contacts (4) Professional resources (5) Means safety/reducing access to lethal means
An individual with high risk of suicide will be addressed with…?
Hospitalization
High Risk of Suicide: Hospitalization / What does it involve?
Typically involves referral to a higher level of care (voluntary or involuntary); stabilize/ensure immediate safety, initiate treatment
Post-hospital discharge of a patient is a high-risk time in terms of suicide. Why?
Hospitalization does not remove risk factors
What type of therapy can be used to manage ongoing suicide risk?
Cognitive Behavioral Therapy (CBT)
CBT for managing ongoing suicide risk
Targeting underlying processes, often used after recent attempt or high-risk event
Components of CBT for managing ongoing suicide risk
Safety planning, coping and problem-solving skills, cognitive restructuring
CBT Key: Suicidal thoughts are ____ through ____ & ____ change
modifiable; cognitive; behavioral
Diagnosable eating disorders are not solely about body weight/size/shape but also…
Persistent symptoms, interfering with daily functioning & causing distress
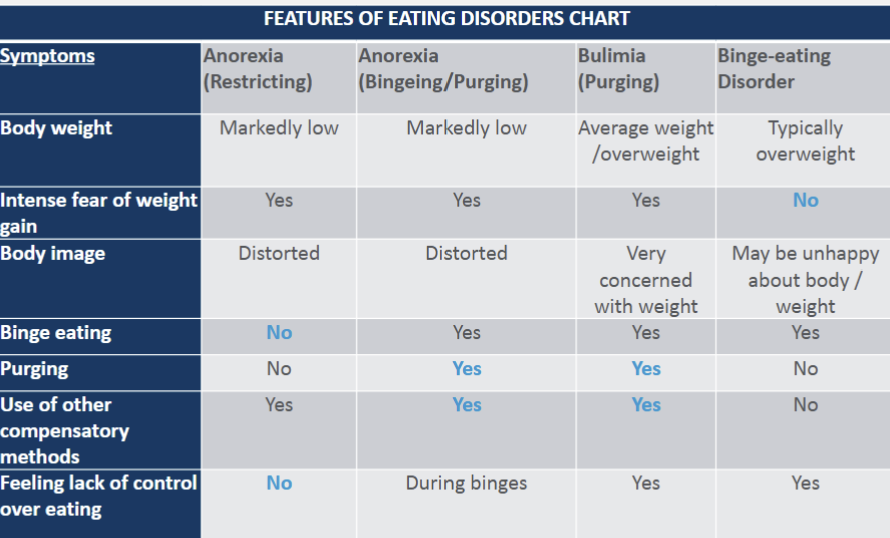
Anorexia nervosa is characterized by…(3)
Caloric restriction + low body weight
Intense fear of weight gain
Disturbance in body image (continue to insist one is overweight even when clearly underweight)
Anorexia’s two subtypes (+ description of each)
1) Restricting: weight loss through extreme dieting or exercising
2) Binge-eating/purging: self-induced vomiting, laxatives, or diuretics
Course of Anorexia Nervosa
Course is highly variable. Some recovery after one episode, others fluctuate between weight gain and relapse, others have chronic/deteriorating course.
Outcome of Nervosa Anorexia
Onset in adolescence is associated with more positive outcomes; high mortality rate in anorexia
Physical complications of Anorexia Nervosa
Irregular heart rate, low blood pressure, heart damage
Characteristics of Bulimia (3)
Recurrent episodes of binge eating followed by compensatory behaviors, self-evaluation strongly influenced by weight or body shape, typically of average weight
Compensatory behaviors seen following binge episode in Bulimia
Purging, excessive exercising, fasting
Cycle of Bulimia

Comparison of onset of Bulimia and Anorexia Nervosa
Bulimia begins in late adolescence or early adulthood; compared to early adolescence for anorexia
Is prognosis (course over time) more positive or negative in Bulimia compared to anorexia?
More positive
Binge-eating Disorder characteristics
Individual engages in binge-eating episodes (1/week for at least three months), experiences distress, but does not use compensatory behaviors
Characteristics of a binge episode (5)
Eating more rapidly than normal, uncomfortable feelings of fullness, eating large amounts of food even when not hungry, eating alone due to embarrassment, feeling depressed or guilt after bingeing
People with eating disorders often later develop ___
Other eating disorders
Two common diagnostic crossovers in eating disorders
Transition between 2 subtypes of anorexia, shift from anorexia to bulimia
Rare diagnostic crossover in eating disorders
Transition from bulimia to anorexia
Psychological Dimension of Eating Disorders
High perfectionism personality type (inflexibly high standards, negative self-evaluation after mistakes), distorted thinking related to weight/shape, difficulty with regulating emotions (anxiety, guilt, shame, sadness)
What personality type is commonly seen in anorexia and bulimia?
High perfectionism
Social Dimension of Eating Disorders
Families and peers often reinforce social messages about weight/shape (“fat talk”), appearance standards strongly influenced by social media (thin ideal internalized)
Among what group are EDs increasing in?
Men
Non-Western countries show increases in EDs after exposed to…?
Western cultural ideals
Biological Dimension of Eating Disorders
Genetics: 40-60% increased risk in first-degree relatives
Neurotransmitters: dysregulation in serotonin and dopamine
Brain circuitry: atypical activity in reward pathways (striatum) and cognitive control (prefrontal cortex)
Hormones: disruptions in leptin & ghrelin (fullness signal) and HPA axis
Neurotransmitters that are dysregulated in eating disorders + their role
Serotonin - mood and appetite, Dopamine - reward
Psychological Interventions for EDs
CBT and Family based interventions
How does CBT address EDs?
Establishing regular eating patterns, address distorted thinking, identify triggers, interrupt behaviors maintaining disordered eating cycles (especially bingeing / compensatory behaviors)
Family based interventions for EDs is especially effective for what group?
Adolescents
Medical Interventions for EDs
Weight restoration (gradual increase) and SSRIs
Why are SSRIs less effective for anorexia compared to bulimia and binge eating disorder?
Less effective when patients are low body weight
Describe the mesocorticolimbic pathway and its role in addiction
Like other rewards, substance activates this pathway. Dopamine is released with pleasure as the response. Chronic usage causes alterations in pathway
DSM-5 Criteria for Substance-Use Disorder: How many symptoms and for how long must these symptoms be present?
Two or more symptoms must be present for > 12 months
Broad symptom themes in Substance-Use Disorder (DSM-5)
Impaired control, social impairment, risky use, pharmacology
Substance Use / Impaired Control
Substance taken in larger amounts or longer than intended, unsuccessful efforts to cut down, time spent obtaining/using/recovering, craving or strong desire to use
“I’ll just have one drink” → ends up drinking all night. This is an example of what broad symptom in substance-use disorders?
Impaired Control
Substance-Use Disorder / Social Impairment
Failure to fulfill major obligations (school, work, home), continued use despite social or interpersonal problems, activities given up or reduced because of use
Skipping class or losing friends because of continued substance use is an example of what broad symptom category?
Social impairment
Substance-Use Disorders / Risky Use
Use in physically dangerous situations, continued use despite knowledge of physical or psychological harm
Drinking and driving despite worsening depression is an example of what broad symptom category of Substance-Use Disorders?
Risky Use
Substance-Use Disorders / Pharmacology
Tolerance ( need more substance for same effect OR diminished effect ), withdrawal ( characteristics symptoms emerge after period of non-use OR using substance to relieve withdrawal )
Substance-Use / Pharmacology Clarification
These can occur with medical use and don’t by themselves equal a disorder
DSM-5 Substance-Use Disorders Severity
Mild - 2 or 3 symptoms present, Moderate - 4 or 5 symptoms present, Severe - 6 or more symptoms present
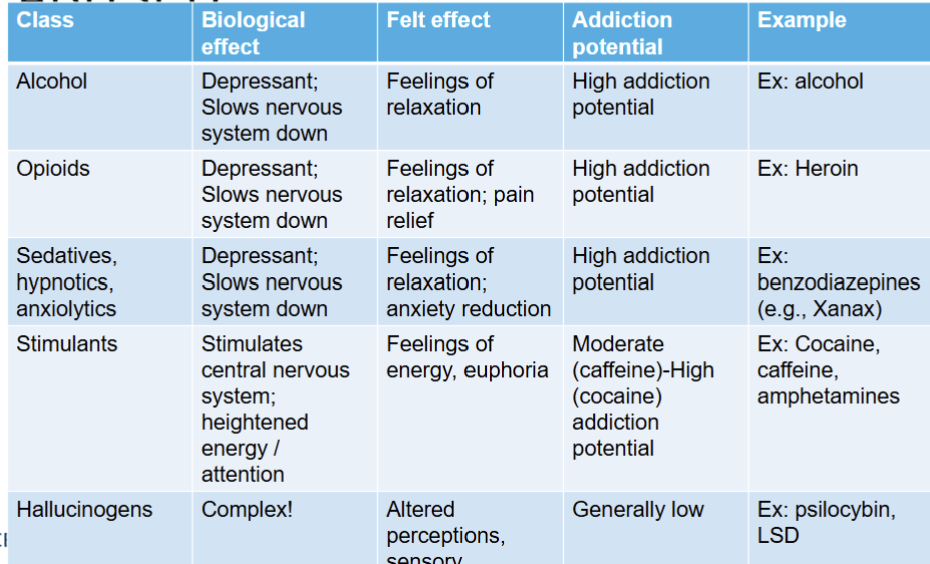
Substances with multiple effects
Nicotine - energy & relaxation felt; high addiction potential
Cannabis - relaxation & euphoria; moderate addiction potential
Ecstasy - feelings of connection & sensory distortions; moderate addiction potential; moderate addiction potential
GHB - relaxation & euphoria; high addiction potential
Alcohol abuse cuts across all…
Age, educational, occupational, and socioeconomic groups
Lifetime prevalence for alcohol abuse in the U.S. is
18%
Alcohol Use Disorder is ___ as likely to be diagnosed in men compared to women
2x
More than 37% of alcohol abusers suffer from
at least one coexisting psychological disorder
Progression of substance use to disorder
Individual decides to experiment with drugs → drug begins to serve important purpose; consumption continues → brain chemistry becomes altered from chronic use and physiological dependence, withdrawal symptoms, cravings arise → lifestyle changes occur due to chronic abuse
Typical progression toward drug abuse/dependence chart

Psychological Dimension of Substance Use Disorders
Coping with psychological stress and emotional symptoms as a major motive for substance use and relapse
Two Pathways in Substance Use Disorder (Psych Dimension) & which is research more focused upon
1) Negative mood (depression, anxiety) → substance use*
2) Substance use → negative mood
Substance Use Disorders / Biological Dimension
Genetic factors account for disorders & vary by substance
____ dependence appears to have stronger genetic risk
Cannabis
Substance Use Disorder / Social Dimension (PPA)
Parents - parental monitoring low / permissive attitude
Peers - peer pressure / social norms (social media)
Attitudes - desire to fit in / desire to rebel
In substance use disorders, relapse is ___
common
What helps recovery from Substance Use Disorders?
Combination treatment (therapy & medication), addressing comorbid conditions, stable life needs (employment)
Treatment for Substance Use / Behavioral Therapies
CBT - changing behavior and thinking
Motivational Interviewing - enhancing motivation to change
Contingency Management - rewards for positive behavior change
Treatment for Substance-Use Disorders / Medications
Negative reinforcement for use, lessen cravings (ex. nicotine gum and patches)
Treatment for Substance-Use Disorders / Social support
12-step programs (AA, NA), family involvement
Gambling Disorder
Compulsive desire to engage in gambling activities, diagnosed when a person exhibits at least 4 defining characteristics in 12 months, ranges in severity, relatively uncommon
Internet Gaming Disorder
Condition involving excessive and prolonged engagement in Internet games; diagnostic criteria (withdrawal, tolerance, impairment, distress) similar to gambling disorder