Exam 2: Brachial Plexus
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Dorsal nerve roots
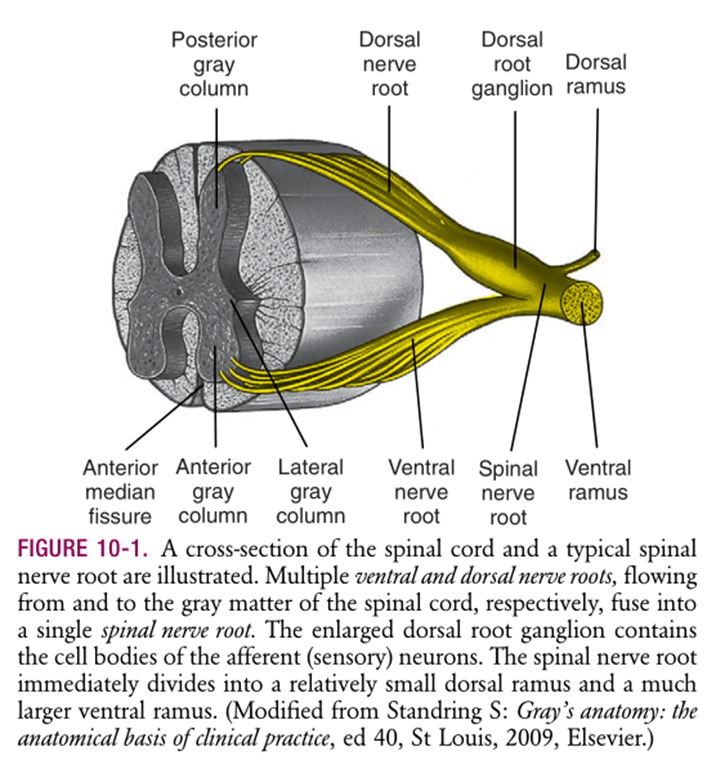
Input: incoming/afferent dendrites supplying sensory information with the neuron cell body located in an adjacent dorsal root ganglion
Sensory neurons transmit information to the spinal cord from muscle, joints, skin
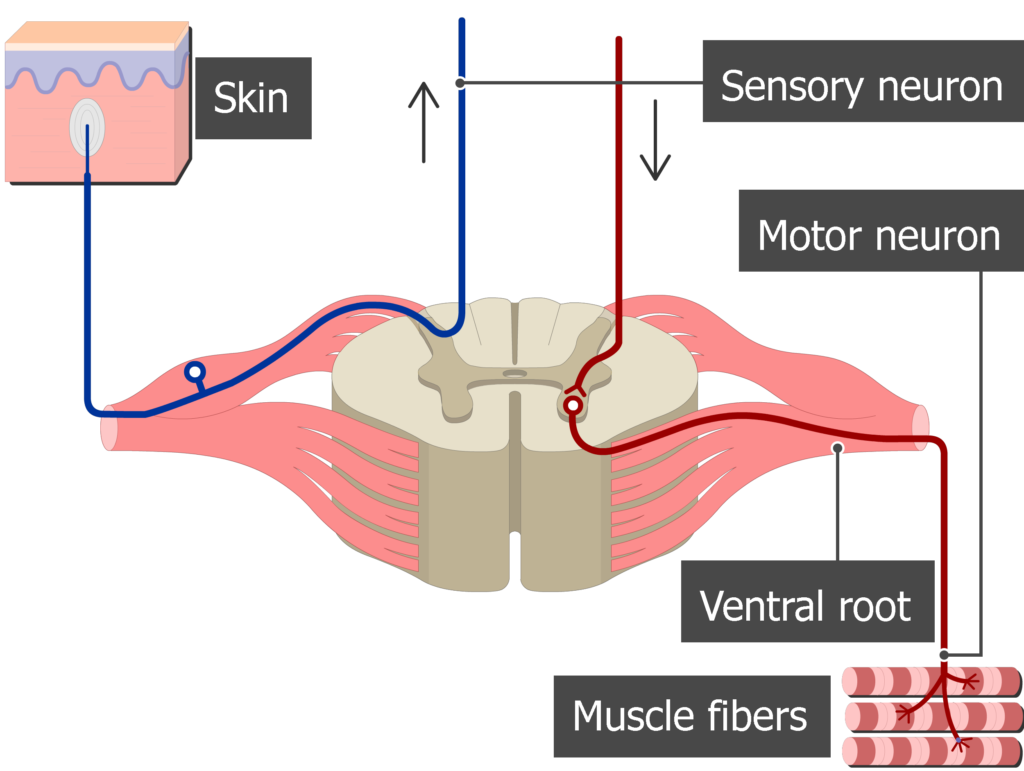
Ventral nerve roots
Output: outgoing/efferent axons supplying motor commands to muscles
Sensory end organs/inputs: Cutaneous Mechanoreceptors (Skin - touch, pressure)
Merkel Discs: Shape, edges, texture (object recognition)
Meissner Corpuscles: Light touch, movement (grip control)
Pacinian Corpuscles: Deep pressure, vibration (tool use)
Ruffini Endings: Skin stretch (hand shaping)
Sensory end organs/inputs: Proprioceptors: Muscles, tendons, joint position sense
Muscle Spindles: Muscle length & stretch
Golgi Tendon Organs: Muscle tension & force regulation
Joint Receptors: Joint position & movement
These are why you can close your eyes & touch your nose. Sensors tell the brain exactly where they are in 3D space.
High speed feedback loop!
Sensory end organs/inputs: Thermoreceptors & Nociceptors (free nerve endings)
• Temperature (heat & cold)
• Pain (mechanical, thermal, chemical)
Spinal Nerve Roots
Ventral (output) and dorsal (input) nerve roots join to form a spinal nerve root. Spinal nerve roots contain both sensory and motor fibers.
31 pairs of spinal nerve roots:
8 cervical nerve roots vs. 7 cervical vertebrae
Suboccipital nerve (C1) leaves the spinal cord between the occipital bone and the atlas (C1)
C1-C7 exit above the corresponding vertebrae
C8 spinal nerve root exits the spinal cord between C7 and T1
12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal
The rest of the spinal nerves after C8 exit below the corresponding vertebrae.
Dermatomes
Area of skin supplied by dorsal root/input of a spinal nerve.
Vary in pattern from one individual to another and overlap one another.
Used to identify location/level of nerve lesion
Nerve root compression or SCI
Dysfunction presents as diminished or altered sensation in the corresponding dermatome.
Dermatome screen: C5
Lateral upper arm
Dermatome screen: C6
Radial forearm to thumb
Dermatome screen: C7
Middle finger
Dermatome screen: C8
Small pinky finger
Dermatome screen: T1
Medial forearm
Myotomes - Motor
Identifies muscle/group of muscles innervated by the ventral root/output of a spinal nerve.
Dysfunction presents as weakness, atrophy, or paralysis in the corresponding myotome.
Both dermatomes and myotomes are used to identify high level lesions.
Myotome screen: C2-4
Shoulder shrug
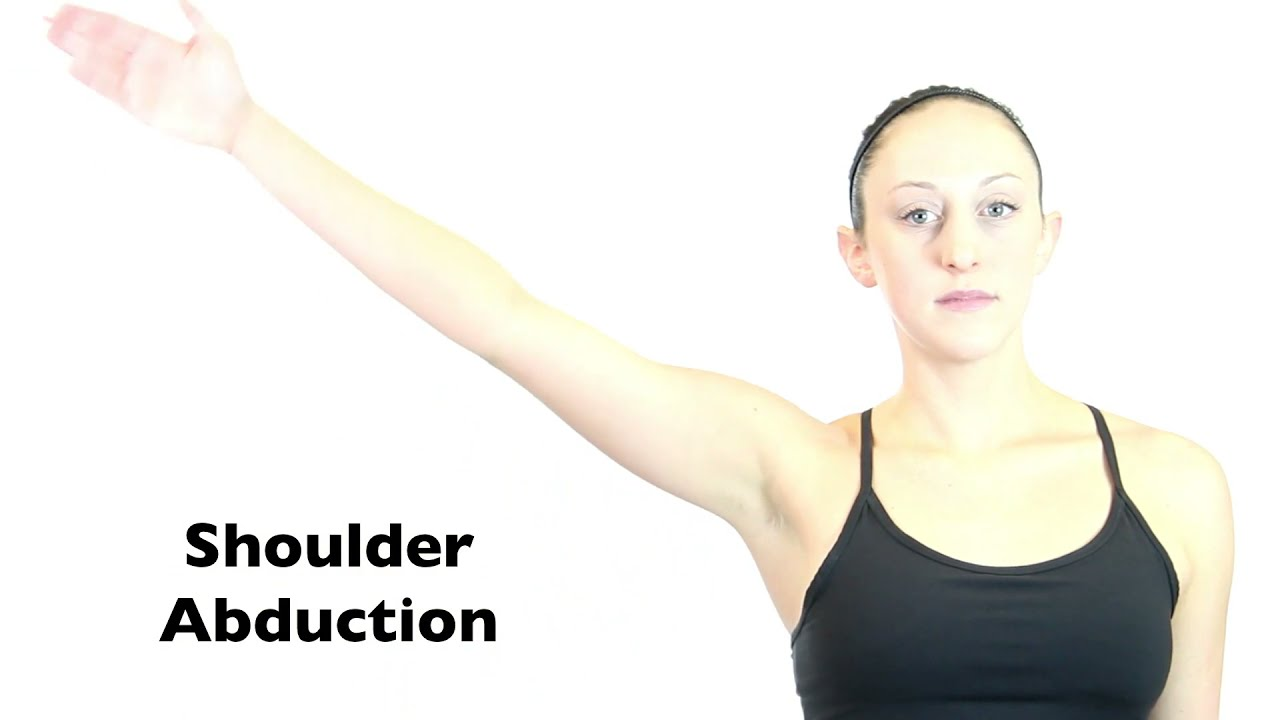
Myotome screen: C5
Shoulder abduction
Muscles: middle deltoid, supraspinatus (+trapezius, SA)
chicken wing; lift shoulders to side
Myotome screen: C5-C6
Elbow flexion
Bicep curl
C6 flexes elbow w/ biceps, but extends the wrist, pulling the hand back.
Myotome screen: C6
Wrist extension (pulls hand back)
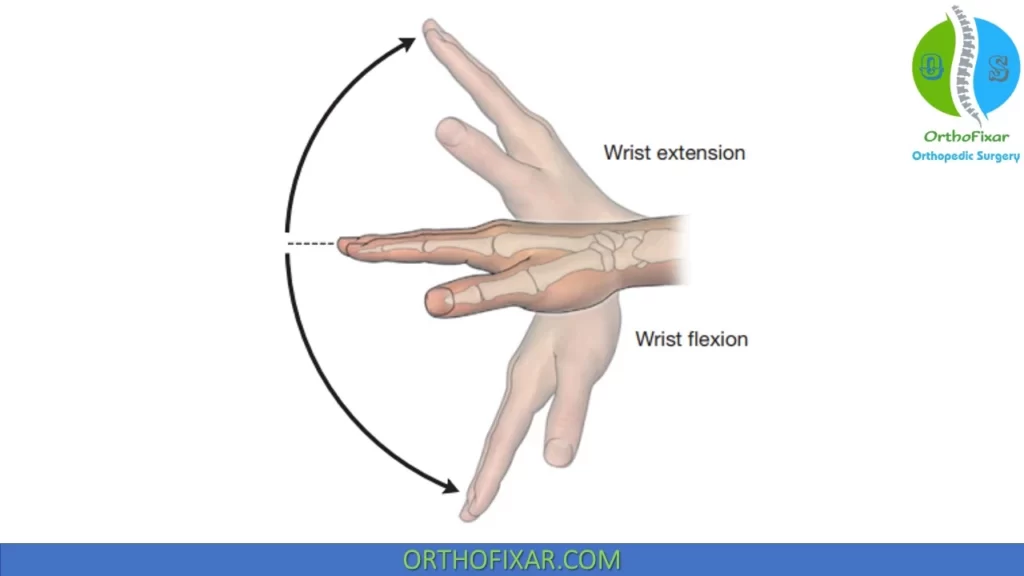
Myotome screen: C7
Wrist flexion (GAY) + Elbow Extension
Extending arm to reach something
Tricep extension: straighten arm, but flexes wrist
Myotome screen: C8
Thumb abduction
Gets fingers ready to grasp
Myotome screen: T1
Finger abduction & adduction
Plexus: an intermingling of ventral rami that form peripheral nerves carrying motor, sensory and sympathetic nerve fibers.
Only the ventral rami innervate limb muscles.
Each ventral ramus of a spinal nerve root either forms a plexus or continues as an individual named nerve.
4 major plexuses are formed by the ventral rami: Cervical, brachial, lumbar, sacral
Cervical (C1-C4) plexus
diaphragm and neck muscles + sensory innervation to neck
Brachial (C5-T1) plexus
upper extremity muscles + sensation
Lumbar (T12-L4) plexus
pelvis, thigh
Sacral (L4-S4) plexus
posterior thigh, lower leg and foot
Brachial plexus – Anatomy and palpation: Trunks
Lie in the neck
Brachial plexus – Anatomy and palpation: Divisions
adjacent to the subclavian artery (continues as axillary artery)
Palpate behind the midpoint of the clavicle to feel the pulse
Brachial plexus – Anatomy and palpation: Cords
extend from the midpoint of the clavicle to the coracoid process
Named based on anatomical relationship to the axillary artery
Palpate inferior to the lateral third of the clavicle
Brachial plexus: Terminal Nerves (5)
Musculocutaneous (C5, C6, C7)
Axillary (C5, C6)
Radial nerve (C5-T1)
Median nerve (C5-T1)
Ulnar nerve (C8-T1)
Brachial plexus: Injuries divided into 3 trunks
Upper trunk (Erb-Duchene C5-C6) = Waiter’s tip posture
Extended upper trunk (Erb-Duchene C5-C7)
Lower trunk (Dejerine-Klumpke C8-T1) = Neck & trunk separation
Brachial plexus: Vulnerable to?
Trauma: childbirth, motorcycle accidents
Susceptible to compression between the anterior and middle scalenes and underneath the pectoralis minor
Upper trunk and extended upper trunk lesion (Erb-Duchene C5-6 and C5-7)

“Waiter’s tip posture”: limp hanging arm
Paralysis of abduction and external rotation in the shoulder, making it pinned to the body/internally rotated
Lacking elbow flexion and supination
C7 involvement causes complete loss of wrist extension (Note: Wrist extension is mostly part of C6 but also partly involves C7 fibers)
Finger, wrist flexors, and hand intrinsics NOT involved.
Lower trunk (Dejerine-Klumpke C8-T1)

"Claw Hand" deformity: The hand appears clawed due to paralysis of the intrinsic hand muscles (interossei = abduction/adduction, lumbricals = flexion @ MCP and ICP joints).
Imbalance of flexors and extensors
Wrist may be in an extended or neutral position
Sensory Loss: Reduced sensation along the inner forearm and hand (C8-T1 dermatomes).
Proximal muscles spared
Musculocutaneous nerve (C5-7): primary motor functions
Elbow flexion & forearm supination
Biceps brachii, brachialis, coracobrachialis
Musculocutaneous nerve (C5-7): Sensory area
Lateral forearm
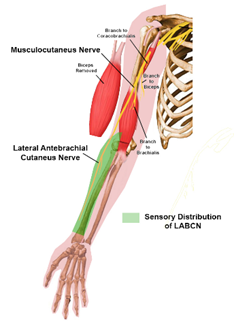
Musculocutaneous nerve (C5-7): Functional deficits
Weakness in elbow flexion (biceps atrophy)
Musculocutaneous nerve (C5-7): Functional tasks
Elbow flexion: lifting objects, hand to mouth
Forearm supination: turn palm up, turn doorknob
Shoulder flexion: reach forward, arm adduction
Axillary nerve (C5-6): primary motor functions
Shoulder abduction/initial lift & stabilization
Middle deltoid, teres minor
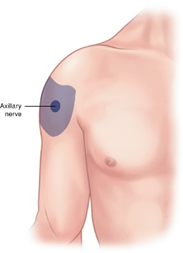
Axillary nerve (C5-6): sensory areas
Lateral shoulder/regimental badge area
Axillary nerve (C5-6): functional tasks
Arm abduction: lift arm away from body
Flexion/extension: move arm forward/back
Axillary nerve (C5-6): functional deficit
Limited shoulder abduction & extension (beyond movement initiated by rotator cuff)
Radial nerve (C5-T1): primary motor functions
elbow, wrist, finger extension
triceps & all major extensors of wrist & digits
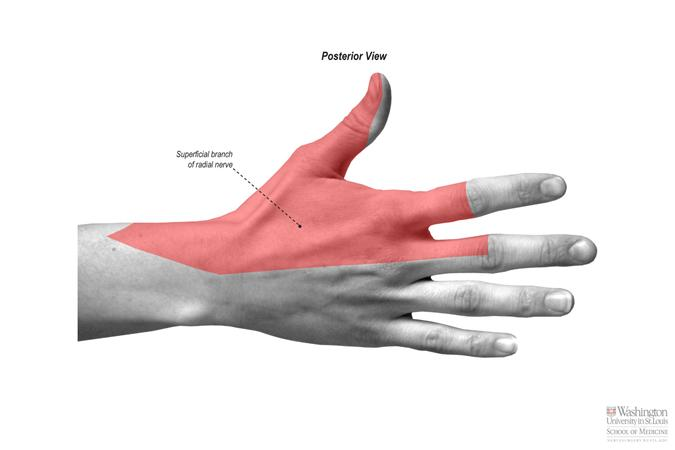
Radial nerve (C5-T1): sensory areas
posterior arm, forearm, dorsum of hand/radial side
Radial nerve (C5-T1): functional tasks
Wrist extension: lift hand up to release grasp
Finger & elbow extension: straighten fingers to open hand, straighten arm
Forearm supination: rotate palm up
Thumb extension/abduction: move thumb away from palm
Radial nerve (C5-T1)/extensors: deficits
Wrist drop
Median nerve (C5-T1): primary motor functions
Forearm pronation, wrist flexion, precision pinch
Most forearm flexors & thumb thenar muscles
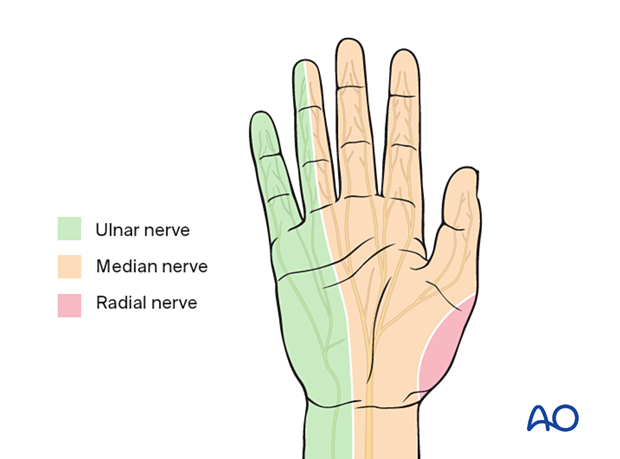
Median nerve (C5-T1): sensory areas
Palmar thumb
Index, middle, radial half of ring finger
Median nerve (C5-T1): functional tasks
Forearm pronation: turn palm down
Pinching & thumb opposition: tripod/pencil grasp
Finger & wrist flexion
Median nerve (C5-T1): deficits
Loss of thumb opposition (‘O’ position) & Carpal tunnel
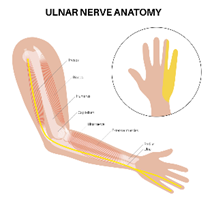
Ulnar nerve (C8-T1): primary motor functions
Intrinsic hand muscle control (fine motor coordination)
FCU, FDP digits 4+5, intrinsic hand muscles, hypothenar muscles
Also DOESN’T innervate any upper arm muscles
Ulnar nerve (C8-T1): sensory areas
Ulnar half of hand (palmar & dorsal side, since nerve splits & goes anterior & posterior)
Ulnar nerve (C8-T1): functional tasks
things that make clawing annoying
Power grip: strong grasp, holding cup ☕
Pinch grip: pinching a cheerio in-between thumb and index, hold thin paper 🤌
Finger manipulation: spread fingers/abduction; bring fingers together/adduction (typing, playing piano) 👋
Fine motor skills: pinky & ring finger
Ulnar nerve (C8-T1): deficits
Claw hand (Klumpke’s)
loss of finger abduction & adduction
Radial nerve motor innervation: upper arm
Triceps C6-8
Radial nerve motor innervation: Elbow
Brachioradialis (C5-6)
Brachialis (small C7 portion ONLY)
ECRB/L (C6-7)
Anconeus (C6-8)
Radial nerve motor innervation: Forearm/PIN group
Supinator (C6-7)
Distal extensor (C7-8): extensor carpi ulnaris (ECU)
Thumb extensors (C7-8):
Extensor pollicis longus (EPL)
Extensor pollicis brevis (EPB)
Abductor pollicis longus (APL)
Finger extensors (C7-8):
Extensor digitorum communis (EDC)
Extensor digiti minimi (EDM)
Extensor indicis proprius (EIP)
Why are triceps usually spared in humeral shaft radial nerve injuries?
The nerve branches that supply the triceps (long, lateral, and medial heads) arise proximal to the typical fracture site, while the radial nerve itself is injured further down in the spiral groove
The nerve only becomes susceptible to compression here as it passes against the bone
Median nerve loss: Anterior interosseous nerve palsy (AIN)
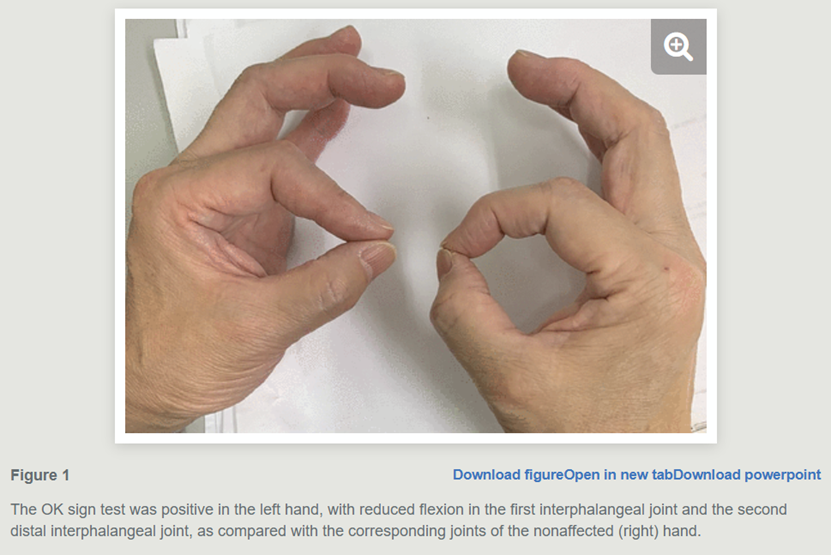
Deep motor branch of median n.
Can’t make perfect ‘O’; end up pressing finger pads together flat, like a pinch
Person IS opposing, can touch finger tip to finger tip
Muscle belly in thumb thenar shown
“OK” sign to see presentation; less round, more angular
Median nerve loss: Carpal tunnel syndrome

Can’t oppose/touch finger tip to tip
Loss of thenar muscles & sensation going into finger tips (eye of hands): compression of the median nerve in the wrist, resulting in pain, numbness, tingling, and weakness in the hand, especially in the thumb, index, and middle fingers
Screening: Try to make OK sign as round as possible; feels clumsy/weak when trying to pick up things
Ulnar nerve loss: High ulnar nerve lesion
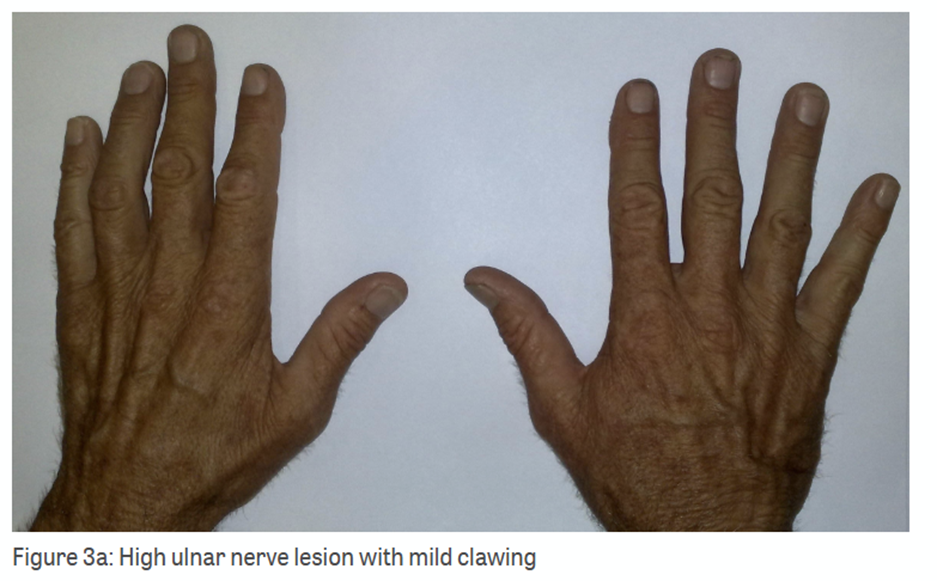
Hand muscles & deep forearm flexors (curl team) both paralyzed = hand looks flatter, less deformed
BUT WORSE! Lost grip strength AND fine motor control. Hand is useless
Ulnar nerve loss: Low ulnar n. lesion

Some grip, even though it looks bad
Nerve signals in forearm muscles are fine, pulling hard against paralyzed hand muscles, yanking fingers into claws
Curl team yes, balancing team NO
Visually more dramatic. Little muscles in hand when paralyzed = Flexors (curl team) WINS = CLAW!
Can still flex/move 4th and 5th fingers
Ulnar Paradox
A low lesion will typically present with more marked clawing of the little and ring fingers due to the unopposed action of the long flexors
Whereas: a high lesion around the elbow the clawing is more mild as the long flexors are affected too.
The more proximal (higher) the nerve injury, the greater the functional loss because all distal muscles and sensory areas supplied by that nerve are affected.
EX: Injuries at the level of the brachial plexus affecting whole trunks vs. injuries at the level of the terminal nerves
Within the specific terminal nerves: the pattern of deficit looks different depending on the specific branch of nerve that was injured
EX: AIN palsy and carpal tunnel both are caused by injuries to the median nerve but occur at different branches of the median nerve
A newborn presents with shoulder adduction, internal rotation, elbow extension, and forearm pronation. Wrist extension is preserved. Which nerve roots are affected?
C5, 6 (Erb-Duchenne palsy)
C5: Shoulder abduction → now shoulder adduction
C5-6: Elbow flexion → now elbow extension
A client presents to outpatient OT following a mid-shaft humeral fracture. They are unable to extend the wrist or fingers.
Which peripheral nerve is most likely injured?
In which anatomical plane does the primary deficit occur?
Radial nerve
Sagittal plane
A 19-year-old female college student while hiking, she slipped and reflexively grabbed a tree branch to break her fall. This caused sudden, forceful hyperabduction (upward traction) of her right arm. She reported difficulty with fine motor coordination and demonstrates a claw hand. She also experienced a loss of sensation or numbness along the medial aspect of the forearm and hand.
Which nerve roots and trunk are most likely involved?
Based on the sensory loss in the medial forearm, which specific cutaneous nerve has been affected?
Ulnar nerve C8 - T1, lower trunk
Medial antebrachial cutaneous n.