MLS Exam #1 (M)
1/316
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
317 Terms
What two hormones are stored in the posterior pituitary (remember, these do not have a true axis)?
ADH; oxytocin
Where is ADH produced & what are some of its effects?
Hypothalamus (but stored in posterior pituitary); vasoconstriction, stimulate free H2O retention in kidney (aka concentrate urine), stimulate ACTH release
What are the 2 forms of diabetes insipidus (DI)? What is each form characterized by?
1) Central (Neurogenic) DI: actual decrease in ADH production/release, often due to trauma of some kind
2) Nephrogenic DI: normal ADH production, but resistance to its effects at the kidney (aka ADH resistance)
What is a medication that can very commonly cause nephrogenic DI?
Lithium
What is the general pathophysiology of DI?
Decreased ADH production (central DI) or ADH resistance (nephrogenic DI) leads to decreased renal reabsorption of free H2O, ultimately causing patient to produce large volumes of very dilute urine
What are some classic s/sxs of DI?
Polydipsia, polyuria (very very dilute), +/- hypernatremia (high blood osmolality)
When taking a fasting ADH level, what results suggest central vs. nephrogenic DI?
Central: ADH will be low
Nephrogenic: ADH will be high
When performing a vasopressin challenge test, what results suggest central vs. nephrogenic DI?
Central: sxs likely improve w/ administration of DDAVP
Nephrogenic: sxs will not improve
Remember: vasopressin (DDVAP) is another name for ADH
When is a brain MRI indicated to assess DI?
For suspected central cases (body unable to produce (hypothalamus) or release (pituitary) ADH for some reason)
What are our first-line treatments for central & nephrogenic DI, respectively? What is another med we may add to refractory cases?
Central: synthetic DDVAP (desmopressin)
Nephrogenic: hydrochlorothiazide (HCTZ) diuretic
Refractory: indomethacin (an NSAID)
What is a med specifically indicated to treat lithium-induced DI?
Amiloride
If we are giving a patient IV fluid replacement for their DI, what is important to keep in mind?
We need to use hypotonic solutions, otherwise we may make cause/exacerbate hypernatremia
Although there are many many causes of syndrome of inappropriate ADH (SIADH), what are 2 common ones?
Various meds such as MDMA (ecstasy); small cell lung cancer (ectopic ADH)
What is the general pathophysiology of SIADH? What does it result in (specifically)?
An abnormal increase in ADH production leads to increased renal reabsorption of free H2O, ultimately resulting in euvolemic hypotonic hyponatremia
Again, what is the most common clinical presentation of SIADH?
Hyponatremia (nausea, malaise, lethargy, HA, disorientation, seizure, coma, respiratory arrest)
Is it usually necessary to draw a patient's ADH level if we suspect SIADH?
No, not usually
What are some general lab findings we expect to see with SIADH (Na+ levels, serum osmolality, urinary output, urine specific gravity)?
Sodium: decreased
Serum osmolality: decreased
Urine output: very low
Urine SG: increased
What is our treatment goal in SIADH?
Treat underlying cause & return Na+ to 125-130 mEq/L (normal level)
In general, what is panhypopituitarism?
Deficiency of ALL hormones secreted by the anterior pituitary; tends to happen in a very predictable pattern (GH --> FSH/LH --> TSH --> ACTH); it is also possible for the posterior pituitary to be affected
How would we go about working up a patient with suspected panhypopituitarism?
We would want to check both pituitary & end-organ hormone levels for all hormones, plus perform the appropriate stimulation tests to confirm
What is the treatment for panhypopituitarism?
Treat underlying cause + HRT (especially cortisol - hydrocortisone!!)
In general, what is empty sella syndrome (ESS)? Do patients always have sxs?
Enlargement of sella turcica + filling w/ CSF; can compress pituitary, but often patients are asymptomatic

What is a classic MRI sign of ESS?
"Infundibulum sign" (pituitary stalk is present, it's just compressed)

How would we go about working up a patient with suspected ESS?
We would want to check both pituitary & end-organ hormone levels for all hormones, plus perform the appropriate stimulation tests to confirm
What is insulin released by, and what triggers its release?
β-cells in the Islets of Langerhan found in the pancreas in response to elevated blood glucose levels
What is the effect of insulin on adipose tissue?
Enhances glucose uptake by adipocytes via lipogenesis (glucose -> glycerol -> TGs) & inhibits lipolysis
Why is it significant that insulin inhibits lipolysis in adipocytes?
It is the most sensitive pathway of insulin action (1st thing to be affected if insulin levels change)
What is the effect of insulin on skeletal muscle?
Enhances glucose uptake by myocytes via glycogenesis (glucose -> glycogen) as well as increasing protein synthesis & preventing protein catabolism
Why is the liver unique in terms of glucose uptake?
It is NOT insulin-mediated as in adipocytes and myocytes
What is the effect of insulin on the liver?
Glycogenesis (glucose -> glycogen) UP TO A POINT (it is saturable); after this point excess glucose is turned into glycerol which combines w/ FFAs to form TGs (lipogenesis - just like adipocyte pathway)
Insulin also inhibits gluconeogenesis & ketogenesis in the liver
How does down-regulation of insulin receptors perpetuate IR?
As insulin levels increase/remain high, the body says "woah I don't need all these insulin receptors" and down-regulates them, perpetuating resistance
How does IR perpetuate itself in terms of adipose tissues/adipocytes, and what does this lead to?
Adipocytes are unable to uptake glucose due to the IR, so they increase lipolysis in an attempt to provide alternative (non-glucose) sources of fuel (i.e. FFAs) creating a downward spiral of lipotoxicity
High FFA levels worsen IR through a variety of ways such as gluconeogenesis, ketogenesis, etc.
How does IR perpetuate itself in terms of skeletal muscle/myocytes, and what does this lead to?
Just like with adipose tissue, myocytes are unable to uptake glucose due to the IR, so they increase glycogenolysis & protein catabolism in an attempt to provide alternative (non-glucose) sources of fuel (i.e. FFAs, AAs)
These FFAs & AAs are subsequently used in processes like gluconeogenesis & ketogenesis, worsening the IR
Although glucose uptake is NOT insulin-mediated in the liver, how does IR still perpetuate itself here?
Hyperinsulinemia (due to IR) causes glycogenesis to occur and rapidly saturate the liver. Following this, the liver will convert all of the remaining excess glucose into TGs via lipogenesis (glucose -> glycerol -> TG) which are carried to adipose tissue via VLDLs and stored there (this is all normal liver response to insulin, it's just happening quickly here because there's high insulin)
Once in the adipose tissue, however, all these extra TGs are now susceptible to the disordered effects of IR on adipocytes: lipolysis -> lipotoxicity -> increased gluconeogenesis & ketogenesis, etc.
By definition, what is gluconeogenesis?
Generation of glucose molecules from non-CHO sources (pyruvate, lactate, AAs, glycerol, FFAs, etc.)
By definition, what is ketogenesis?
Oxidation of FFAs or AAs to produce ketone bodies
In general, what is obesity?
Adipocyte hyperplasia (increase in number) and hypertrophy (increase in lipid deposition within them)
Which type of adipose tissue (visceral or subcutaneous) has more adverse metabolic effects and is considered to be more harmful?
Visceral
What BMI values are considered to be normal, overweight, and obese, respectively?
Normal: 18.5-24.9 kg/m²
Overweight: 25-29.9 kg/m²
Obese: ≥ 30 kg/m² (class III morbid obesity = ≥ 40)
How does obesity contribute/perpetuate IR in terms of adipose tissue?
By definition, obesity is hyperplasia & hypertrophy of adipose tissue. In IR, adipocytes activate lipolysis in an attempt to create alternative (non-glucose) sources of fuel. FFAs, a product of lipolysis, perpetuate IR in several ways
Why is visceral adipose tissue considered to be more metabolically active & thus more harmful?
It is (1) less sensitive to insulin & thus cannot prevent lipolysis as effectively and (2) is more sensitive to hormones like glucagon, which increases BG
What is the relationship between how obesity & adipokine dysregulation perpetuates IR?
Obesity causes the release of several pro-inflammatory adipokines, stimulate production of CRP & fibrinogen (clotting), & decreases other adipokines such as leptin leading to hunger & overfeeding
Many of these pro-inflammatory adipokines directly perpetuate IR via their MOAs but it's beyond our scope
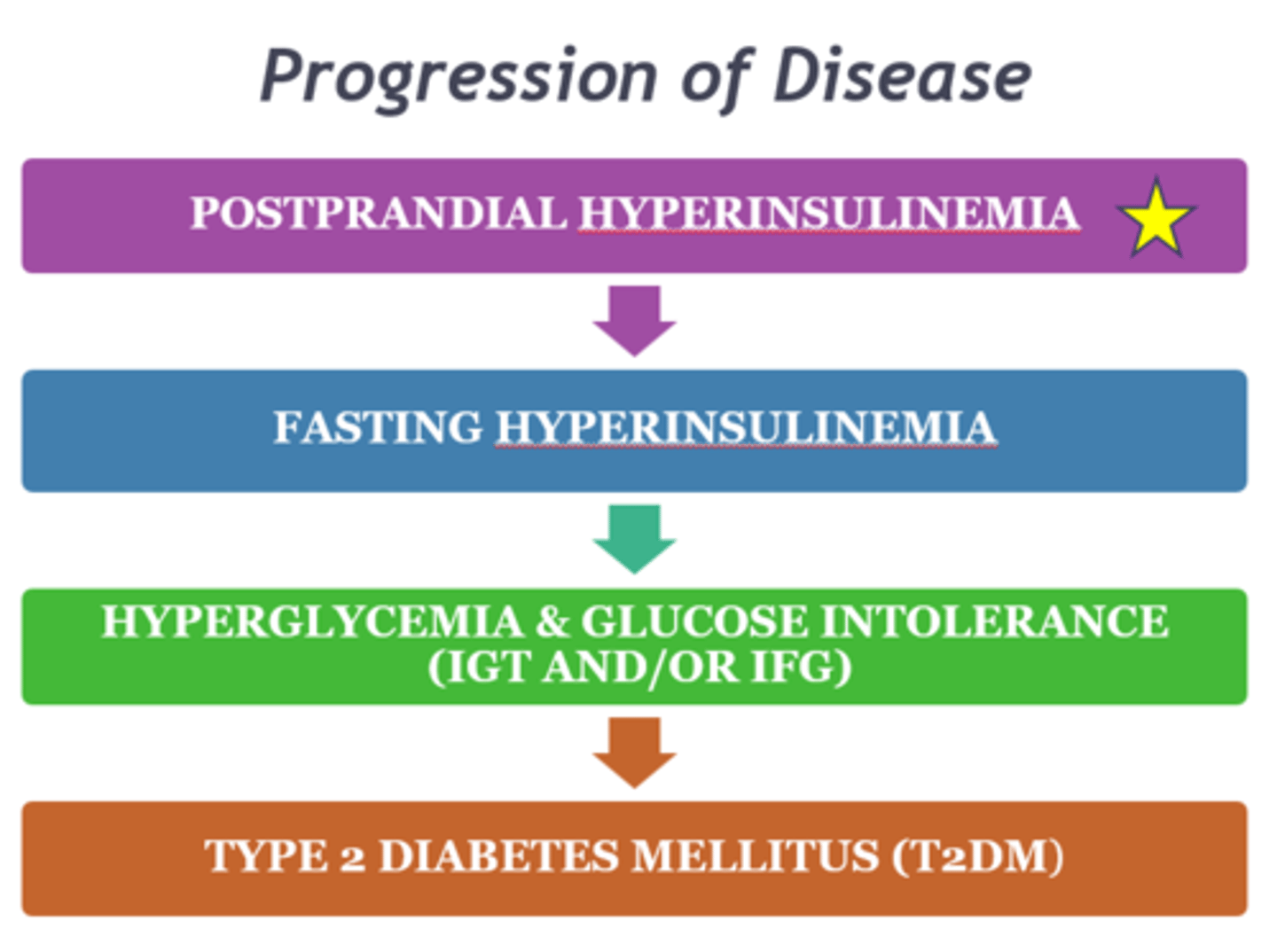
What is the first step/sign we will see in the disease progression of insulin resistance & T2DM?
Postprandial hyperinsulinemia
What is the best dyslipidemia-related marker that we have of IR?
Hypertriglyceridemia (high TGs)
JUST KNOW: increased sdLDLs, HTN, hyperuricemia, inflammation, & hypercoagulability are all side effects of IR/hyperinsulinemia. There are several complex physiologic reasons this happens
What 2 diseases does metabolic syndrome put patients at greatly increased risk of?
1) T2DM
2) CVD
What is the main pathophysiologic driving force behind the development of metabolic syndrome? What is the greatest risk factor?
Insulin resistance; obesity
What is the diagnostic criteria for metabolic syndrome as defined by NCEP ATP III?
Three or more of the following:
1) Central obesity (WC > 40 in for males, > 35 in for females)
2) Hypertriglyceridemia (≥ 150 mg/dL)
3) Low HDL (< 40 for males, < 50 for females)
4) High BP (≥ 130 systolic or ≥ 85 diastolic)
5) Fasting hyperglycemia (≥ 100 mg/dL)
If any of these values are normal but the patient is being currently treated for the condition, they still fulfill the criteria
JUST KNOW: nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), PCOS, and obstructive sleep apnea (OSA) are all highly associated with IR
What is acanthosis nigricans?
Darkened patches of velvet-like skin that is a classic PE finding of IR

What is the most important lifestyle change a patient can make to lose weight? What about maintain weight loss?
Lose weight: diet (caloric reduction)
Maintain weight loss: increase physical activity
What class of medication is very effective for weight loss in patients with metabolic syndrome?
GLP-1 receptor agonists
What class of medication is very effective for dyslipidemia therapy in patients w/ metabolic syndrome?
Statins
What class(es) of medication(s) is/are very effective for hypertension management in patients w/ metabolic syndrome?
ACEi/ARBs
What class(es) of medication(s) is/are very effective for hyperglycemia management in patients w/ metabolic syndrome?
Biguanides (metformin); thiazolidinediones (TZDs)
Actually more important than the GLP agonists for managing IR because they address the underlying cause - they increase insulin sensitivity
What is the general pathophysiology of Type 1 DM?
Autoimmune destruction of β-cells leads to an inability to produce sufficient insulin
What is the difference between Type 1A and Type 1B DM?
Type 1A: >95% of cases, autoantibodies identified
Type 1B: <5% of cases, idiopathic
What is the general pathophysiology of Type 2 DM?
Gradual progression of insulin resistance leads to a vicious cycle of worsening loss of blood glucose control
In terms of speed of onset, how do T1DM and T2DM differ?
Type 1 generally occurs very rapidly from insult->disease while Type 2 generally progresses slowly over many years
What is latent autoimmune diabetes of adulthood (LADA)?
Atypical, milder form of Type 1 DM that develops in adulthood; patient will gradually lose β-cell function over time and will eventually require insulin
What is gestational diabetes mellitus (GDM)?
Form of diabetes that develops in pregnant women
What is maturity-onset diabetes of the young (MODY)?
Autosomal dominant trait that leads to impaired insulin secretion; primarily affects non-obese patients <25 y/o (no clinical evidence of IR)
JUST KNOW: there are various genetic mutations & secondary causes such as endocrine disorders/tumors, pancreatic disorders, & medications that can also produce DM, but these are not nearly as common
What are some common s/sxs of DM (all types)?
Polyuria, polydipsia, polyphagia w/ weight loss (T1), weakness/fatigue, blurred vision, vulvovaginitis/balanitis, peripheral neuropathy, nocturnal enuresis (T1), or completely asymptomatic (T2)
What fasting plasma glucose (FPG) levels signify normal, impaired glucose tolerance (IGT), & DM, respectively?
Normal: < 100 mg/dL
IGT: 100-125 mg/dL
DM: ≥ 126 mg/dL
What 2-hr postprandial glucose levels signify normal, IGT, & DM, respectively?
Normal: < 140 mg/dL
IGT: 140-199 mg/dL
DM: ≥ 200 mg/dL
What HbA1c levels signify normal, IGT, & DM, respectively?
Normal: < 5.7%
IGT: 5.7-6.4%
DM: ≥ 6.5%
Why is coronary disease (CAD, MI) relevant to DM?
It is the leading cause of death in Type 2 patients
JUST KNOW: although coronary disease may be the leading cause of death in Type 2 diabetic patients, cerebrovascular disease and peripheral vascular disease - including gangrene - are also VERYY common in these patients and must be considered on examination - these patients are many times at risk of developing these conditions
At what BP threshold do we decide to treat patients for HTN? What is our preferred class of meds for this, and what is our BP goal for them?
≥ 130/80; ACEi or ARBs; goal = < 130/80
What is our preferred class of meds to treat dyslipidemia in diabetic patients?
Statins
What are 2 classes of meds that have CV benefit for Type 2 diabetic patients?
SGLT2 inhibitors; GLP-1 receptor agonists
How is diabetic nephropathy relevant to DM? How do we screen diabetic patients for it?
It is the 2nd leading cause of CKD (HTN is first); annual UACR
What is finerenone?
Agent similar to aldosterone (but is non-steroidal) that is indicated very specifically for T2DM patients w/ CKD + albuminuria on maximally-tolerated ACEi/ARB
How is peripheral neuropathy relevant to DM? How do we screen for it?
It is the most common complication of DM; annual diabetic foot exam + monofilament
How does peripheral neuropathy usually present?
In a "stocking-glove" pattern, sensory loss usually occurs first followed by motor changes (like decreased reflexes)
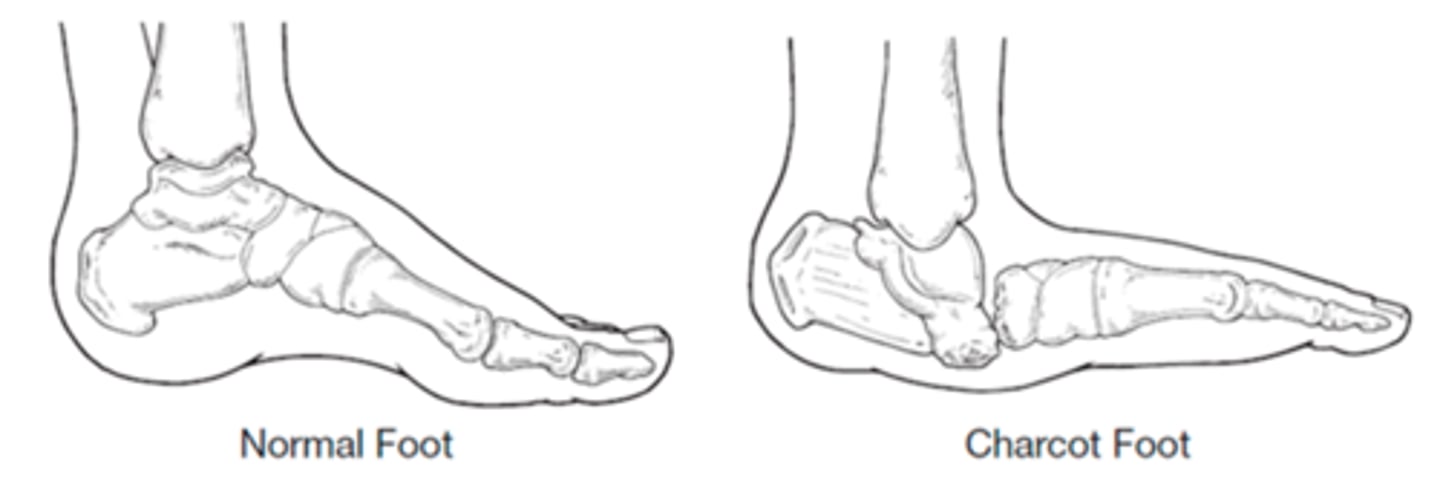
What is Charcot foot arthropathy?
Deformity of the foot secondary to the motor changes of diabetic neuropathy that leaves the patient susceptible to callus & ulcer formation
What are the only 2 FDA-approved drugs available for diabetic neuropathy?
Pregabalin (an anti-epileptic) and duloxetine (an SNRI)
What are 4 possible complications of central (autonomic) neuropathy in diabetic patients?
Orthostasis; gastroparesis; erectile dysfunction; neurogenic bladder
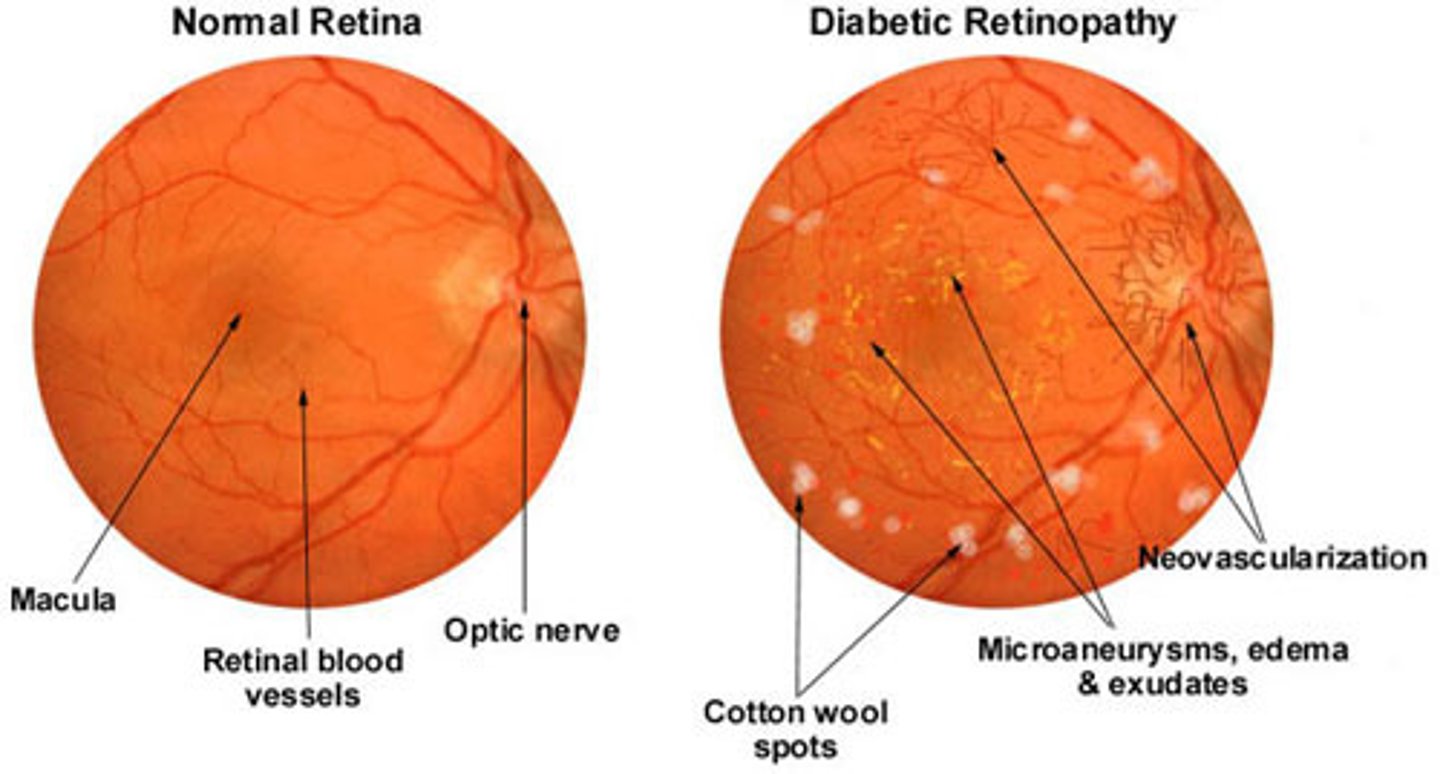
What are some eye pathologies that can develop secondary to DM? How do we screen for these?
Diabetic cataracts; glaucoma; diabetic retinopathy (proliferative vs. non-proliferative); annual ophthalmologist visits
What is disseminated granuloma annulare?
Ring/arc-shaped lesions that are raised & sharply-defined; may develop secondary to DM; easily mistaken for tinea

What is diabetic dermopathy?
Light brown scaly patches that do not hurt, open up, or itch (d/dx from venous stasis); may develop secondary to DM

What is necrobiosis lipoidica diabeticorum (NLD)?
Appears similar to diabetic dermopathy but is fewer, larger, deeper, & may be itchy, painful, or open up; may develop secondary to DM

What is bullosis diabeticorum?
Diabetic blisters that may develop secondary to DM

What is digital sclerosis?
Development of thick, waxy skin that can lead to joint stiffness; may develop secondary to DM

What are some MSK pathologies that can develop secondary to DM?
Hyperuricemia/gout; osteoporosis; inflammation or glycosylation of collagen & synovium (tightens up tissues); Charcot's deformity; digital sclerosis
According to the most recent guidelines, at what age do we begin screening asymptomatic adults for T2DM? If results are normal, how often do we repeat testing?
Beginning at age 35; every 3 years
What are 4 groups of people who warrant T2DM screening at any age?
1) Overweight/obese patients w/ ≥ 1 additional risk factor(s)
2) Patients w/ HIV
3) Patients on high-risk meds
4) Patients w/ a hx of pancreatitis
If a patient has a hx of GDM, how often/how long do they require T2DM screening for?
Every 1-3 years for life
As a Clinical Science refresher, what are our options to screen for T2DM?
HbA1c, FGP, 2-hr PP OGTT are all appropriate
What group of children warrant screening for T2DM? When do we begin this, and how often is it done?
Overweight/obese w/ ≥ 1 additional risk factor; begin after age 10 onset of puberty; every 3 years
Although it's not very common, what are 2 situations that may warrant a patient to be screened for T1DM?
1) Positive fhx of T1DM in a first-degree relative
2) Hx/fhx of autoimmunity
What is the most important obligation of the clinician who provides initial care to the diabetic patient?
EDUCATION of the patient and the family
In terms of medication, what are the mainstays of therapy for Type 1 and Type 2 DM, respectively?
Type 1: insulin
Type 2: metformin (caution w/ renal dysfunction)
Although HbA1c goals must be individualized to the patient, what are our general targets for most non-pregnant patients according to the ADA and AACE, respectively?
ADA: < 7%
AACE: < 6.5%
What are our general FBG & 1-2-hr postprandial glucose targets for most patients, respectively?
FBG: 80-130 mg/dL
1-hr: < 180 mg/dL
2-hr: < 150 mg/dL
What is the most common treatment complication in diabetic patients? How is it treated?
Hypoglycemia (particularly if they're on insulin therapy); PO CHO ingestion if able, parenteral glucagon if emergency
What are some s/sxs of hypoglycemia?
Jitteriness/shaking (1st to appear), tachycardia, palpitations, sweating, nausea, irritability, confusion, HA/fatigue, seizure, LOC/coma
What common anti-HTN med can contribute to "hypoglycemic unawareness?"
β-blockers
What is the Somogyi effect?
Patient experiences hypoglycemia overnight due to heightened insulin level (counter-regulatory hormones respond by raising BG); presents as persistent/recurring hyperglycemia in morning despite therapy