Part 3: Dermatitis, Allergic Contact Dermatitis, Stasis Dermatitis, Psoriasis, Scleroderma, Hives, Atopic Dermatitis, Drug Reactions, TEN, Stevens-Johnson Syndrome, and SLE
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
inflammatory/vascular skin disorders
allergic contact dermatitis
stasis dermatitis
psoriasis
scleroderma
allergic & hypersensitivity dermatoses
psoriasis
lupus
What are inflammatory skin disorders?
Conditions characterized by inflammation of the skin resulting from immune, allergic, vascular, infectious, genetic, or environmental factors.
What inflammatory and vascular skin disorders were covered in this lecture?
Allergic contact dermatitis, stasis dermatitis, psoriasis, scleroderma, hives (urticaria), atopic dermatitis, drug-induced skin eruptions, and systemic lupus erythematosus (SLE).
What is dermatitis?
Inflammation of the skin caused by various irritants, allergens, injuries, or immune responses.
What stimuli can trigger dermatitis?
Drugs
chemical allergens
ultraviolet radiation
trauma
metabolic disorders
immunologic disorders.
What are manifestations of acute dermatitis?
Red, exudative skin with numerous minute erosions and crusts.
How does dermatitis appear in later stages?
The skin becomes thickened, dry, and scaly.
ex. chronic eczema gets thicker → prescribe cortisol = thin skin
How is dermatitis diagnosed?
Through clinical evaluation and assessment of lesion distribution.
contact dermatitis
morph pattern = eczema
location = site of allergen contacts
freq = most common
severity = distressing, recurrent
atopic dermatitis
morph pattern = eczema
location = face → extremities
freq = common
severity = disfiguring, impaired function
seborrheic dermatitis
morph pattern = greasy, scaling
location = scalp, face, trink
freq = common
severity = variable
light-induced dermatitis
morph pattern = eczema or rash
location = exposed skin
freq = common
severity = mild
exfoliative dermatitis
morph pattern = sloughing of superficial epidermis
location = total body
freq = uncommon
severity = may be fatal
What is allergic contact dermatitis?
A Type IV delayed hypersensitivity reaction that occurs after exposure to an allergen.
What type of hypersensitivity reaction causes allergic contact dermatitis?
Type IV delayed hypersensitivity reaction.
How does allergic contact dermatitis develop?
An allergen contacts the skin and binds to a carrier protein, forming a sensitizing antigen.
What happens after an allergen binds to a carrier protein?
Langerhans cells process the antigen and present it to T lymphocytes.
What role do Langerhans cells play in allergic contact dermatitis?
They process allergens and present them to T cells, initiating sensitization.
What happens to T cells during allergic contact dermatitis?
They become sensitized and mount an immune response upon future exposure.
What are the clinical manifestations of allergic contact dermatitis?
Red papules, plaques,
sharply circumscribed vesicles,
swelling,
itching,
occasionally blister formation. = poison ivy

What are papules?
Small raised solid lesions less than 1 cm in diameter.
What are plaques?
Raised, flat-topped lesions larger than 1 cm.
What type of lesion commonly develops in poison ivy exposure?
Blisters and vesicles.
What symptom is often most bothersome in allergic contact dermatitis?
Pruritus (itching).
What is the primary treatment goal for allergic contact dermatitis?
Removal of the triggering allergen and reduction of inflammation. (antihistamine + topical corticosteroids)
What is stasis dermatitis?
A skin disorder caused by chronic venous insufficiency and poor circulation in the lower extremities.
blood pools in lower legs
What causes stasis dermatitis?
Venous stasis, edema, and vascular trauma to the lower legs.
How does poor circulation contribute to stasis dermatitis?
Pooling of blood causes inflammation and skin changes in the lower extremities.
What are manifestations of stasis dermatitis?
Erythema
progressing
pruritus
scaling
petechiae
ulcerations. + changes in shape of leg

What is erythema? - stasis dermatitis
Redness of the skin caused by increased blood flow.
What are petechiae? - stasis dermatitis
Small pinpoint hemorrhages beneath the skin.
Why are ulcerations common in stasis dermatitis?
Poor circulation impairs tissue oxygenation and healing.
What is psoriasis?
A chronic autoimmune inflammatory skin disease characterized by excessive epidermal cell turnover.
polygenic bases
What is the underlying cause of psoriasis?
Autoimmune activation involving T cells and inflammatory cytokines.
T cells release cytokines + growth factor
What role do T cells play in psoriasis?
They release cytokines and growth factors that stimulate abnormal skin cell growth.
How do cytokines contribute to psoriasis?
They trigger excessive keratinocyte proliferation and inflammation.
What are keratinocytes?
The predominant cells of the epidermis responsible for producing keratin.
How are dermal blood vessels affected in psoriasis?
They undergo abnormal growth and increased vascularity.
Which inflammatory cells infiltrate psoriatic lesions?
Neutrophils and monocytes.
What effect does inflammation have in psoriasis?
It contributes to redness, swelling, pain, and plaque formation.

What is the hallmark pathological process in psoriasis?
Rapid turnover of epidermal cells.
What are the characteristic skin lesions of psoriasis?
Reddish, silver-scaled maculopapular plaques.
Where are psoriasis lesions commonly found?
Elbows, knees, scalp, and trunk.
What symptoms accompany psoriasis?
Itching, burning, pain, and scaling.
How severe can psoriasis symptoms become?
They range from mild localized disease to severe widespread involvement.
What are first-line topical treatments for psoriasis?
Topical corticosteroids and emollients.
What systemic immunosuppressant may be used for severe psoriasis?
Cyclosporine.
What biologic medication was discussed for psoriasis?
Humira (adalimumab).
What is phototherapy? - psoriasis
Treatment using ultraviolet light to reduce skin inflammation and excessive cell growth.
Why is phototherapy effective in psoriasis?
It slows keratinocyte proliferation and reduces inflammation.
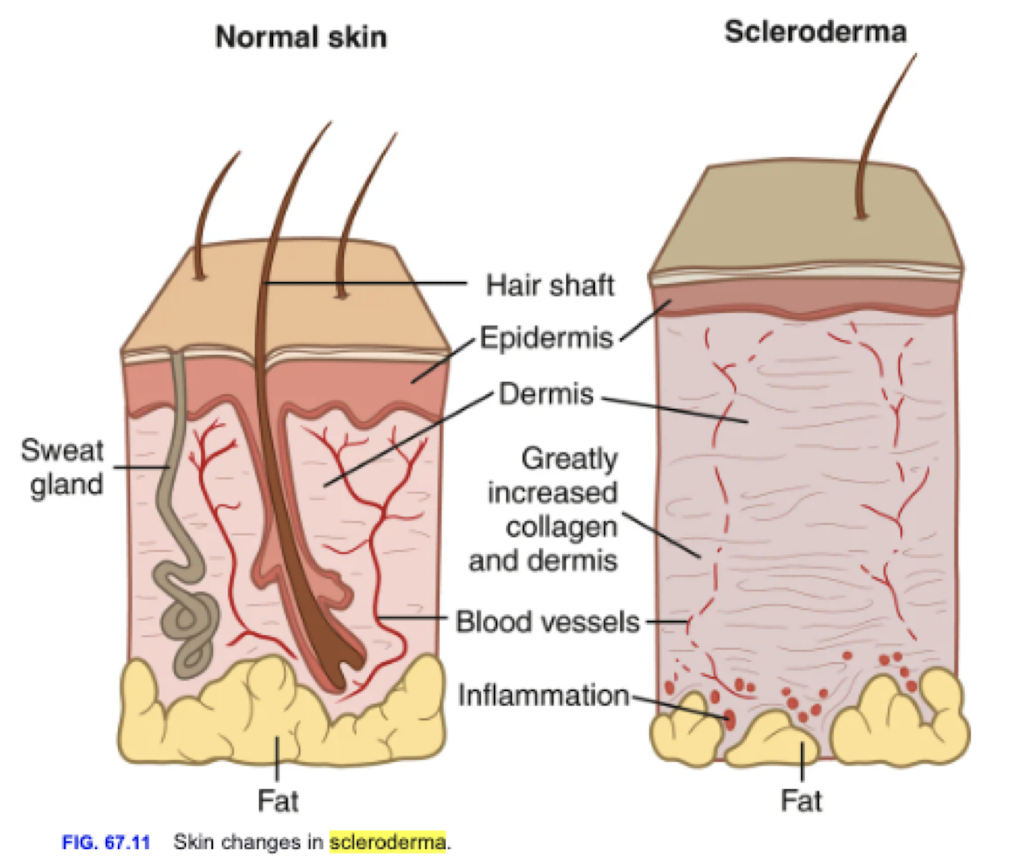
What is scleroderma?
An autoimmune connective tissue disease characterized by fibrosis and vascular abnormalities.
overproduction of collagen = stiffness + occlusion of blood vessels
What body systems can be affected by scleroderma?
Skin, blood vessels, synovium, musculoskeletal system, and internal organs.
What causes skin thickening in scleroderma?
Fibroblast activation leading to excessive collagen production.
What is fibrosis? - scleroderma
Excessive formation of connective tissue leading to hardening and thickening of tissues.
How does inflammation contribute to scleroderma?
It stimulates collagen overproduction and progressive fibrosis.
What happens to blood vessels in scleroderma?
They become narrowed and occluded due to fibrosis and vascular damage.
What is sclerodactyly?
Thickening and tightening of the skin of the fingers.

What are the characteristic skin findings in scleroderma?
Hard, taut, hypopigmented skin tightly attached to underlying tissues.
Can scleroderma be localized?
Yes, localized forms primarily affect the skin.
Can scleroderma become systemic?
Yes, diffuse forms can affect internal organs.
What is the pathological hallmark of scleroderma lesions?
Massive collagen deposition with inflammation and vascular changes.
CREST - scleroderma
C = calcinosis = Ca+ deposits in skin (light-up on x-ray)
R = Raynaud’s phenomenon = spasm of blood vessels in response to cold/stress (white/purple)
E = esophageal dysfunction = acid-refux/decrease motility
S = Sclerodactyly = tjock/tight fingers
T = Telangiectasias = dilation of capillaries = red marks on skin + spider veins
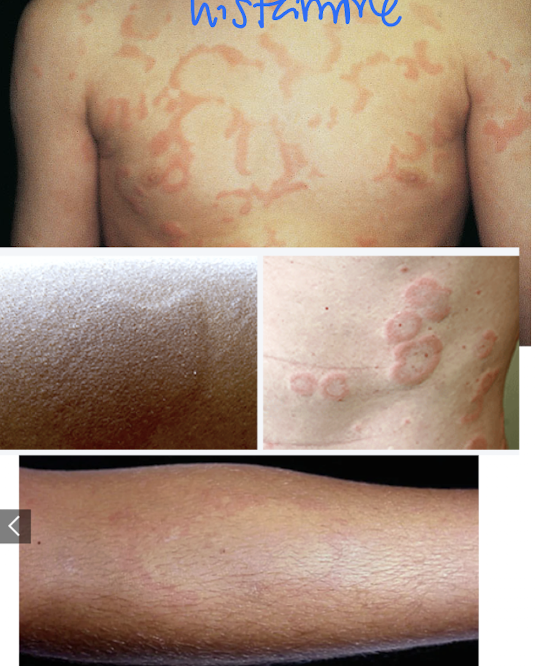
What are hives?
Acute eruptions of itchy raised wheals surrounded by erythema.
What is another name for hives?
Urticaria.
What causes urticaria?
Allergic reactions, infections, exercise, or other triggers causing histamine release.
What is a wheal?
A raised, transient area of localized edema in the skin.

Why do hives itch?
Histamine release stimulates nerve endings in the skin.
What treatments are used for urticaria?
Removal of the trigger
antihistamines
does not remove hives, only takes away itch
corticosteroids
cool compresses.
How do antihistamines help hives?
They block histamine receptors and reduce itching and swelling.
What is atopic dermatitis?
A chronic relapsing inflammatory skin disorder commonly known as eczema.
type I hypersensitivity rxn
What type of hypersensitivity reaction is associated with atopic dermatitis?
Type I hypersensitivity reaction.
What are the hallmark symptoms of eczema?
Chronic itching, inflammation, dryness, and recurrent flare-ups.
What factors contribute to atopic dermatitis?
Genetics
atopy (food allergies, asthma)
environmental factors (dry environments, seafood)
What does atopy mean?
A genetic tendency to develop allergic diseases.
What is the primary symptom of eczema?
Pruritus.
How is atopic dermatitis treated?
Skin lubrication
must keep moist
topical corticosteroids
acute flare-up
antibiotics if infection develops.
Why are moisturizers important in eczema?
They restore the skin barrier and reduce water loss.
What is erythema multiforme?
A self-limiting skin reaction that commonly occurs after infection.
macula patones

What is the prognosis for erythema multiforme?
Usually self-limiting and resolves without significant complications.
What is anaphylaxis?
A severe life-threatening systemic allergic reaction.
2+ systems
resp
skin
GI
What are drug-induced skin eruptions?
Skin reactions caused by medications.
Steven-Johnson
TEN (toxic epidermal necrolysis)
What is Stevens-Johnson syndrome (SJS)?
A severe mucocutaneous reaction characterized by epidermal detachment involving less than 10% of body surface area.

What causes Stevens-Johnson syndrome?
Most commonly medication reactions.
How much body surface area is involved in SJS?
Less than 10%.
Does Stevens-Johnson syndrome involve mucous membranes?
Yes, mucosal involvement is a hallmark feature.
What is toxic epidermal necrolysis (TEN)?
A severe life-threatening skin disorder characterized by widespread epidermal detachment.
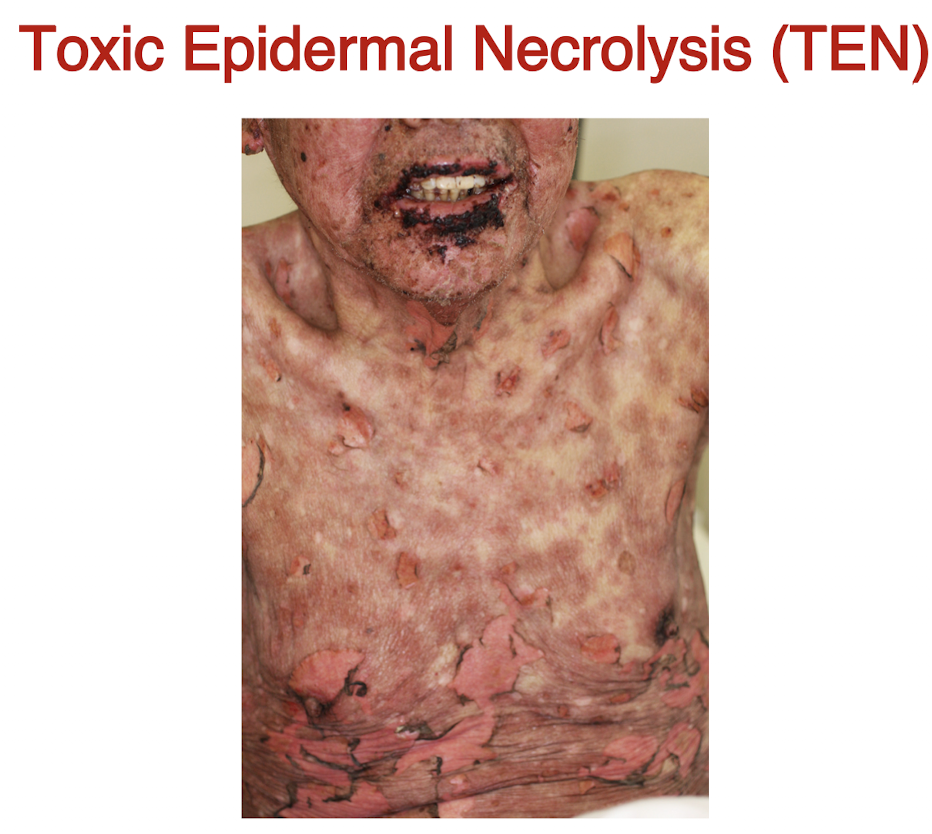
How much body surface area is affected in TEN?
Greater than 30%.
What is the mortality rate associated with TEN?
Approximately 40%.
What are the hallmark findings of TEN?
Diffuse lesions
skin sloughing
lose Na+ and barriers = evaporation
epidermal detachment
extensive tissue loss.
What electrolyte abnormalities may occur in TEN?
Hyperkalemia and hyponatremia.
What hematologic abnormality may occur in TEN?
Elevated hematocrit levels.
Why are fluid and electrolyte imbalances common in TEN?
Massive skin loss leads to fluid shifts similar to severe burns.
fluid shift interstitial (look swollen, less vascularized)
Compare Stevens-Johnson syndrome and toxic epidermal necrolysis.
SJS affects less than 10% of body surface area, whereas TEN affects more than 30%; both involve mucosal damage and skin detachment.
What is systemic lupus erythematosus (SLE)?
A chronic multisystem autoimmune inflammatory disease.
mostly females
butterfly rash
multisystem disease
Which body systems are commonly affected by SLE?
Skin, joints, kidneys, hematologic system, neurologic system, pleura, and pericardium.
What pattern of disease activity is characteristic of SLE?
Alternating periods of exacerbation and remission.
What autoantibodies are produced in SLE?
Antibodies against DNA, erythrocytes, coagulation proteins, lymphocytes, and platelets.
What happens to immune complexes in SLE?
They circulate and deposit in tissues and basement membranes.
Where are immune complexes commonly deposited in SLE?
Kidneys, heart, skin, brain, and joints.
What happens after immune complex deposition?
Complement activation and inflammation occur.