Resp Disorders and Mechanical Ventillation
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
compare anatomy of right and left bronchi
right bronchus is shorter, wider, and more vertical than the left
VQ ratio
what does high indicate?
low?
amt of air that reaches the alveoli divided by amt of blood flow in the capillaries of the lungs
high = ventilation typ normal, but alveolar perfusion is dec or absent (PE, dec CO)
low = pulm circulation is adequate but not enough O2 available to the alveoli for perfusion (airway obstruction, pneumonia, pulm edema)
end tidal CO2 monitoring
normal?
cont. capnography uses infrared light to measure exhaled CO2 at end expiration using a sensor attached to an ETT, tracheostomy tube, or nasal cannula
compare w/ ABGs and use as trend
normal: 30-45 mmHg
low = poor systemic perfusion (caused by hypovolemia, sepsis, dysrhythmias)
values tend to be 2-5 mmHg less than PACO2
normal pH
7.35-7.45
<7.35 = acidosis
>7.45 = alkalosis
PaCO2
regulated by ?
normal?
regulated by the lungs
normal: 35-45 mmHg
<35 = alkalosis
>45 = acidosis
remember: this is an ACID → more CO2 = ACIDosis
HCO3 (bicarbonate)
regulated by ?
normal?
regulated by the kidneys
normal: 22-26 mEq/L
<22 = acidosis
>26 = alkalosis
remember: this is a BASE!!
compensation (2 types)
partial = pH ABNORMAL
complete = pH normal
normal PaO2
80-100 mmHg
common causes of respiratory acidosis
retention of CO2
CNS depression (anesthesia, narcotics, sedatives, drug OD)
neuromuscular disorders
trauma: spine, brain, chest wall
restrictive lung diseases
COPD
acute airway obstruction (late phase)
common causes of resp alkalosis
LOSS of CO2
anxiety, pain, fever (think hyperventilation → expelling lots of CO2)
stimulants
CNS disorders
hypoxia causing lung conditions
pneumonia, atelectasis, asthma (early stage), ARDS, CHF
pulm vascular disease
common causes of metabolic acidosis
GAIN OF ACID
renal failure
DKA
lactic acidosis
drug OD (salicylates, methanol, ethylene glycol)
LOSS OF BASE
diarrhea (ASS-idosis)
renal failure
common causes of metabolic alkalosis
GAIN OF BASE
excess ingestion of antacids
excess administration of Na Bicarb
LOSS OF ACID
vomiting, NG suctioning
low K+ and/or Cl-
diuretics
inc levels of aldosterone
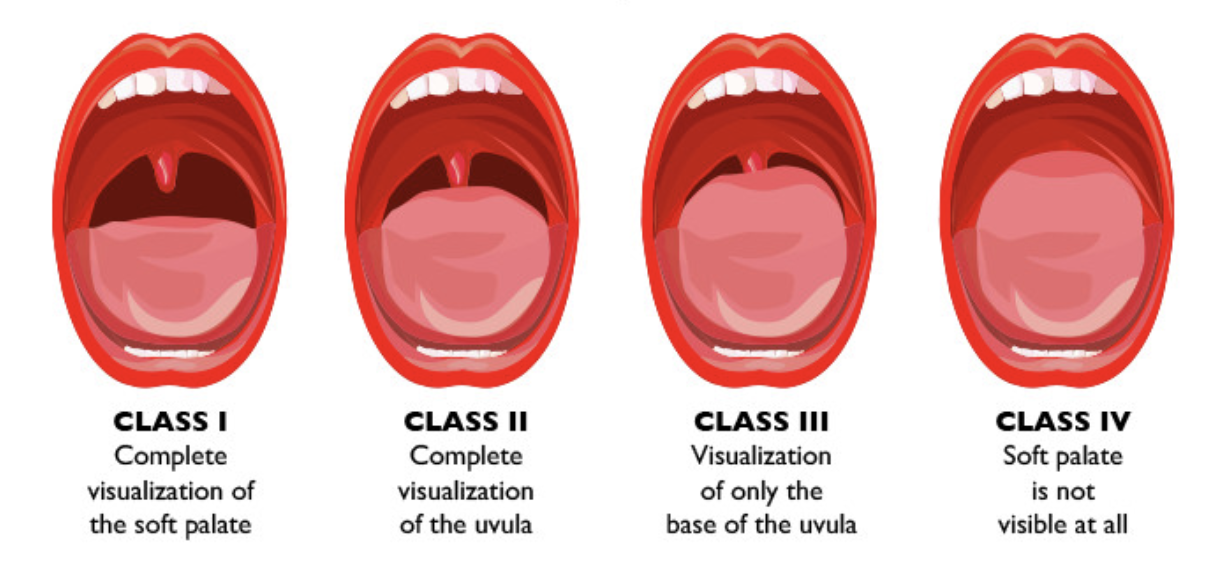
Mallampati Scores
predict intubation difficulty or predict sleep apnea
what structures in throat are visible when pt opens mouth
think “more mouth = more easy”
classes 3 and 4 = difficult intubation or probability of sleep apnea
does an OPA provide oxygen?
NO!! → must ventillate
nurse’s role in intubation
gather supplies
meds available
sedation, neuromuscular blocks, paralytics, fluids, vasopressors,
watch monitor
clinical def of resp failure
PaO2 =
PaCO2 =
pH =
PaO2 = 60 or lower
PaCO2 = 50 or higher
pH = 7.25 or less
positive end expiratory pressure (PEEP)
reduce collapse of alveoli and small airways
more pressure to force alveoli open
inc PEEP dec CO
vent settings: 500/20/60/8
tidal volume / RR / FiO2 / PEEP
synchronized intermittent mandatory ventilation (SIMV) - vent setting
traditional mode
can be assisted, controlled, or supported
delivers mandatory breaths w/ FIXED volume
UNCOMFORTABLE; pt CANNOT trigger
airway pressure release ventilation (APRV)
pt breathes spontaneously
good for ARDS
pressure support (PS) — vent setting
all breaths pt initiated
best for weaning
pressure controlled / assist (PC) — vent setting
assisted or controlled
preset pressure for a set time and rate
pt needs adequate tidal volumes
volume controlled / assist (VC) — vent setting
assisted or controlled
preset tidal volume or rate
noninvasive positive pressure ventilation (NPPV)
2 types
CPAP provides low levels of cont. positive airway pressure throughout the resp cycle
stents open larger airways and PREVENTS ALVEOLI FROM COLLAPSING
BiPAP provides 2 levels of positive airway pressure — 1 cont. pressure during exhalation and 1 during inhalation to assist the ventilatory muscles
CI to non-invasive positive pressure ventilation (NPPV)
actual complete apnea
cardiovascular instability — hypotensive, uncontrolled dysrhythmia, active MI
relative CI: claustrophobia, impaired sense of consciousness, very high aspiration risk, can’t clear secretions, recent gastroesophageal surgery, cranial / facial surgery, facial burns

nursing role for vented pt
location of ETT → verify placement (auscultation and ETCO2 detector)
want bilateral breath sounds
verify settings
ensure emergency equipment available
assess adequacy of CO and oxygenation
monitor for alarms
med management
prevention of AE
ABCEF bundle
pt education
involve pts and family in decision-making
what meds are commonly used for pts who require mechanical ventilation?
bronchodilators
sedation / anxiolytics
neuromuscular blockers / paralytics
analgesics
high pressure vent alarm
aka high peak airway pressure alarm
vent exceeded preset pressure limit → will immediately cycle into expiration and gas flow ceases
MOST COMMON
causes: coughing, attempting to speak, pt / vent asynchrony, kinks, water in circuit, mucous plugs, bronchospasm, pulm edema, pneumothorax, ARDS
low pressure vent alarm
aka low tidal volume alarm
causes: disconnection, air leak, tidal volume too low
high / low rate vent alarms
high = pt agitated, pain , RASS too high
low = oversedated, broken vent
think what causes high vs low RR
ABCDEF protocol
Assess, prevent, and manage pain
Both spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT)
Choice of analgesia and sedation
Delirium — assess, prevent, and manage
Early mobility and exercise
Family engagement and empowerment
mechanical ventilation complications
barotrauma
s&S: high peak airway pressures, dec breath sounds, tracheal shift, hypoxemia, subQ emphysema
ventilator associated pneumonia (VAP)
bundle of practices
HOB at 30 degrees
SBT
PUD & DVT prophylaxis
daily oral care w/ CHG
ETT w/ subglottic suction
early mobility
ETT out of position
unplannned extubation
tracheal damage
damage to oral or nasal mucosa
oxygen toxicity
acid-base imbalance
aspiration
acute respiratory failure
causes?
assessment findings?
most common MICU dx
inability to oxygenate or remove CO2
oxygenation failure
ventilation failure
acute vs chronic
causes?
hypoventlation
intrapulmonary shunting
V/Q mismatch
diffusion defects
low CO
low Hgb
tissue hypoxia
assessment findings?
lethargy, confusion, dysrhythmias, dec peripheral perfusion, tachypnea, bradypnea, tachycardia, HTN
oxygenation failure
PaO2 <60
normal or dec CO2
ventilation failure
hypercapnic resp failure
CO2 >50
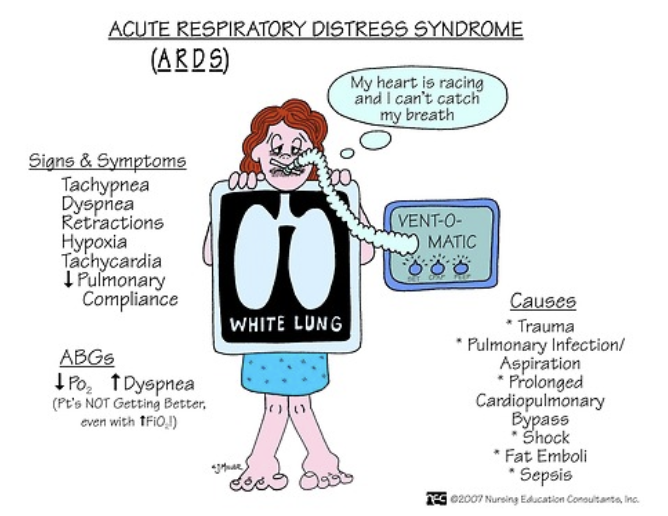
acute resp failure vs ARDS
causes of ARDS?
ARDS = severe ARF
ARDS = dyspnea, tachypnea, dec lung compliance, alveolar infiltrates on CXR
Berlin Criteria
pt must have acute onset w/in 1 wk after some initial clinical insult
bilateral pulmonary opacities (CXR white, opaque) not explained by other conditions
altered PaO2:FiO2 ratio = giving high FiO2 and PaO2 not inc
causes
aspiration, fat embolism, toxic inhalation, drowning, PNA, bypass, OD, sepsis, trauma
ARDS pathophysiology
acute phase = uncontrolled inflammation
proliferative phase = 1-3 wks after onset
fibrotic phase = 2-3 wks after onset
if untreated, leads to multi-organ dysfunction syndrome or multi-organ system failure and death
assessment findings in ARDS
initially:
dyspnea, tachypnea, hypoxemia
anxiety / agitation
initial resp alkalosis
as it progresses:
inc WOB, adventitious breath sounds
worsening CXR
difficulty ventilating due to dec compliance
resp acidosis (body no longer able to compensate)
refractory hypoxemia
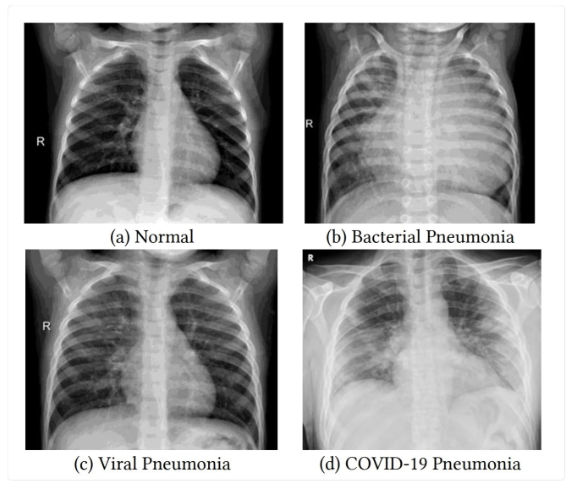
pnemonia (PNA)
lower resp infection that inflames the alveoli in one or both lungs
lots of causes (CAP, HAP, HCAP, VAP, ARF)
can be bacterial, viral, fungal
ventilator acquired PNA
lung infect. that can develop in pts on a vent for more than 48hrs
healthcare associated infect. (HAI)
sx: cough, fever, chills, inc mucous, N, V, SOB
COPD
hallmark signs
chronic and acute exacerbation ABG
tx?
chronic inflamm lung condition that causes obstructed airflow from lungs
exacerbations can lead to ARF and/or ARDS
hallmark signs: dyspnea, chronic cough, excessive sputum production
chronic ABG: compensated resp acidosis, low PaO2
acute exacerbation ABG: uncompensated resp acidosis, lower PaO2
generally tolerate SpO2 >88%
tx:
inhalers (albuterol)
short-term steroids — inhaled (mometasone, budenoside); oral (prednisone, cortisone, methylprednisolone, dexamethasone)
antibiotics
NPPV or intubation
palliative care in late stages
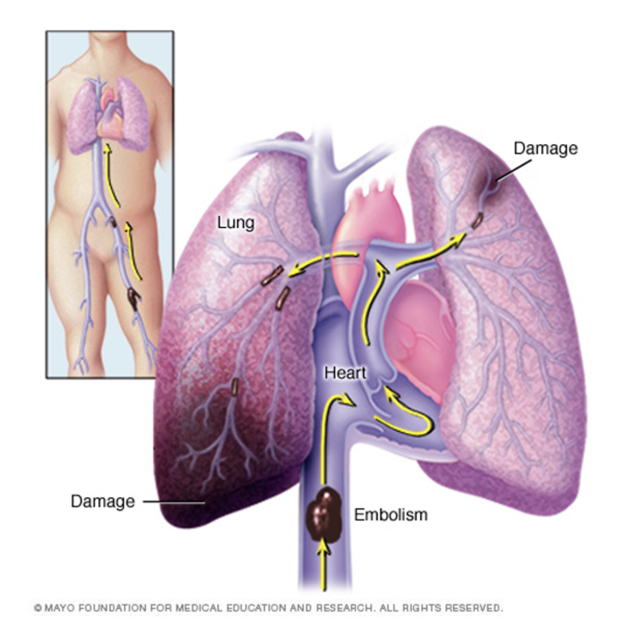
pulmonary embolism
dx?
tx?
blood clot, fat, septic, amniotic fluid in lungs
usually originates from lower extremity DVT
acute (new obstruction that requires immediate tx) vs chronic (older obstruction that has not been resolved; can worsen over time → pulm HTN → R HF )
massive PE → shock, severe pulm HTN, cardiac / resp arrest
mortality rate 30-60%
>50% of pts have NO sx
dx: D dimer (positive = clot that’s beginning to break down), ultrasounds, VQ scan, CT angiogram, pulm angiogram, MRI
tx: anticoagulation, thrombolytics, embolectomy, ventilation → SMALL TIDAL VOLUME AND LOWER PEEP b/c do not want to press emboli to brain