CPR2 - Exam 3 Practice Questions
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms
A 24-year-old patient has a defect that impairs amino acid reabsorption in the proximal tubule. Which of the following is the most likely immediate consequence?
Increased amino acids in the tubular fluid and urine
Which of the following best explains the primary driving force for amino acid reabsorption across apical membrane of proximal tubule cells?
Sodium gradient established by basolateral Na+/K+-ATPase
A 3-year-old female presents with generalized edema shortly after recovery from an upper respiratory infection. Laboratory studies reveal marked albuminuria, as well as hypoalbuminemia and hyperlipidemia. Prior similar episodes responded to adrenal steroid medication. The most likely diagnosis is
minimal change disease.
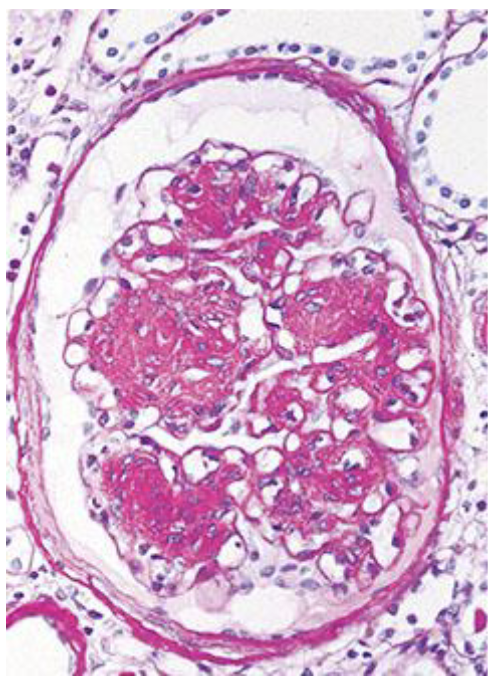
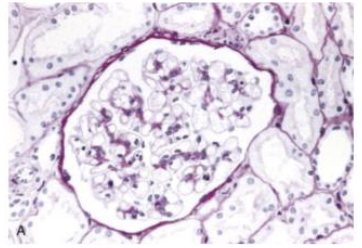
A 50-year-old man with hypertension and nephrotic syndrome undergoes a renal biopsy. The appearance of the biopsy is similar to that shown in the figure. Of the following possible additional laboratory findings, which one is most characteristically associated with this lesion?
Hyperglycemia
At physiologic pH (~7.4), most organic acids (e.g., lactate, pyruvate) exist in which form, and how does this influence their renal handling?
Deprotonated (negatively charged) form; requires transport mechanisms
A patient is given an infusion of parathyroid hormone (PTH). Which of the following changes is most likely to occur in the kidney?
Decreased phosphate reabsorption in the proximal tubule
Which of the following best describes phosphate handling in the proximal tubule under normal conditions?
Majority reabsorbed (~80-95%)
Which nephron segment reabsorbs the largest fraction of filtered calcium?
Proximal tubule
A loop diuretic inhibits Na+-K+-2Cl- transport in the thick ascending limb. What is the most likely effect on calcium handling?
Decreased Ca2+ reabsorption due to loss of lumen-positive potential
Which mechanism is primarily responsible for potassium reabsorption in the proximal tubule?
Paracellular solvent drag and diffusion
Which mechanism in the thick ascending limb is essential for generating the driving force for paracellular cation reabsorption?
K+ recycling into lumen creating a lumen-positive voltage
Where is most of the body’s potassium located?
In the intracellular compartment
In which nephron segment does most amino acid reabsorption occur?
Proximal tubule
How does flow rate in the tubular lumen affect the reabsorption of solutes like calcium?
High flow rate favors secretion and reduces reabsorption
What transporter is most involved in the reabsorption of monocarboxylates like lactate in the proximal tubule?
Na+-monocarboxylate cotransporter
What is the main site of potassium secretion in the nephron?
Distal tubule and collecting duct
Which of the following best describes the mechanism of glucose reabsorption in the proximal tubule?
Glucose is reabsorbed from the lumen via SGLT transporters and exits the cell basolaterally via GLUT transporters
A 21-year-old male presents to the office with a 3-day history of fatigue and darkcolored urine. Physical examination reveals edema. He had a sore throat that lasted 5 days and resolved 2 weeks ago. Osteopathic examination reveals residual evidence of this previous infection with the lingering presence of a unilateral hyoid restriction. Vital signs reveal: Temperature: 37.3ºC (99.1ºF) Blood pressure: 150/90 mmHg Heart rate: 90/min Urinalysis reveals ++blood, - leukocyte esterase, and 1+ protein. RBC casts were present on microscopic examination. Which of the following pathological processes is most likely causing his symptoms?
Acute glomerulonephritis
As tubular fluid passes along a juxtamedullary nephron of a dehydrated person with severe central diabetes insipidus and essentially no antidiuretic hormone, where is the filtrate osmolarity lowest?
Fluid leaving the collecting ducts (urine)
In Goodpasture's syndrome, circulating autoantibodies bind to the noncollagenous-1 (NC1) domain of type IV collagen in the glomerular basement membrane (GBM). Which of the following options corresponds with the definitive diagnosis of this glomerulopathy?
Positive anti-IgG immunofluorescent staining of renal biopsy
Which of the following are typically found in the setting of AKI due to allergic interstitial nephritis?
Eosinophilic cellular infiltrate of the renal parenchyma
A 10-year-old male has a 2-day history of nausea and vomiting accompanied by "red-brown urine." The mother states that 3 weeks ago, he scraped his leg at play. A purulent lesion developed and healed with local treatment. Physical examination reveals a blood pressure of 160/110 mmHg, facial edema, and small eschar was present over the anterior aspect of the left tibia. The urine sediment contained innumerable red cells and waxy casts per high-power field. A percutaneous renal biopsy was performed, and light microscopic examination disclosed that 16 of the 20 glomeruli had exuberant cellular crescents. There was irregular proliferation of mesangial and endothelial cells, with a moderate accumulation of neutrophils within the tufts and fibrinoid necrosis of one arteriole. Which of the following corresponds with the ultrastructure in this patient?
Subepithelial dense deposits shaped like “humps”
A 65-year-old female, a lifelong smoker, was admitted for evaluation of worsening dyspnea and left-sided pleuritic chest pain of several days' duration. One year before admission, the patient underwent needle biopsy of the right kidney for evaluation of hypertension and proteinuria. In this occasion, a rapidly progressive glomerulonephritis was diagnosed. Which of the following morphologic features correspond with this glomerulopathy?
Crescent formation
A 6-year-old male has a 3-day history of nausea and vomiting accompanied by "red-brown" urine. His mother states he had a sore throat 2 weeks ago. Physical examination reveals temperature of 37ºC, arterial blood pressure of 160/100 mmHg, and periorbital edema and pitting edema of the ankles. Urinalysis shows red blood cell casts and dysmorphic red blood cells. Which of the following would best describe this clinical condition?
Nephritic syndrome
A 55-year-old female is admitted with a potassium of 6.0 mEq/L. Her ECG shows no abnormalities. Labs also show a BUN of 60 mg/dL and a Creatinine of 4.5 mg/dL (baseline 1.0). She has had no urine output for 6 hours. Which of the following is the most definitive treatment for her electrolyte abnormality?
Hemodialysis
A 60-year-old female is brought to the ED for confusion. Her serum sodium is found to be 108 mEq/L. She is started on a 3% saline infusion. Twenty-four hours later, her sodium is 126 mEq/L. Three days later, the patient develops dysarthria, dysphagia, and spastic quadriparesis. Which of the following was the most likely cause of her new neurological symptoms?
Central Pontine Myelonosis (CPM)
A patient presents with a serum sodium of 130 mEq/L. Laboratory evaluation reveals a serum osmolality of 290 mOsm/kg (Reference: 285-295 mOsm/kg). Which of the following clinical scenarios is most consistent with this finding?
A patient with Multiple Myeloma and high circulating protein levels
A patient with elevated parathyroid hormone presents with low serum phosphate. Which renal mechanism explains this?
Decreased proximal tubule phosphate reabsorption
A patient with hypocalcemia is given PTH. Which nephron segment primarily mediates the increase in calcium reabsorption?
Distal convoluted tubule
A patient with renal failure develops hyperkalemia. Which nephron segment is primarily responsible for impaired potassium regulation?
Distal nephron (principal cells)
A patient is given aldosterone. Which change promotes potassium secretion?
Increased lumen-negative potential
A researcher wants to measure true GFR. Which substance should be used?
Inulin
A patient’s creatinine clearance is measured. Why does it overestimate GFR?
Tubular secretion of creatinine
A previously healthy 5-year-old boy is brought to the clinic by his parents because of swelling around the eyes and legs that began 3 days ago. The symptoms started about one week after a mild upper respiratory infection. On exam, he has periorbital edema and ascites. Blood pressure is normal. Laboratory studies show serum albumin of 1.8 g/dL, total cholesterol elevated, and urinalysis with 4+ protein but no blood or casts. Complement levels are normal. Kidney biopsy is performed. Which of the following options best matches the underlying pathogenesis and ultrastructural findings of this condition?
T-cell cytokine-mediated podocyte injury causing foot process effacement
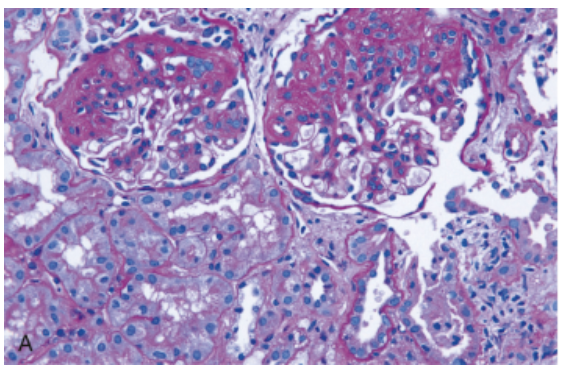
A 38-year-old man presents with progressive lower extremity edema and frothy urine over 3 months. He has a history of poorly controlled HIV infection and past IV drug use. Blood pressure is 150/92 mmHg. Labs show serum creatinine 1.8 mg/dL and urine protein 6 g/day. Kidney biopsy (showed in the picture) shows segmental areas of sclerosis involving some glomeruli with collapse of capillary loops and hyalinosis. Which of the following options best matches the underlying pathogenesis of this condition?
Podocyte loss due to adaptive hyperfiltration injury
A 9-year-old boy is brought to the clinic by his parents because of dark “tea-colored” urine and facial swelling for the past 2 days. Two weeks ago, he had an episode of sore throat with fever that resolved spontaneously without antibiotics. On physical examination, blood pressure is 140/90 mmHg. There is periorbital edema and mild bilateral lower extremity swelling.
• Laboratory studies show:
• Urinalysis: hematuria with RBC casts, mild proteinuria
• Serum creatinine: mildly elevated
• Serum complement (C3): decreased
• A renal biopsy is performed
Which of the following histopathologic findings is most likely seen on renal biopsy?
Subepithelial “humps” with granular immune complex deposition
A 62-year-old man presents with progressive edema and weight gain over 4 months. He has a 40-pack-year smoking history. Workup reveals a newly diagnosed bronchogenic carcinoma. Urinalysis shows heavy proteinuria. Kidney biopsy demonstrates diffuse thickening of the glomerular basement membrane. Silver stain shows spikes between subepithelial deposits. Immunofluorescence reveals granular IgG along capillary loops. Which of the following options represents the pathogenesis?
Subepithelial immune complex deposition with complement activation
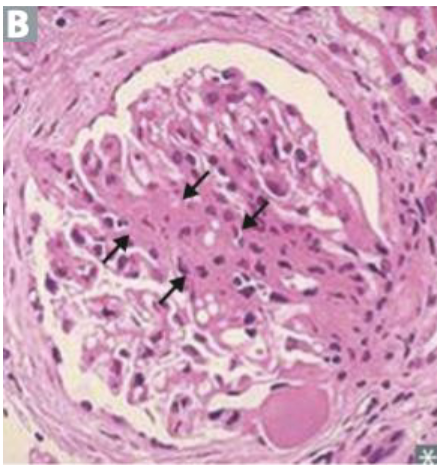
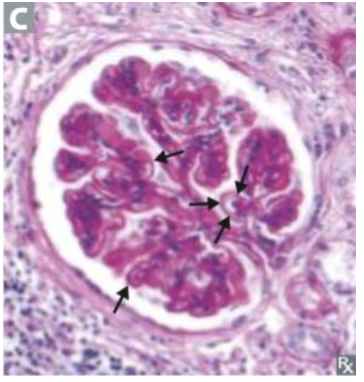
A 55-year-old woman with a 15-year history of poorly controlled type 2 diabetes presents with progressive fatigue and leg swelling. Urinalysis shows persistent albuminuria. Serum creatinine is elevated. Kidney biopsy shows diffuse and nodular glomerulosclerosis with Kimmelstiel-Wilson nodules and thickened basement membranes. Pathogenesis?
Nonenzymatic glycation of proteins forming advanced glycation end products
A 21-year-old man presents with recurrent episodes of gross hematuria that consistently occur 1–2 days after upper respiratory infections. He has no edema or hypertension. Urinalysis shows RBC casts and mild proteinuria. Serum complement levels are normal. Kidney biopsy shows mesangial proliferation with IgA deposition on immunofluorescence. Pathogenesis?
Abnormal IgA1 immune complexes deposited in mesangium with alternative complement activation
A 58-year-old man is treated with high-dose gentamicin for sepsis. Several days later, he develops acute kidney injury. Urinalysis shows granular casts and tubular epithelial cells. Which of the following best describes the mechanism of injury?
Direct toxicity and increased drug concentration in proximal tubular cells
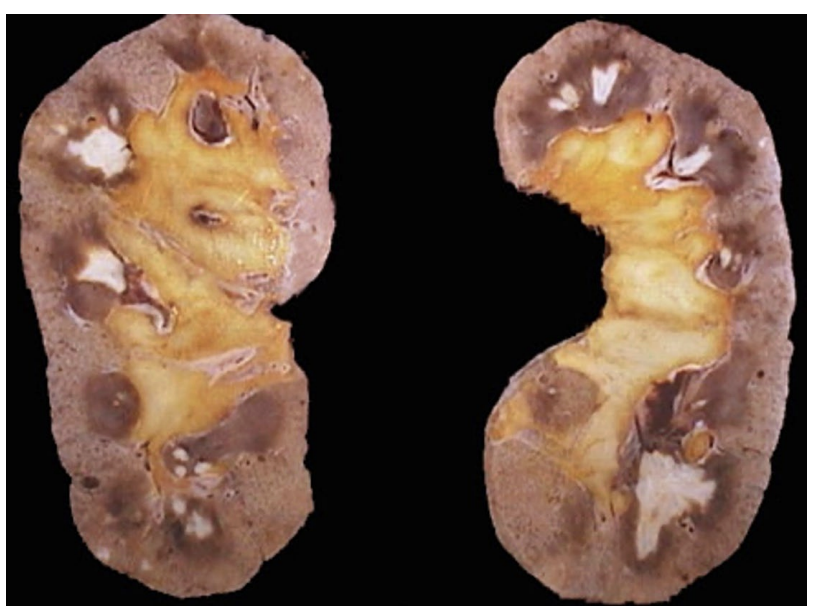
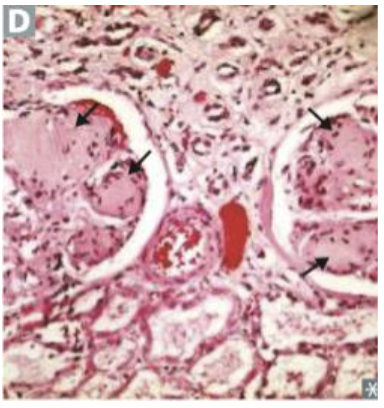
A 55-year-old male with chronic NSAID use develops chronic kidney disease. The attached image shows a gross depiction of his renal pathology. Which of the following mechanisms best explains this NSAID-associated injury?
Inhibition of prostaglandin synthesis leading to reduced papillary blood flow
A 65-year-old man presents with fatigue and back pain. Labs reveal hypercalcemia, anemia, and elevated creatinine. Urinalysis shows proteinuria, but dipstick is negative for albumin. Kidney biopsy reveals glassy, fractured, eosinophilic casts in the tubules surrounded by multinucleated giant cells. What is the most likely diagnosis?
Light chain cast nephropathy
A 55-year-old woman with recurrent urinary tract infection develops a large staghorn calculus. Which of the following organisms is most likely responsible?
Proteus mirabilis
A 17-year-old boy presents with polyuria, polydipsia, and progressive renal insufficiency. Blood pressure is normal. Urinalysis shows minimal proteinuria. Renal ultrasound reveals small kidneys. A biopsy shows interstitial fibrosis and tubular atrophy with small cysts at the corticomedullary junction. Which of the following is the most likely diagnosis?
Nephronophthisis
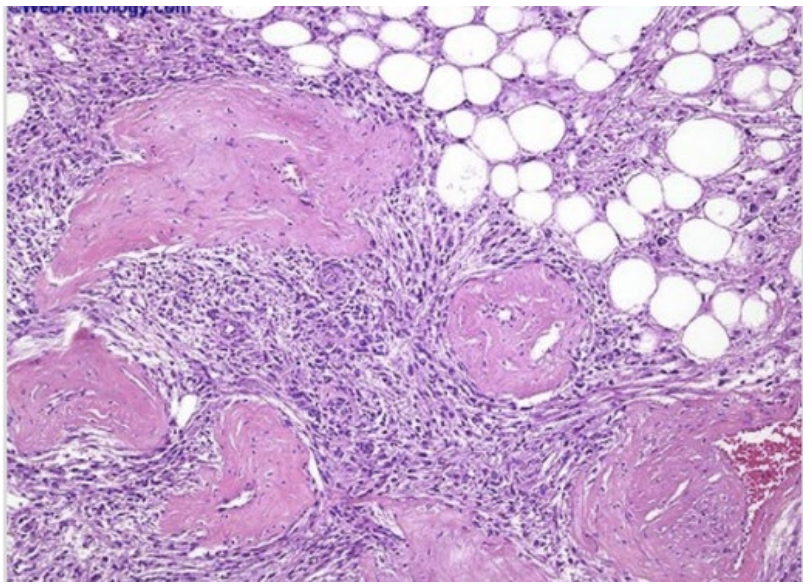
A 35-year-old female is brought to the emergency department in hypovolemic shock, after sudden onset of severe left flank pain. Physical examination reveals a tender, palpable mass in the left upper abdomen. Abdominal CT scan demonstrates a large renal mass and evidence of retroperitoneal hemorrhage.The patient has a long-standing history of seizures since childhood and multiple hypopigmented “ash-leaf” macules on her trunk. Family history is notable for a brother with intellectual disability. On examination, she is also found to have multiple small reddish papules over the nose and cheeks. The patient undergoes emergent nephrectomy. Gross examination reveals a variegated tumor containing adipose tissue, thick-walled blood vessels, and smooth muscle bundles. The microscopic specimen from surgery is shown in the attached photo. This patient is most likely at increased risk for developing which of the following additional findings?
Cardiac rhabdomyomas and subependymal giant cell astrocytoma
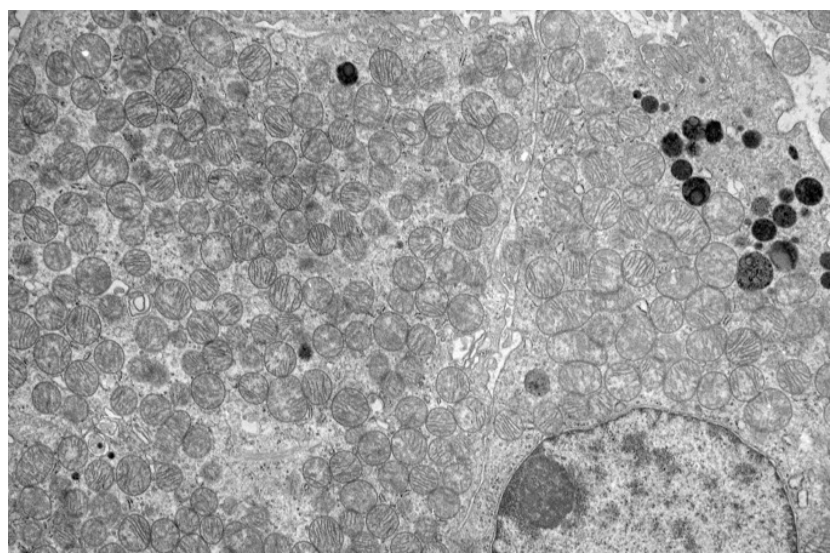
A 50-year-old man undergoes a partial nephrectomy for an incidentally discovered 4 cm renal mass located at the upper pole of the right kidney. Gross examination reveals a well-circumscribed, mahogany-brown tumor with a characteristic central stellate scar. Microscopic examination shows uniform cells arranged in nests and tubules. The tumor cells have abundant granular eosinophilic cytoplasm and small, round, centrally placed nuclei. Special staining is negative for Hale colloidal iron. Electron microscopy of the tumor is shown in the attached image. Which of the following subcellular structures is most likely responsible for the dominant ultrastructural finding in this tumor?
Mitochondria
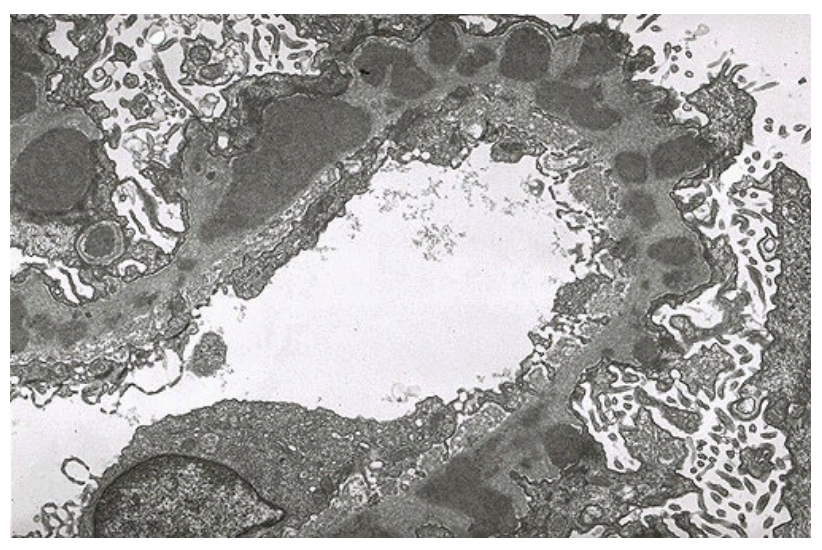
A 32-year-old female is admitted to the hospital because of worsening left flank pain, fever, and new-onset shortness of breath. Two weeks before admission, she developed intermittent sharp pain in the left flank, which progressively worsened and became constant. Over the next several days, she developed nausea and multiple episodes of vomiting. One day before admission, she noted a dry cough and subjective fever. On presentation, her temperature is 39.6°C, blood pressure 102/58 mm Hg, pulse 122/min, respiratory rate 28/min, and oxygen saturation 96% on 3 L nasal cannula. Physical examination reveals diffuse crackles in both lungs and tenderness to palpation of the left lower abdomen. No rash, oral ulcers, or joint abnormalities are present. Laboratory studies show: Serum albumin: 2.8 g/dL Urinalysis: 4+ protein, 3+ blood Urine protein/creatinine ratio: 3.5 White-cell count: 19,000/µL. CT imaging reveals: Filling defects in segmental pulmonary arteries and nearly occlusive thrombus in the left renal vein and partial thrombus in the right renal vein. A renal biopsy is performed and electron microscopy microscopy findings are shown in the figure. The electron microscopy findings most strongly support which of the following mechanisms of glomerular injury?
Subepithelial immune complex deposition with podocyte injury due to in situ antigen–antibody interactions
A 41-year-old male presents with progressive lower-extremity edema and worsening fatigue. Laboratory studies reveal nephrotic-range proteinuria. A renal biopsy is obtained, and the diagnosis is consistent with focal segmental glomerulosclerosis. Further evaluation reveals the following possible contributing factors in different patients with the same histologic pattern:
(1) Circulating permeability factor causing podocyte injury
(2) Chronic heroin use
(3) Reduced nephron mass following unilateral nephrectomy
(4) Infection with human immunodeficiency virus (HIV)
(5) Mutation affecting slit diaphragm proteins (e.g., nephrin, podocin).
Which of the following combinations correctly classifies primary vs secondary causes of this disease?
Primary: 1 Secondary: 2, 3, 4, 5
A 34-year-old male presents to the emergency department with progressive fatigue, shortness of breath, and new onset of coughing up blood over the past week. He reports dark, urine and decreased urine output. Over the past month, he has also experienced intermittent low-grade fevers, malaise, and unintentional weight loss. He denies recent travel, but reports a history of smoking. Physical examination reveals tachycardia, mild respiratory distress, and bilateral inspiratory crackles. No skin rash or joint swelling is noted. Laboratory studies show elevated serum creatinine and blood urea nitrogen. Urinalysis reveals hematuria with dysmorphic red blood cells and red blood cell casts. Chest imaging demonstrates diffuse bilateral alveolar infiltrates consistent with pulmonary hemorrhage. A renal biopsy is performed. Light microscopy shows segmental necrosis of glomeruli with crescent formation. Which of the following mechanisms best explains this patient’s disease?
Anti–glomerular basement membrane antibodies directed against type IV collagen NC1 domain
A 65-year-old female, a lifelong smoker, was admitted for evaluation of worsening dyspnea and left-sided pleuritic chest pain of several days' duration. One year before admission, the patient underwent needle biopsy of the right kidney for evaluation of hypertension and proteinuria. In this occasion, a rapidly progressive glomerulonephritis was diagnosed. Which of the following morphologic features correspond with this glomerulopathy?
Crescent formation
A 4-year-old male is brought to the pediatric clinic by her parents after they noticed progressive abdominal distension over the past several weeks. Physical examination reveals a large, smooth, non-tender abdominal mass that is confined to one side of the abdomen and does not cross the midline. The child is otherwise stable, with no signs of infection or systemic illness. Further evaluation reveals microscopic hematuria. Imaging demonstrates a well-circumscribed renal mass arising from the kidney cortex. The patient undergoes surgical resection. Gross pathology shows a large, tan-white renal mass with areas of hemorrhage and necrosis. Histologic examination demonstrates a triphasic pattern composed of primitive blastemal cells, abortive epithelial tubules, and spindle-shaped stromal elements. Cytogenetic analysis reveals loss-of-function mutation in a tumor suppressor gene involved in early renal and gonadal development. Which of the following genes is most likely mutated in this patient?
WT1
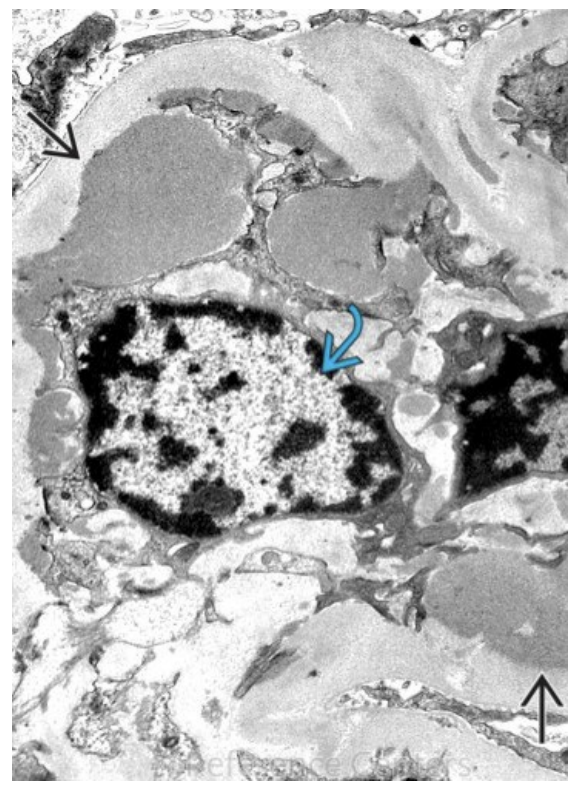
A 19-year-old college student presents to the clinic with recurrent episodes of dark, “tea-colored” urine. He reports that the episodes typically begin within 24–48 hours after an upper respiratory tract infection. Between episodes, he feels well and his urine returns to normal color. He has no edema, no rash, and no joint pain. Blood pressure is 118/76 mmHg. Urinalysis during an episode shows hematuria with red blood cell casts and mild proteinuria. Serum creatinine is normal. Complement levels (C3 and C4) are within normal limits. A renal biopsy is performed. Light microscopy shows mesangial hypercellularity. Immunofluorescence microscopy demonstrates a granular pattern of immune complex deposition within the mesangium. Electron microscopy reveals electrondense deposits located in the mesangial region as shown in the image attached. Which of the following best describes the underlying mechanism of this disease?
Immune complex deposition following abnormal antibody response to mucosal antigen exposure
What is the defining feature between nephritic and nephrotic syndrome?
Urine protein levels 3.5
Which nephrotic syndrome is associated with HIV?
FSGS
Which condition is associated with anti-PLA2R antibodies?
Membranous nephropathy
Which condition causes a loss of antithrombin III to lead to a hypercoagulable state?
Nephrotic syndrome
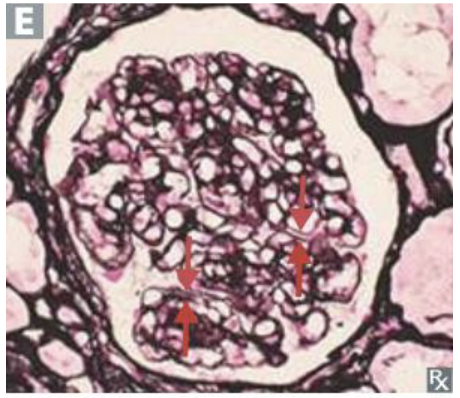
This change of the glomerulus is associated with which condition?
Diabetic nephropathy
A child presents to the office after 2 weeks of an untreated sore throat. What is seen on electron microscopy?
Subepithelial IC humps– infection-related glomerulonephritis
What condition is seen here?
Minimal change disease
Minimal change disease is also known as _________ which can be seen with what special stain?
Lipoid nephrosis, oil red O
A “tram-track” appearance is associated with which nephritic/nephrotic condition?
Membranoproliferative glomerulonephritis
This disease presents with hematuria + hemoptysis... what is the immunofluorescence pattern?
Linear
9yo male with 3+ proteinuria no recent illness, 3+ pitting edema with periorbital & lower extremity swelling. Pathogenesis of this disease?
Cytokine-mediated effacement of podocyte foot processes - minimal change disease
6yo male with blood in urine, progressive hearing loss since birth, bx of kidney shows splitting of basement membrane. What is the inheritance of this disease?
x-linked dominant
Which nephrotic syndrome is most associated with hepatitis B infection?
Membranous nephropathy
Which finding is most characteristic of nephritic syndrome
RBC casts
A patient presents with cola-colored urine after an upper respiratory infection. Diagnosis?
IgA nephropathy
A patient with nephrotic syndrome has frothy urine and edema. Which lab finding is most expected?
Increased lipids
“wire loop” glomerular capillaries on light microscopy are associated with what condition?
Diffuse proliferative glomerulonephritis
What syndrome?
FSGS
This condition is associated with a “spike and dome” appearance on LM.
Membranous
A 42-year-old man is brought to the emergency department by his wife because of a 1-day history of progressive confusion. He recently lost his job. He has a history of chronic alcoholism and has been drinking 14 beers daily for the past week. Before this time, he drank 6 beers daily. He appears lethargic. His vital signs are within normal limits. Serum studies show a sodium level of 111 mEq/L and a potassium level of 3.7 mEq/L. Urgent treatment for this patient's current condition increases his risk for which of the following adverse events?
Osmotic myelinosis
A 47-year-old man with bipolar I disorder and hypertension comes to the physician because of a 2-week history of increased thirst, urinary frequency, and sleep disturbance. He says that he now drinks up to 30 cups of water daily. He has smoked 2 packs of cigarettes daily for the past 20 years. Examination shows decreased skin turgor. Serum studies show a sodium concentration of 149 mEq/L, a potassium concentration of 4.1 mEq/L, and an elevated antidiuretic hormone concentration. His urine osmolality is 121 mOsmol/kg H₂O. Which of the following is the most likely explanation for these findings?
Adverse effect of a medication
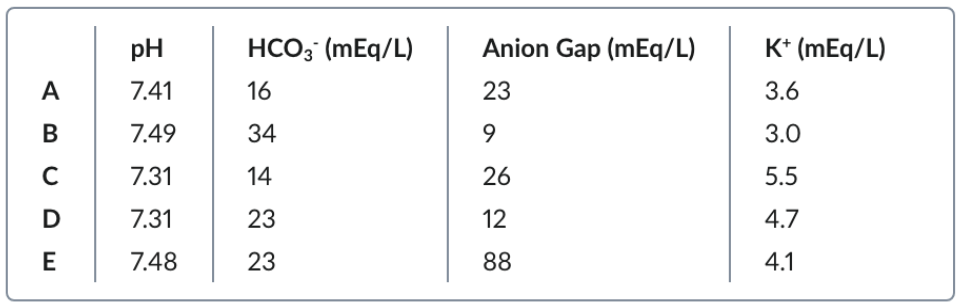
A 21-year-old female college student with a history of anxiety is brought to the physician for evaluation of fatigue for the past 6 months. Over the past year, she has had extreme fluctuations in her weight and has become more distant from her friends. She admits to binge eating and induced vomiting. She appears tired and pale. Her BMI is 18.7 kg/m². Examination shows poor dentition. This patient is most likely to have which of the following sets of serum findings?
B
A 67-year-old man with a history of chronic kidney disease presents to the emergency department with generalized weakness and palpitations. He recently missed multiple dialysis sessions. Vitals: BP 92/60 mmHg, HR 48/min. ECG shows peaked T waves and widening of the QRS complex.
Laboratory studies reveal:
A. K⁺: 7.6 mEq/L
B. Creatinine: 5.8 mg/dL
He is immediately given IV calcium gluconate. Repeat ECG shows improvement in QRS widening, but serum potassium remains elevated. Which of the following is the most appropriate next step in management to rapidly reduce serum potassium levels?
IV insulin with dextrose
A 32-year-old diabetes mellitus is brought to the emergency department by her husband because of a 2-day history of profound fatigue and generalized weakness. One week ago, she dose because of inadequate control of her glucose concentrations. Neurologic examination shows woman with type 1 hyporeflexia. An ECG increased her basal insulin shows T-wave flattening and diffuse ST-segment depression. Which of the following changes are most likely to occur in this patient's kidneys?
Increased activity of the H+/K+ antiporter in a-intercalated cells
Where is the major site of reabsorption of Calcium (bulk), Phosphate, and amino acids?
Proximal tubule
Where is the major site of reabsorption for Calcium (fine-tuning) and magnesium (minor control)?
Distal convoluted tubule
Where is the major site of reabsorption for Magnesium (major)?
Thick ascending limb
Does insulin cause K+ to shift into or out of cells?
Into cells
Do β₂-agonists (e.g., albuterol) cause K+ to shift into or out of cells?
Into cells
Does Aldosterone cause K+ to shift into or out of cells?
Into cells
Does Alkalosis cause K+ to shift into or out of cells?
Into cells
Does hypoosmolality cause K+ to shift into or out of cells?
Into cells
Does Cell lysis (TLS, rhabdo, crush injury) cause K+ to shift into or out of cells?
Out of cells
Do α-adrenergic agonists (e.g., phenylephrine) cause K+ to shift into or out of cells?
Out of cells
Do burns cause K+ to shift into or out of cells?
Out of cells
Does acidosis cause K+ to shift into or out of cells?
Out of cells
Does exercise cause K+ to shift into or out of cells?
Out of cells
Does hyperosmolality cause K+ to shift into or out of cells?
Out of cells
Patient with lymphoma undergoing chemotherapy, K elevated, ↑phosphorus, ↑uric acid. Diagnosis?
Tumor lysis syndrome
Severe muscle pain after intense workout, dark urine, ↑CK, +urine myoglobin, hyperkalemia. Diagnosis?
Rhabdomyolysis
Anemia, jaundice, ↑LDH, ↓haptoglobin, hyperkalemia. Diagnosis?
Hemolytic anemia
Diabetic patient, mild renal insufficiency, hyperkalemia, normal anion gap metabolic acidosis. Diagnosis?
Type 4 renal tubular acidosis (hypoaldosteronism)
Hospitalized patient with rising creatinine, ↓urine output, hyperkalemia. Diagnosis?
Acute kidney injury (AKI)
Patient with uncontrolled diabetes, hyperglycemia, acidemia, hyperkalemia without ↑total body K. Diagnosis?
Metabolic acidosis causing transcellular shift
Chronic diarrhea, K 2.9, (↓HCO₃⁻), urine K low. Diagnosis?
Hypokalemia with Metabolic Acidosis
Recurrent vomiting, K 3.0, (↑HCO₃⁻), urine K low. Diagnosis?
Hypokalemia with Metabolic Alkalosis
Started insulin for DKA, K dropped from 4.2 → 2.8, normal acid-base now. Diagnosis?
Intracellular shift
Persistent hypokalemia despite repletion, Mg 1.5, alcohol use. Diagnosis?
Hypomagnesemia causing renal potassium wasting