SPHG 352 Unit 2 Flashcards (Completed)
1/165
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
166 Terms
How has North Carolina's population distribution changed over time?
1990s: ~50.4% urban; 2019: ~57% urban; Despite this shift, most counties are still rural; Creates a mismatch between population growth and healthcare resource distribution
How did North Carolina address rural health challenges early on?
The NC Institute of Medicine identified rural health issues early; Brought together stakeholders to examine system constraints; Demonstrates that rural disparities are long-standing and well-documented
What happened with Medicaid expansion under the ACA?
Originally required for all states (Jan 1, 2014); 2012 Supreme Court ruling made it optional; 24 states + DC expanded on Jan 1, 2014; Early adopters: Michigan (April 1, 2014), New Hampshire (July 1, 2014); First major nationwide ACA implementation wave
What health disparities exist in rural areas?
Higher rates of heart disease; Higher infant mortality; Small population sizes → less reliable data in some counties; More uninsured adults
What drives rural health disparities?
Access barriers (distance, transportation); Economic instability; Aging populations; Limited infrastructure; These overlapping factors sustain outcome gaps
How does geography impact rural healthcare?
Long travel distances to care; Lower incomes + limited transportation; Contributes to food access issues; Reduces preventive and timely care
Why are there fewer providers in rural areas?
Providers prefer urban areas (higher salaries, resources); Rural areas have: More Medicare/Medicaid patients, Lower reimbursement rates; Makes rural practice less financially attractive
What insurance challenges do rural populations face?
More likely to be uninsured; Often self-employed or work for small employers; Limited access to employer-sponsored insurance; May fall into "coverage gap"; ACA improved coverage (~8 percentage point gain)
Why is Medicare more common in rural areas?
Younger people move to cities; Rural populations are older; Leads to higher Medicare coverage; Lower reimbursement impacts provider supply
What is happening to the rural–urban physician gap in NC?
Gap is widening over time; Population growth worsens per capita disparity; Leads to delays in care and reduced access
Where is healthcare concentrated in NC?
Surplus in areas with medical education & research; Rural areas remain underserved; Uneven distribution worsens disparities
How does medical debt affect NC?
NC has high levels of medical debt compared to other states; Linked to uninsured rates and access barriers
What is happening to rural hospitals?
Closures occurring at alarming rates; Many more at risk; Impacts: Healthcare access, Local economy, Employment
What data shows rural hospital vulnerability?
iVantage (2016): 631 hospitals vulnerable, 355 in high-disparity areas, ~99,000 jobs at risk; UNC study: 8.1% of rural hospitals at high risk of closing; Most affected region: Southern U.S.
Why are rural hospitals closing?
Low reimbursement rates; High uncompensated care; Lack of Medicaid expansion; Declining inpatient demand; High costs (technology, compliance, EMRs, telehealth)
What financial factors strain rural hospitals?
More uninsured & publicly insured patients; Lower Medicare/Medicaid reimbursement; Budget cuts (e.g., sequestration); Low patient volume makes tech investments less viable
How does Medicaid expansion affect hospitals?
University of Michigan study: 50% drop in uninsured care within 6 months; Reduces uncompensated care burden; Improves hospital financial stability; Important partial solution
How is demand shifting in rural healthcare?
Decreased demand for inpatient services; Shift toward outpatient and value-based care; Further reduces hospital revenue
How do modern healthcare systems affect rural hospitals?
EMRs and telehealth are expensive; Require trained staff; Cost-effective in high-volume areas; Not sustainable for low rural patient volumes
Why is policymaking important in public health?
Public health is inherently political; Avoiding policy limits impact; Understanding policymaking is key for effective interventions
What is the overall situation of rural healthcare in North Carolina?
Persistent disparities due to structural issues; Workforce shortages worsening; Hospitals closing or at risk; Insurance gaps remain; Medicaid expansion is a key but incomplete solution
Why is Medicaid central to state health systems?
Covers 2+ million NC residents; Pays for ~50% of births; Covers ~43% of children; Major role in behavioral & developmental health; One of the best case studies for state-level healthcare administration
Why is Medicaid uniquely useful for studying health policy?
Publicly administered program; States have direct control and flexibility; Federal–state shared system; Unlike private insurance (market-driven) or Medicare (federal-only); Shows how politics and economics shape healthcare access and outcomes
How is Medicaid funded and governed?
Federal government pays ~2/3 of costs; States pay ~1/3; Federal gov sets baseline rules; States have flexibility in implementation; Reflects balance between national standards and state autonomy
Who did Medicaid originally cover?
Low-income individuals with categorical eligibility: Pregnant, Disabled, Parents; Did NOT cover all low-income adults; Impoverished adults without these categories were often excluded
What was the Medicaid "coverage gap"?
Income below 138% FPL, but still uninsured; Earned too much for Medicaid; Too little for Marketplace subsidies; Left hundreds of thousands without affordable insurance
What did the ACA aim to do with Medicaid?
Expand Medicaid to all individuals <138% FPL; Intended as nationwide policy; Goal: reduce uninsured population significantly
How did the Supreme Court affect Medicaid expansion?
Ruled federal government cannot force states to expand Medicaid; Reinforced state autonomy in policymaking; Made expansion optional
How did the federal government encourage expansion?
Covered 100% of expansion costs initially (first 3 years); Then reduced to 90% federal / 10% state; Higher match rate for expansion population; Designed to make expansion financially attractive
What additional incentives were offered under ARP?
Extra 5% federal funding increase for first 2 years; NC projected gain: ~$1.2 billion; Encouraged expansion during COVID-19
What political factors influenced NC Medicaid expansion?
Long-standing support from Democratic leaders (e.g., Roy Cooper); Republican support increased over time; Reduced national backlash to ACA; Rural leaders pushed for expansion due to local needs
Why is Medicaid expansion important for rural areas?
Up to 1 in 5 adults uninsured in some rural areas; Helps rural hospitals remain financially stable; Reduces uncompensated care; Improves provider retention
What has been the impact of expansion in NC?
Implemented in 2023; 600,000+ new enrollees; Significant increase in coverage
How does Medicaid expansion affect health outcomes?
Associated with ~12 fewer deaths per 100,000 adults annually; Increased preventive care use; Better adherence to treatment plans
How does Medicaid expansion affect the economy?
Supports labor force participation; Helps small businesses (no need to provide insurance); Reduces burden of uncompensated care; Allows people with disabilities more flexibility to work
What impacts of Medicaid expansion are still being evaluated?
Physical and mental health outcomes; Treatment-seeking behavior; Substance use trends; Long-term economic effects
What are CON laws?
Require state approval before expanding healthcare facilities/services; Designed to control supply of healthcare services; Hospitals must prove a "need" before expansion
Why are CON laws controversial in NC?
Partial repeal tied to Medicaid expansion compromise; May lower prices but risk destabilizing hospitals; Economic and health impacts are uncertain
What are the two main healthcare payment models?
Fee-for-service: paid per service (volume-based); Value-based care: paid for quality and outcomes; Shift aims to improve care and reduce costs
How is NC changing healthcare payments?
Emphasis on prevention and population health; Goal: 70%+ of payments via alternative models; One of the fastest transitions in the U.S.
How do Managed Care Organizations (MCOs) differ from ACOs?
MCOs: Insurance-run, Operate on fixed budgets, Limit provider networks, Control costs; ACOs: Provider-led, Coordinate patient care, Incentivized by quality outcomes, Share savings
What is NC Medicaid Transformation?
Goal: move 80% of beneficiaries to managed care; DHHS contracts with organizations (PHPs); Focus on alternative payment models
What are Advanced Medical Homes?
Primary care providers manage patient groups; Paid via capitation (per member per month); Focus on coordinated, continuous care
What are tailored Medicaid plans?
Designed for high-need populations; Includes: Serious mental illness, Intellectual/developmental disabilities; Integrates physical, behavioral, and pharmacy care
What challenges come with implementing value-based care?
Data sharing across systems; Building infrastructure; Measuring outcomes; Coordinating care across providers
Why is data important in Medicaid reform?
Needed for care management and evaluation; NC requires data sharing laws; Supports better coordination and outcomes
How does Medicaid reform address social factors?
Develops payment strategies for social needs; Improves coordination between clinical and community services; Targets underserved populations
Why is stakeholder engagement important?
Involves providers, hospitals, and clinicians; Reduces provider burden; Aligns public and private systems; Ensures successful implementation
How do employers influence Medicaid reform?
Support payment reform initiatives; Help expand access to care; Influence broader healthcare system changes
What does Medicaid reveal about healthcare systems?
Intersection of policy, economics, and health outcomes; Expansion improves access, health, and finances; Payment reform shapes provider behavior; Ongoing reforms aim to balance cost, quality, and access
How do Medicaid and private insurance differ in payment models?
Medicaid: primarily uses value-based payment systems (focus on quality and outcomes); Private insurance: traditionally uses fee-for-service (pay per service, volume-driven); Reflects broader shift in public programs toward value over volume
What is the historical shift in healthcare payment models?
Traditional system: quantity of care (fee-for-service); Current trend: quality of care (value-based); Goal: improve outcomes while controlling costs
Why are payment models important in health policy?
Influence provider behavior; Affect costs and care quality; Central to health system sustainability; Major focus of state-level reforms like NC Medicaid Transformation
Why is SNAP important in North Carolina?
1.4+ million North Carolinians rely on SNAP; Over 1 million are food insecure; Includes 1 in 6 children; 600,000+ children (<18) and 159,000+ adults (65+) benefit; 4 in 5 SNAP households include a child, senior, or person with disability; 46,000+ veterans receive SNAP; SNAP is a major economic driver, especially in rural areas; Can account for 40–50% of retailer sales; Provides $2.8B in federal funding → $4.2B economic impact
What is H.R. 1 and why is it important?
Signed into law July 4, 2025; Introduces major changes to SNAP eligibility and funding; Impacts state budgets, administration, and access to food assistance; Requires state-level implementation strategies (e.g., NC)
What eligibility changes does H.R. 1 make to SNAP?
Expands work requirements; Eliminates certain exemptions; Restricts non-citizen eligibility; Limits SNAP–LIHEAP connection (utility benefits qualification)
How does H.R. 1 change SNAP funding?
Eliminates future SNAP-Ed funding; Reduces federal administrative match: 50% → 25% (starting Oct 2026); Introduces state cost-sharing for benefits (starting 2027); Cost-share tied to Payment Error Rates (PER)
How are SNAP work requirements changing?
Applies to ABAWDs (18–64); Now includes parents with children >14; Removes exemptions for: Veterans, Homeless individuals, Youth aging out of foster care
Who qualifies for SNAP under new citizenship rules?
Eligible groups: U.S. citizens/nationals, Lawful permanent residents (with exceptions), Cuban/Haitian entrants, Compact of Free Association migrants (Micronesia, Marshall Islands, Palau)
How does H.R. 1 affect SNAP administrative funding?
Federal share drops to 25% (Oct 2026); State + counties pay 75%; Estimated costs: $16M (state), $69M (counties) annually
How will states share SNAP benefit costs?
Begins Oct 2027; Based on Payment Error Rate (PER); Could cost NC up to $420M annually
How does PER determine state cost share?
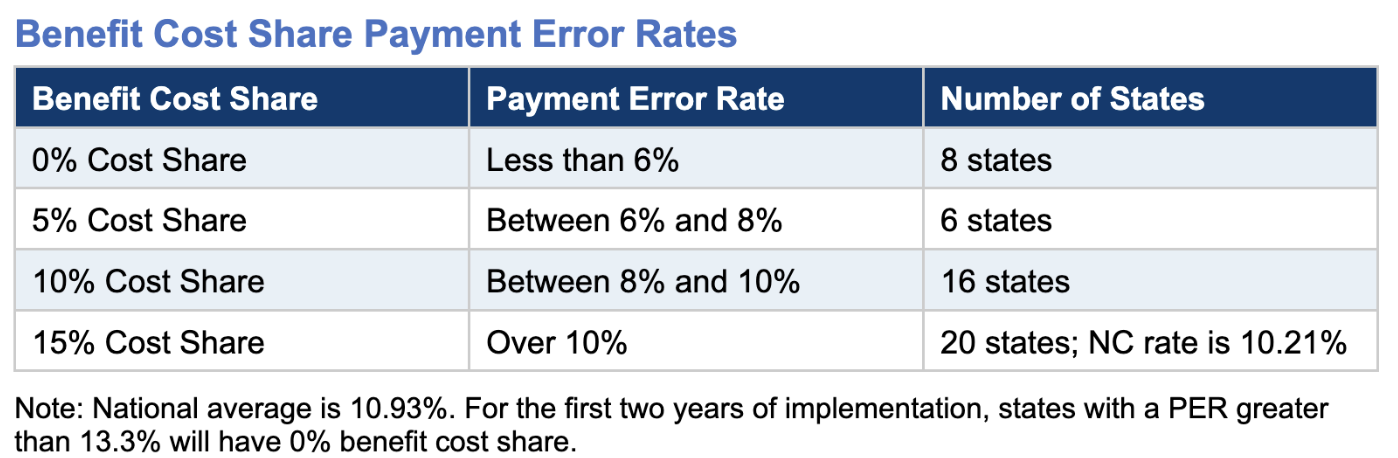
What is a SNAP payment error?
Incorrect benefit amount (over/underpayment); PER = total error value ÷ total benefits; Only counts errors > ±$57 (FFY25) or ±$58 (FFY26); Causes: 55% agency error, 45% client error
What is NC's PER and target?
Preliminary FFY25: 7.01%; Goal: <6% by 2026; Official rate released June 30, 2026
What is the role of NCDHHS in SNAP implementation?
Oversees: Policy & training, Technical assistance, Continuous quality improvement (CQI), Information technology (NC FAST)
How is NCDHHS implementing H.R. 1?
Three workstreams: Policy & Training, Technical Assistance & CQI, Information Technology
What does Policy & Training include?
Update policies (2025–2026); Train county DSS staff (2025–2026); Focus areas: Work requirements, Utility allowance, Non-citizen eligibility, Error reduction; Streamline policies (2026); Rewrite manuals using root cause analysis
What does Technical Assistance & CQI involve?
Identify best practices (top counties); Share lessons across counties; Conduct error analysis; Provide targeted support to high-error counties; Implement continuous improvement systems
What role does IT play in SNAP changes?
Update NC FAST for policy changes; Add tools to reduce errors; Use county feedback to improve system; Develop new tech solutions to reduce workload and PER
What is the NC Healthy Opportunities Pilot (NCHOP)?
Medicaid program addressing social determinants of health; Covers 29 services; Integrates healthcare with social support services
Who qualifies for Healthy Opportunities Pilots?
Must meet ALL: Enrolled in Medicaid managed care, Live in pilot region, Have ≥1 social risk factor, Have ≥1 physical/behavioral health condition, Meet service-specific criteria
What social risk factors qualify someone for NCHOP?
Housing insecurity/homelessness; Food insecurity; Transportation insecurity; Exposure to interpersonal violence
What health conditions qualify for NCHOP?
Adults: multiple chronic conditions; Pregnant women: poor birth outcomes; Children (0–3): NICU history; Children (0–20): adverse childhood experiences
What housing services are provided?
Housing navigation; Move-in support; Utility setup; Home repairs/modifications; Safety inspections; Healthy home goods; Rent/security deposit assistance; Post-hospital housing
What transportation services are offered?
Transport reimbursement; Transportation case management
What interpersonal safety services are included?
Case management; Violence intervention; Parenting programs; Home visiting; Dyadic therapy
What food-related services are offered?
Nutrition case management; Nutrition classes; Diabetes prevention; Produce prescriptions; Food boxes; Prepared meals; Medically tailored meals
What cross-domain services exist?
High-intensity case management; Medical respite care; Legal service connections
What are the main types of public health governance systems?
Centralized: State has primary control over public health decisions; Decentralized: Local governments (counties) have most authority; Shared: Authority divided between state and local levels; Mixed: Combination that varies by function or program
What type of public health governance does North Carolina use?
Largely decentralized system; Local health departments have significant autonomy and decision-making power; State provides guidance, but counties implement many programs independently
How do centralized and decentralized systems differ?
Centralized systems: Less local autonomy, More uniform policies, Often in smaller population states; Decentralized systems (like NC): More local control, Policies vary by county, Greater flexibility
What are the benefits of decentralized public health systems?
Diverse perspectives across counties; More flexibility to address local needs; Less bureaucratic "red tape" at state level; Faster decision-making at county level
What are the responsibilities of local public health agencies?
Follow CDC 10 Essential Public Health Services; Act as official county health authorities; Responsible for implementing public health directives; Must operate to the best of their ability given resources
How do counties monitor health status?
Use EMS data systems (major data source in NC); Systems vary widely: Some counties use Excel spreadsheets, Others use advanced electronic systems; Challenge: Data must be combined across systems; Requires large-scale funding and analysis efforts
How do local agencies investigate health risks?
Example: NC State Fair (Wake County) - Vendor inspections, Crowd health management; Child Fatality Task Force: Investigates every child death, Includes physicians, PH workers, EMS, Mostly volunteer-based, Determines cause and prevention strategies
How do counties inform and educate communities?
Health messaging tailored to local needs; Language access challenges (reduced translation services); Examples: Onslow County - Focus on mental health, substance use, breastfeeding, Tattoo permitting/inspection; Orange County - COVID education in Karen (Burmese) for refugee populations
How do local health departments mobilize partnerships?
Collaborate with communities to solve problems; Engage stakeholders across sectors; Build locally relevant solutions
How do counties develop health-related policies?
Example: Wake County "Sip and Stroll" - Controlled public drinking zones, Community collaboration; Durham County replicated model
What is Durham Vision Zero?
Goal: Zero pedestrian deaths; Uses data to identify high-risk areas; Adjusts infrastructure: Roads, Speed limits, Bike safety measures
What is the Durham HEART program?
Alternative emergency response system; Redirects some 911 calls away from police; Focuses on mental health and non-violent crises; Operates under Durham Community Safety Department
What enforcement roles do counties have?
Enforce sanitation regulations; Conduct inspections; Manage water systems; Can be sued by the state for failure to enforce; Funding cuts can reduce enforcement capacity
How do counties connect people to care?
Example: Durham integrated Health Dept + DSS campus (~2014) - Services include: COVID vaccination sites, WIC program; Barriers: Must physically visit offices; Opportunity: connect people to additional services
What workforce and evaluation roles do local PH agencies have?
Ensure competent workforce; Evaluate service effectiveness and access; Conduct County Health Assessments every 3–5 years; Participate in research
What are CRTs in the HEART program?
Unarmed 3-person teams; Respond to non-violent crises; Staff: Mental health clinician, Peer support specialist, EMT; Provide trauma-informed care; Restrictions: No weapons, No severe intoxication/overdose, No imminent violence risk
What is CCD?
Places mental health clinicians in 911 call centers; Functions: Triage calls, Provide immediate support, De-escalate situations, Divert unnecessary in-person responses, Follow-up with individuals
What is Care Navigation?
Follows up after initial response; Connects individuals to community-based services; Ensures continuity of care
What is Co-Response?
Teams clinician with CIT-trained police officer; Used for higher-risk situations; Handles: Violent crises, Involuntary commitment cases; Goal: safer and more appropriate response
What does the IRT do?
Handles involuntary commitment (IVC) cases; Staffed by EMT + clinician; Determines if commitment criteria met; Provides support during and after hospitalization; If not eligible: creates safety plan + follow-up
What are subversive strategies in public health?
Operate outside formal systems; Challenge traditional approaches; Center community knowledge; Push for change by: Applying pressure, Creating alternatives, Exposing system gaps
Why do subversive public health approaches develop?
Traditional systems are: Too slow, Underfunded, Politically constrained, Not trusted by communities