Resp Exam 2
1/131
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
132 Terms
Caused by physical blockage of the upper airway. Key features include vigorous respiratory effort (chest/abdomen movement) to overcome the blockage and hallmark signs of loud snoring, gasping, and choking sounds
Obstructive Sleep Apnea (OSA)
Primary cause of hypoxemia in all obstructive pulmonary diseases
low VA/Q ratio
Primary cause of sleep-related pulmonary diseases
physical obstruction or lack of respiratory effort
Primary cause of obstructive lung diseases
reduced FEV1/FVC ratio
Primary cause of restrictive lung diseases
Low TLC ratio
An uncommon inherited form of COPD, not caused by smoking. Inhibits neutrophil elastase, and leads to development of emphysema at an early age. Destruction occurs at the base of the lungs, rather than diffusive
Alpha-1 Antitrypsin Deficiency
Long-term continuous O2 therapy is the only Tx clearly shown to improve life expectancy from which condition
COPD
Nitrous oxide is contraindicated in patients with _____ or severe _____
Emphysema; Chronic bronchitis
What do dentists avoid prescribing asthma patients?
NSAIDS (Aspirin)
characterized by air in the pleural space between the chest wall and lung, from a chest wall penetration, rupturing of an area of lung, and appears as a “bleb”
Pneumothorax
what is primary spontaneous pneumothorax
no underlying lung disease, occurs without warning
What is secondary spontaneous pneumothorax
underlying lung disease, emphysematous COPD
Risk of pneumonia is increased from this substance by blunting protective airway reflexes
Alcohol intoxication
An abnormal collection of fluid (>15 cc) in the pleural space; can be caused by pus from infection serious effusion (transudative or exudative), blood (hemothorax), or lymph (chylothorax)
Pleural Effusion
If your patient comes in and you review their health history (like you should always be doing), and you see Rifampin, Isoniazid, Pyrazinamide, Ethambutol, also known as the RIPE Treatment, what does your patient have?
TB
Caused by a neurological failure to signal for respiration. Key features include absent respiratory effort (no chest movement) and hallmark signs of quiet pauses in breathing without snoring or gasping
Central Sleep Apnea (CSA)
A disease of the conducting airways characterized by reversible airflow obstruction. Symptoms like wheezing and dyspnea are variable and often triggered by allergens, cold air, or exercise
Asthma
Characterized by incompletely reversible airflow obstruction, typically caused by cigarette smoking. It includes Chronic Bronchitis (chronic productive cough) and Emphysema (destruction of alveolar walls)
Chronic Obstructive Pulmonary Disease (COPD)
A genetic disorder where a loss of CFTR protein function leads to thick, viscous mucus, causing recurrent infections and airflow obstruction
Cystic Fibrosis (CF)
An intraparenchymal disease involving chronic scarring (fibrosis) of lung tissue. Diagnostic features include "honeycombing" on CT scans, reduced diffusion capacity (DLCO), and "velcro" crackles on examination
Idiopathic Pulmonary Fibrosis (IPF)
Restriction due to external factors like obesity, kyphoscoliosis, or pleural effusions. Unlike IPF, the lungs themselves may be healthy, but the chest wall cannot expand
Chest Wall/Pleural Extraparenchymal Restriction
Restriction caused by muscle weakness (e.g., ALS or diaphragmatic weakness). A key differentiator is a high Residual Volume (RV) because the patient lacks the strength to exhale fully
Neuromuscular Extraparenchymal Restriction
Acute inflammation of the tracheobronchial mucosa, usually viral. It is distinguished by a cough with mucus and is primarily a clinical diagnosis
Acute Bronchitis
Infection of the lung parenchyma (alveoli). Key features include fever, cough, and dyspnea, with diagnosis confirmed by infiltrates on chest imaging
Pneumonia
A bacterial infection spread via airborne transmission
Tuberculosis (TB)
Elevated blood pressure in the pulmonary arteries. Key features include exertional dyspnea, fatigue, and syncope. Right heart catheterization is required for a definitive diagnosis
Pulmonary Hypertension (PH)
A blood clot that travels to the pulmonary artery, often from a deep vein thrombosis (DVT). It is characterized by acute onset dyspnea and pleuritic chest pain and is typically diagnosed via CT Angiogram
Pulmonary Embolism (PE)
Fluid accumulation in the alveoli. It can be cardiogenic (due to high heart pressure) or non-cardiogenic (e.g., high altitude)
Pulmonary Edema
Chronic lung diseases caused by inhaling inorganic dusts, such as Asbestosis, Silicosis, or Coal Dust. These typically have a long latency period (years) before symptoms appear
Pneumoconiosis
Acute lung injury linked to vaping, often involving Vitamin E Acetate in THC-containing products, causing high morbidity in young adults
Vaping-Associated Lung Injury (EVALI)
The individual is infected with viable TB, but the immune system has "walled off" the bacteria. These patients are asymptomatic and not contagious, though the disease can progress to an active state if they become immunocompromised
Latent TB
This is a symptomatic pulmonary infection where radiographic or microbiologic evidence of the bacteria is present. Patients with active TB are contagious and typically present with a chronic cough, fever, fatigue, and weight loss
Active TB
This occurs when a patient develops the symptoms and signs of Active TB within the first two years of being infected
Primary TB
This is active TB disease that develops two or more years after the initial infection. It is common in the lungs and can present with night sweats and hemoptysis (coughing up blood)
Reactivation TB
This describes an individual who was previously exposed to TB but has either naturally cleared the infection or has been successfully cured through antimicrobial therapy
Eliminated TB
What is important to remember about testing for active TB infections
Neither the skin test nor the Quantiferon blood test should be used, as they are not designed to identify active disease
What condition does a patient’s low DLCO suggest
emphysema
Why would a pt’s TLC and RV be high?
air gets stuck behind in airway collapses due to emphysema, which increases the Residual Volume (RV) and pushes the Total Lung Capacity (TLC) higher than normal.
Define “air trapping”
The inability to fully exhale the inspired air.
How does "Hyperinflation" make it harder to take a breath
It flattens the diaphragm
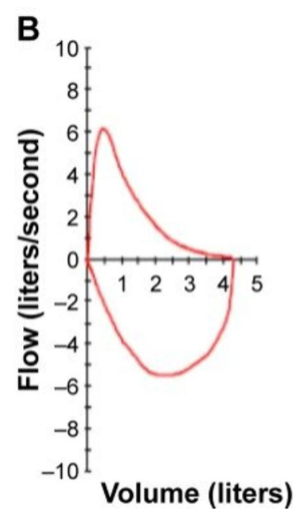
Explain what is occurring in the Flow-volume loop
The expiratory limb (top) shows a classic "Scooped-out" appearance because airflow drops off rapidly as the airways collapse, due to emphysema
How might a young woman with asthma differ from a patient with emphysema?
Reversibility and Variability. An asthmatic patient would have a similar "scooped" loop during an attack, but her PFTs would return to normal after using a bronchodilator Her DLCO would be normal, as her alveolar membranes are not destroyed like a COPD patient's
Explain the 95% to 84% drop in Respiratory Volume using the "Safety Margin" of capillary transit time
At rest, blood spends 0.75 seconds in the capillary. Even with a thick membrane, the oxygen has enough time to "equilibrate." When the patient walks, their heart rate increases and blood speeds up, spending only 0.25 seconds in the capillary. In a fibrotic lung, 0.25s is not enough time to cross the thick barrier, so the blood leaves the lung without enough oxygen.
Explain a “stiff” lung
Low Compliance. It takes a massive amount of pressure to achieve a small change in volume. The pressure-volume curve is shifted down and to the right.
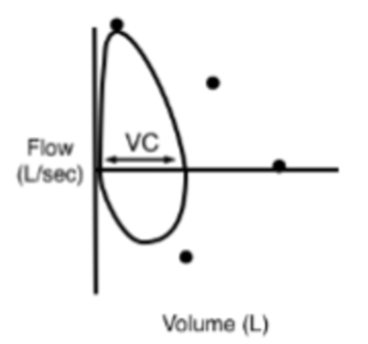
Describe the pressure-volume loop and what it is most often associated with.
A "Witch’s Hat" appearance. The loop is shifted to the Right (low volumes). It is very narrow because the total volume (FVC) is low, but it is tall because the stiff tissue pulls the airways
open, allowing for high flow rates relative to the volume. Can happen in pts with pulmonary fibrosis and neuromuscular weakness
Why would DLCO be normal in a pt with neuromuscular weakness, such as ALS
the lung tissue and gas-exchange membrane are healthy. The low TLC is caused by the skeletal muscles being too weak to pull the chest open, diffusion (DLCO) remains normal.
Why is a patient with neuromuscular weakness at a high risk for aspiration pneumonia?
A cough is a "forced exhalation." It requires strong abdominal and intercostal muscle contraction to blast air out. ALS patients lack this strength. If they aspirate water or a crown fragment, they physically cannot "cough it up," allowing the material to sit in the lung and cause infection
How should patients with neuromuscular weakness be positioned to receive dental treatment?
Semi-upright (45 degrees). Lying flat allows the weight of the abdominal organs to push up against the already weak diaphragm, which could lead to immediate respiratory failure in the chair.
Why would an obese patient (I’m talking an absolute beast) be at risk for deep sedation
The patient is already in a state of chronic hypoventilation. Sedatives (like opioids) suppress the remaining "respiratory drive." If you give this patient a sedative, their breathing will slow further, their PaCO2 will rise to toxic levels (CO2 Narcosis).
During NREM sleep, breathing is primarily controlled by the __________ system.
Metabolic (Chemical) system
During REM sleep, which respiratory muscle remains active while others undergo atonia?
The Diaphragm.
In Obstructive Sleep Apnea (OSA), respiratory effort is __________.
Present. The patient is physically struggling to overcome a blocked airway.
In Central Sleep Apnea (CSA), respiratory effort is __________ (Present/Absent).
Absent. The brainstem temporarily fails to send the signal to the diaphragm to move.
What is the Primary Infection stage of TB?
Initial exposure and immune response.
What is the Latent TB infection stage?
Bacteria are walled off by the immune system (granulomas). Asymptomatic and not contagious.
What is the Active/Reactivation TB infection stage?
The bacteria overcome the immune system, leading to tissue destruction and systemic symptoms.
HIGHLY contagious.
How do we test for latent TB?
PPD (skin test) or IGRA (blood test).
How do we evaluate for active TB?
A combination of clinical symptoms (cough >3 weeks, weight loss), Chest X-ray (looking for cavitary lesions), and sputum testing (AFB smear, PCR, and culture).
What is the Screening tool used on patient who grind?
The STOP-Bang questionnaire.
BMI > 35, Hypertension, Neck circumference > 17 inches, and Male gender are all risk factors for what condition?
Obstructive Sleep Apnea
Clenching/grinding is thought to be a subconscious neuromuscular effort to move the mandible forward and stabilize the airway to trigger a "micro-arousal" so the patient can resume breathing in WHAT CONDITION?
OSA
What is the dental management for OSA?
MADs, pulls the tongue forward to increase retroglossal space,
preventing airway collapse.
Side effects of MADs
Hypersalivation and temporary tooth tenderness/jaw soreness upon waking
In patients with obstructive or restrictive disease, baseline oxygen is already low. This is because
During an apnea event, they have no "oxygen reserve," causing their saturation to crash much faster and deeper than a healthy patient
You are observing a patient in a sleep study and they are not moving during the apnea. What condition might this be, and why
The patient is "quiet" because the pump isn't being told to move.
Differences between OSA and CSA
OSA is a physical block (snoring/effort);
CSA is a neurological failure (quiet/no effort)
CSA is often associated with Heart Failure (Cheyne-Stokes respiration)
why are opioids not recommended for patients with CSA?
Opioids are potent respiratory depressants. They blunt the metabolic drive (sensitivity to CO2). Since the metabolic drive is the only system keeping an apnea patient breathing during sleep, suppressing it can lead to dangerous respiratory complications.
_______ involves the conducting airways (bronchi). ______ involves the gas-exchange units (alveoli/parenchyma) and typically presents with a higher fever and more severe systemic illness.
bronchitis; pneumonia
Are antibiotics necessary in acute bronchitis cases?
NO, over 90% of them are viral
Why are viral infections cause for respiratory concern?
paralyze the cilia and prevent clearing of mucus and trapped pathogen in the mucociliary escalator
If you suspect a patient has pneumonia, what are your next steps?
Referral for chest Xray and immediate medical attention
combo of subacute cough (>3 weeks), hemoptysis (blood
in sputum), weight loss, and night sweats
Reactivation (Active) TB
You are at the front desk and patient comes in with what you suspect is active TB. What do you do next?
front desk should provide the pt with a surgical mask to contain the source, isolate, and call the DOH. Pt can return once medical clearance is granted (negative sputum cultures)
How is TB spread
Droplet nuclei (1-5 microns) that stay suspended in the air for hours. Standard masks only stop large "droplets" that fall. N95 respirators and negative pressure rooms are required
A patient with TB symptoms tells you they received the BCG test for TB but their doctor told them “not to worry about it.” Why should you still worry about it?
BCG does not provide 100% protection. It often causes a false positive PPD (skin test)
What test do you give a patient with TB symptoms who has received the BCG vaccine?
The IGRA blood test - it does not cross-react with the BCG vaccine
The patient describes his chest pain as "sharp and stabbing" specifically during deep inhalation. Which anatomical structure is responsible for transmitting this sensory pain signal?
The Parietal Pleura
If a thoracentesis (fluid sampling) was performed and the fluid was found to have a high protein count and high LDH levels, how would this effusion be classified, and what is the most likely underlying cause in this specific patient?
Exudative; Local inflammation and infection from pneumonia.
"Pleuritic Chest Pain" clues you into which types of pleural processes?
It suggests processes that irritate or involve the parietal pleura. This includes pneumonia (parapneumonic effusion), pleurisy (inflammation), pulmonary embolism (if it causes a small peripheral infarction), or an empyema.
What is transudate look like
Clear, protein-poor fluid (like "water") because the capillaries
are intact but pressure is high.
What does Exudate look like
Cloudy and rich in protein and inflammatory cells because the capillaries are "leaky" or damaged by inflammation.
What impact might a large pleural effusion have on the mechanical function of the respiratory system?
It creates a restrictive ventilatory defect. The fluid occupies space in the thoracic cavity, physically compressing the lung and significantly decreasing lung compliance (stiffening the system), it also pushes on the diaphragm, making it inefficient.
In a patient taking an anticoagulant like apixaban, what is the most likely classification of a pleural collection following blunt chest trauma?
Hemothorax (accumulation of blood).
How does a large hemothorax affect the pulmonary function of the affected lung?
It creates a restrictive defect by physically preventing the lung from expanding.
What are the benefits of anticoagulation of a patient on apixaban?
The benefit is the prevention of recurrent, life-threatening pulmonary emboli.
What are the risks of anticoagulation of a patient on apixaban?
The risk is a significantly increased predisposition for severe hemorrhage, even after minor trauma (like a fall).
How would you distinguish the "dullness to percussion" found in a patient from the expected auscultation on a patient with a pneumothorax?
Fluid (blood/hemothorax) is dense and produces dullness (a thud). Air (pneumothorax) is less dense than tissue and produces hyper-resonance (a hollow, drum-like sound).
A patient is appearing pale (anemic). Why might a hemothorax lead to systemic symptoms like pallor and hypotension, whereas a simple transudative effusion typically does not?
A hemothorax involves the loss of circulating blood volume into a non-functional space. This leads to anemia (pallor) and hypovolemic shock (hypotension). A transudative effusion is just a leak of plasma-like fluid, which does not deplete the red cell count or total blood volume as acutely.
In a patient with a hemothorax, what is the course of tx for you as a dentist?
urgent drainage (chest tube) and stabilization. Do not proceed with dental procedure; the patient is hemodynamically unstable and requires emergency medical intervention.
A pulmonary embolism creates a specific type of V/Q mismatching. What describes the physiological change in the affected lung area
Increased Physiologic Dead Space (Ventilation without Perfusion).
What is the most significant clinical concern for a dentist performing an extraction on a patient taking apixaban for a recent PE?
Risk of prolonged and difficult-to-control post-operative bleeding.
What are in Virchow’s triad?
Stasis, vessel injury, hypercoaguability
In the context of a PE, why would a patient experience a "syncopal event" (fainting)?
A large PE increases Pulmonary Vascular Resistance (PVR). The Right Ventricle (RV) fails against this high afterload, causing the septum to bow and prevent the Left Ventricle from filling. This causes a sudden drop in Cardiac Output, leading to cerebral hypoperfusion and fainting.
As a dentist, if your patient is experiencing a syncopal event, should you proceed with your procedure? Should you ask your patient to stop their anticoagulant?
Consult with their physician. Simple Exts can be done with local hemostatic measures. Don’t ask them to stop any anticoagulants without physician approval
Based on the mPAP of 26 mmHg, a pt meets the clinical criteria for which condition?
Pulmonary Hypertension
What is the clinical term for right-sided heart failure that results specifically from chronic high pressure in the pulmonary vasculature?
Cor Pulmonale
Explain "Hypoxic Pulmonary Vasoconstriction." How does it become a problem in COPD?
HPV is normally local and helpful (diverts blood to good alveoli). In COPD, the hypoxia is global (throughout the lungs). This causes widespread vasoconstriction, which raises total PVR and creates a permanent, high-pressure burden for the Right Ventricle.
What is Group 1 Pulmonary Hypertension
Pulmonary Arterial Hypertension
What is Group 2 Pulmonary Hypertension
Left Heart Disease
What is Group 3 Pulmonary Hypertension
Lung Disease/Hypoxia