Ischaemic Heart Disease Pharmacology
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
What are the 2 categories ischaemic heart disease is split into?
Chronic arterial disease and acute coronary syndromes
What is an example of a chronic arterial disease?
Stable angina
What are examples of acute coronary syndromes?
Unstable angina, NSTEMI, STEMI
What does a NSTEMI stand for?
Non ST elevated myocardial infarction
What does a STEMI stand for?
ST-elevated myocardial infarction
What is the term to describe a reduced blood flow to a region of the heart, mostly caused by atherosclerosis?
Ischaemic heart disease
What is the term to describe a partial vessel block in the heart?
Stable angina
When does angina pain occur for stable angina?
Upon exertion - o2 demand exceeds o2 supply due to the reduced BF, pain radiates to arm and jaw and resolves upon rest
What is the term to describe pain resolving upon rest in angina, where there is no heart cell death?
Transient ischaemia
What is the term to describe a lack of oxygen causing pain even when at rest, caused by a plaque rupture that causes platelet aggregation and ultimately thrombus formation but no cardiac tissue damage?
Unstable angina
What should you do for unstable angina if the thrombus has lysed?
Recover blood supply
What is the term to describe where the coronary artery isn’t fully blocked so some tissue perfusion remains, relatively small area of tissue death?
NSTEMI
What is the term to describe complete occlusion of a coronary artery leading to a large area of tissue death?
STEMI
What is the colloquial term for myocardial infarction?
Heart attack
What is the term to describe a plaque of lipid, fibres and cells, causing reduced blood flow and vasospasm that occludes arteries?
Atherosclerosis
What is the therapeutic goal in stable angina?
Improve coronary BF, reduce cardiac oxygen demand
What is the therapeutic goal in NSTEMI/unstable angina?
Prevent further thrombus formation and progression to STEMI, symptomatic relief
What are the therapeutic goals in STEMI?
Re-establish perfusion, symptomatic relief
What do organic nitrates produce?
NO
What effects does NO have?
Arterial dilation - reduces resistance and workload
Venous dilation - decreases venous return, preload and increases blood supply to the heart as less pressure on coronary arteries
What is the main issue with organic nitrate use for stable angina?
Treats symptoms, not the cause!
How do nitrates work?
Made from bradykinin, diffuse into vascular smooth muscle, cGMP activates PKG which causes relaxation of smooth muscle
What action does angiotensin 2 have on receptors?
Causes contraction of smooth muscle
What medicinal forms is glyceryl trinitrate usually formulated in to avoid first pass metabolism?
Sublingual spray, buccal, transdermal, IV
What are the slower onset nitrates?
Isosorbide mononitrate and isosorbide dinitrate
What are the ADRs of nitrates?
Hypotension, dizziness, headache and flushing, tolerance
Why do nitrates cause hypotension?
Decreased venous return decreases cardiac output so less blood to brain
How can you avoid nitrate tolerance?
Avoid with nitrate low period - only administer once a day, if TD patch remove overnight
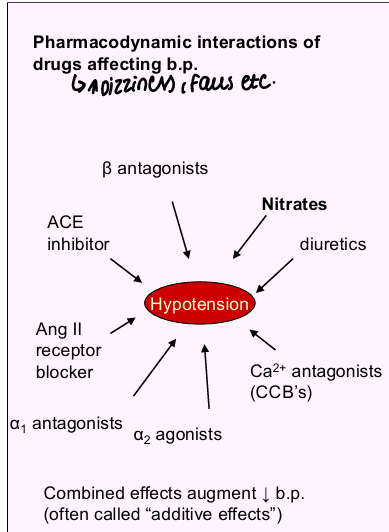
What are some common drug interactions with nitrates?
Drugs causing hypotensive effect e.g., diuretics, other drugs causing vasodilation, PDE inhibitors, can increase heparin excretion
What are the cautions for nitrates?
Avoid in pregnancy due to affecting placental BF
What are the contraindications for nitrates?
Hypotension, hypovolaemia, nitrate hypersensitivity
Why should nitrates and PDE inhibitors not be used together?
Both produce vasodilation and significantly decrease BP - PDE5 inhibitors e.g., sildenafil potentiates cGMP
How does the angiotensin and a1 adrenergic receptor cause contraction?
Both bind intracellular phosphate
IP3 produced
Releases calcium from IP3 receptor
Ca activates CAM kinase
CAM kinase activates MLCK
MLCK phosphorylates myosin light chain
Phosphorylation causes contraction
What receptors in vascular smooth muscle cause contraction?
Angiotensin and a1 adrenergic receptor
What receptors cause relaxation in vascular smooth muscle?
B2 adrenergic receptor
How does b2 adrenergic receptors cause relaxation?
Produces cAMP
Prevents phosphorylation of MLCK via protein kinase A
Doesn’t allow contraction to occur
What structure in smooth muscle allows calcium to enter the cell, into the stores and waiting at the pump to bring about the contraction?
Ca2+ channel
Where is nitric oxide derived from?
Endothelium
How does nitric oxide work?
Activates guanylate cyclase, which makes cGMP and makes protein kinase G to cause relaxation
What are the roes of protein kinase G?
Activates myosin light chain phosphatase which reverse conversion of the phosphorylated myosin light chain and causes relaxation.
Stimulates calcium pump which usually pumps calcium into stores - reduces calcium amount so less able to drive phosphorylation
Phosphorylates K channel - allowing potassium efflux causes hyperpolarisation, which closes calcium channel and reduces influx
What blood vessel does nitric oxide mostly have its effect on?
Veins
What is the MOA of beta blockers/beta antagonists?
Decreas rate and force of heart contraction and BP - negative chronotrope and inotropic effects
What is the impact of beta blockers reducing heart rate?
Reduces myocardial o2 demand
What adrenergic drugs cause vasodilation?
b2 partial agonists and a1 antagonists
What are examples of cardioselective beta blockers, selective for b1?
Atenolol, bisoprolol, metoprolol
What are some examples of non-selective beta blockers?
Propranolol, sotalol
Aside from adrenergic receptors, what else does sotalol inhibit?
K+ Channels
What are some examples of partial agonists that still allow some antagonism of b1 to inhibit tachycardia during exercise and mildly increase HR at rest, useful for bradycardia?
Acebutolol, pindolol
Why may beta blockers NOT be used in poorly controlled heart failure?
May reduce the heart rate and contraction too much and make it worse
Why are beta antagonists contraindicated in asthma?
Beta antagonists blocks airway relaxation of b2 adrenoceptor and can exacerbate breathlessness
What are some ADRs of beta blockers?
Bronchoconstriction - less with cardioselective
Bradycardia and reduced cardiac contractility - can lead to cold hands and feet, fatigue, decreased exercise capacity
Erectile dysfunction
Sleep disturbances, lucid dreams
What beta blockers is less likely to cause sleep disturbances as it has a poor CNS penetration?
Atenolol
What are cautions and contraindications for beta blockers?
Avoid in pregnancy unless essential, avoid suddenly stopping therapy, can mask hypoglycaemia signs, caution in diabetes, reduced metabolism in those with renal/hepatic impairment
CI in asthma, bradycardia, hypotension
What is the risk of using beta blockers with verapamil?
Asystole risk!
How do beta blockers block signs of hypoglycaemia?
Hypoglycameia usually activates sympathetic nervous system to restore blood glucose via b2 but b1 antagonist masks tachycardia and inhibits homeostatic response
What are examples of dihydropyridine calcium channel blockers?
Nifedipine, amlodipine, felodipine, lercanidipine
What effects do dihydropyridine calcium channel blockers have?
Vascular effects
What are examples of non-dihydropyridine calcium channel blockers?
Verapamil, diltiazem
What effects do non-dihydropyridine calcium channel blockers have?
Vascular and cardiac effects
What are some examples of vascular effects that calcium channel blockers bring about?
Arteriolar dilation, lower resistance/BP, lower workload, lower o2 demand, coronary artery dilation, reduced vasospasm and improves o2 supply
What are examples of cardiac effects that non-dihydropyridine calcium channel blockers bring about?
Reduced rate and cardiac contractility, lower workload, lower o2 demand
How do calcium channel blockers work in smooth muscle and cardiac tissue?
Inhibits vascular smooth muscle contraction which reduces afterload, inhibits cardiac myocyte contraction which reduces workload
How do calcium channel blockers work in cardiac tissue?
Inhibits rate and conduction velocity in AV node - phase 0 depends on calcium influx and blocks conduction to regulate contractility and reduce workload
What are some common ADRs of dihydropyridine calcium channel blockers?
Vasodilation related effects e.g., flushing, headache, oedema, can cause reflex tachycardia/palpitations and increased contractility
What is a way of overcoming the effects of dihydropyridines causing increased contractility which may increase risks of MI?
Modified release formulations used
What are the cautions/contraindications of dihydropyridines?
Can be referred in heart failure as they don’t reduce cardiac contractility, avoid in pregnancy and breastfeeding, not to be used during unstable angina/1 month after MI as vasodilation can worsen
What are the interactions of dihydropyridine CCBs?
Augment effect of other drugs that lower BP, avoid grapefruit juice, increases plasma ciclosporin and digoxin concentrations
What are the ADRs of diltiazem?
Bradycardia - inhibits cardiac AV node conduction and SA node threshold, teratogenic
What are the cautions and contraindications of diltiazem?
Reduces dose in hepatic and renal failure, CI in breastfeeding, pregnancy, patients with heart failure shouldn’t use as it is negatively inotropic, not to be used in patients with AV block
What are some interactions with diltiazem?
NOT to be used with beta blockers as cardiac output can be significantly reduced, increase effect of other drugs that lower BP/reduced heart rate, reduces propranolol clearance, increases plasma ciclosporin and digoxin
Why are verapamil and diltiazem contraindicated in heart failure?
Reduces cardiac output further - heart failure already has reduced output and leads to insufficient cardiac output overall
Why are verapamil/diltiazem contraindicated in heart block?
Heart block usually has slower AV node signals, non-selective CCB worsens this conduction
What are the ADRs of verapamil?
Bradycardia, hypotension from vasodilation, constipation due to GIT muscle relaxation
What are the cautions/contraindications of verapamil?
Reduces dose dose with hepatic impairment as metabolised by cyp3a4, CI in breastfeeding, pregnancy, patients with HF and AV block
What are the interactions of verapamil?
NOT to be used with beta blockers as cardiac output can be significantly reduced, increase effect of other drugs that lower BP/reduced heart rate, increases plasma ciclosporin and digoxin concentrations and grapefruit juice
What is an example of a K+ channel opener?
Nicorandil
What is the MOA of Nicorandil?
Opens K+ channels to cause hyperpolarisation and cause calcium channel to close, also an NO donor which causes arterial dilation so decreases afterload and causes venodilation which increases preload
What are the ADRs of Nicorandil?
Headache, flushing, reflex tachycardia
What are the cautions/contraindications of Nicorandil?
Hypovolaemia, CI in cardiogenic shock, hypotension
What are the interactions of Nicorandil?
Interacts with sildenafil - can Potentiate hypotension because of slow turnover of cGMP
What are some treatments for stable angina to avoid MI?
Lifestyle changes, aspirin, statins, angioplasty and stents, clopidogrel, abciximab
What is the term used to describe the process whereby a balloon is introduced to open a blocked coronary artery and stent may be inserted to maintain patency?
Angioplasty
How can platelet aggregation be inhibited in unstable angina?
Aspirin/heparin, clopidogrel, GPIIb/IIIa antagonists