retinovascular document part 2
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
risk factors of central and branch retinal artery occlusions
advancing age
diabetes
smoking
high cholesterol levels
cardiac disease
pathophysiology of central and branch retinal artery occlusions
sudden and often total obstructions to the retinal blood flow
the main cause is atheroma( build up of fatty deposits
what is this caused by
transient(short lasting) obstruction of retinal artery e.g embolus position may change and vary with blood flow
or
degree of inflammation may vary so diameter of artery varies
what does this cause
transient retinal ischemia which then leads to amourosis fugax
is amourosis fugax severe
yes it usually affects the whole visual field and lasts at least 7 minutes, usually resolves within the hour
if symptoms last more than an hour it means permanent vision loss
what may the patient describe
vision going back, grey or dim
depending on artery affected patient may describe the darkness spreading across the visual field at once
what is the main cause of amarosis fugax
acute retinal ischemia induced by carotid artery disease with secondary emboli causing blockage
are there any other causes
papillodema
migraine
what should we ask if we suspect amaurosis fugax symptoms
common symptoms of stroke/TIA: - down need to memorise just general awareness
HA- sudden , severe, unusal, associated with stiff neck
confusion
weakness
sensory loss
speech problems
dizziness
nausea
specific cranial nerve deficits(ptosis,miosis,facial anhidrosis
difficulty with fine motor coordination
neck or facial pain
we must check for FAST (what is this)
danger signs
f- Face, can the person smile/ has face fallen to one side
A- arms - can they raise both and keep them there
S- speech problems-
T- time- if you see any of these signs - call 999
what else should we check for
double vision
homonymous Vf defects(suggest post chiasmal damage)
clinical signs of arterial occlusion
poor VA
pupil defect - +ve RAPD
CRAO produce striking whitened opaque and cloudy appearance in fundus
narrowing of blood vessels
cherry red spot at central macula( CRAO characteristic sign)
cilioretinal artery
15%- 50% of population have this additional blood supply
if they get cRAO the central retinal artery maintains normal colour due to this.
may maintain VA reaso

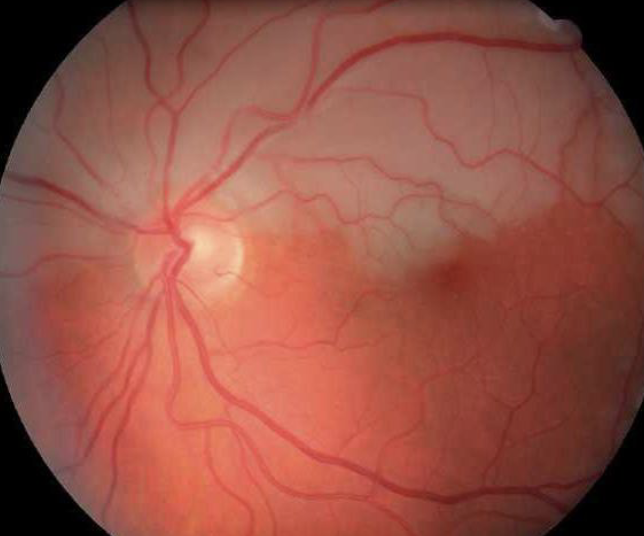
what this and how do you know
CRAO- generalised arteriole narrowing and pale fundus
cherry red spot at macula
what this and how do you know
BRAO- only superior branch has become occluded
area of pallor is confined to this hemisphere
no cherry red spot at macula( however it is possible )
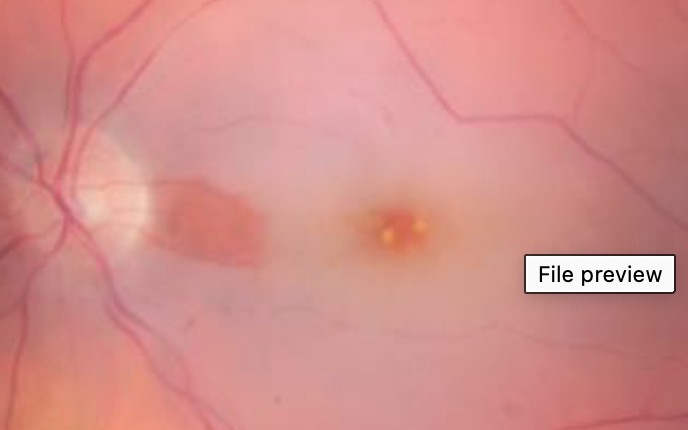
what this and how do you know
CRAO - blood flow within the retinal area between optic disc and macula is preserved
differential diagnosis
small percentage of CRAO can be attritable to Giant cell arteritis
what are distinguishing features of GCA
pain
diploipia
jaw claudication
fever
management of CRAO and BRAO
prolonged ischemia leads to infarction( irreversible cell death)
so retina cannot withstand without oxygen for very long so unless obstruction is removed within 4 hrs and under 24 hr period vision restoration is limited
management techniques
ocular massage on closed lid- 15 minutes- help blood flow
px breath into paper bag- elevates blood CO2 which increases vasodilation
refer immediately for any symptoms of severe vision loss
what should you do if amaurosis fugax symptoms identified but no abnormalities idenitified
refer to GP instead of ophthalmologist because otherwise it will delay stroke investigation- should see within 24 hrs
what does the ophthalmologist do
monitor for neovascularisation - so it can remove the stimulus to new vessel growth by destroying the damaged retinal tissue
risk factors Central and Branch Vein occlusions
age
cardiovascular risk factors (hypertension, obesity, hyperlipidemia, diabetes, glaucoma)
pathophysiology of CRVO
arteriosclerosis- thickening of wall leads to vein compression- forms thrombus then occlusion
pathophysiology of BRVO
always occur at A/V crossings
60% along the superotemproal retina
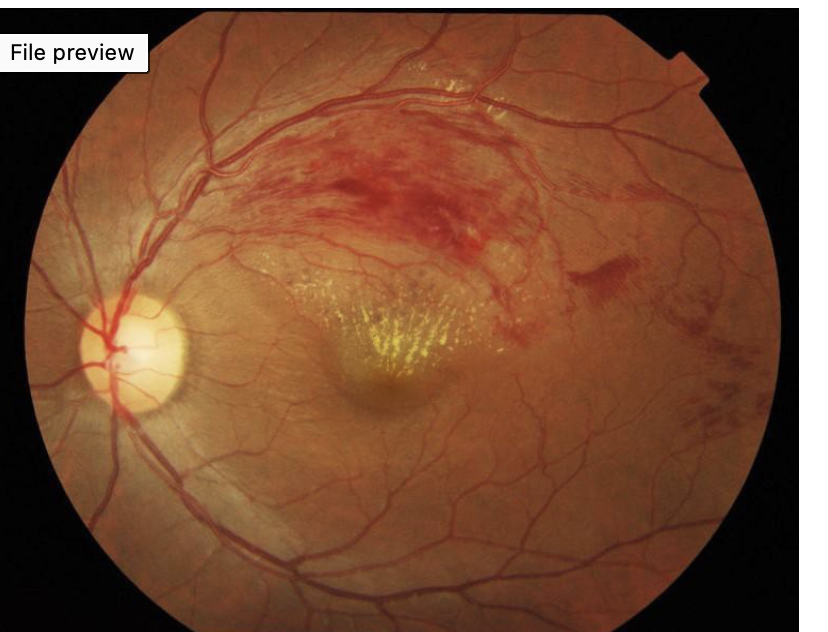
what this and how do you know
BRVO- haemorrhaging confined to superotemporal arcade
yellow deposits originating in macular are hard exudates in fan pattern- indicates fluid leaked from occluded vein has been reabsorbed
this means occlusion has started some time ago
why is it mostly in the superotemporal region
highest concentration of A/V Crossings are here
what does the A/V crossing look like
In BRVO most;y arteries crossing over vein- which means the vein is getting compressed
why might retinal haemorrhaging or oedema occur
venous occlusion disrupts drainage of blood and increases the pressure, pressure is passed backwards from retinal vein via venues to capillaries which may rupture
what does the occlusion also cause
chronic ischemia- if prolonged it leads to permanent vision loss
what’s the difference with ischemia in artery and vein occlusions
in artery occlusions retinal schema arises as a direct result of the occlusion but in vein occlusion it arises secondary to issues that occur due to the occlusion and and the impeded retinal drainage
what its the structure of arteriolar and venue capillaries
arteries narrow progressively before becoming wider and turning into veins
what does this mean for ischemia
drainage failure in wider diameter veins leads to increased intraluminal pressure(build up of pressure upstream from site of occlusion)
this pressure causes blood products(haemorrhaging,lipids,proteinplasma) transfer through vessel wall
this then impedes the outflow of blood which is oxygenated from arteriolar walls=ischemia
how long does this take
it takes time to develop days/weeks/months
that’s why vein occlusion is not classed as ischemic
is artery occlusion classed as ischemic
yes , acute severe ischemia leading to rapid infarction
CVRO symptoms
sudden, painless, monocular vision loss
BRVO symtoms
altitudinal or sectoral VF loss
if they have peripheral BRVO may be asymptomatic
Non ischemic CRVO signs
dot/blot/flame haemorrhaging all over
dilated and tortuous veins
VA varies 6/30 to 6/60
pupil reactions normal - may have mild RAPD
cotton wool spots not common
management of vein occlusions
both central and branch require opthalmolagist HES referral sooner than routine
what time line of referrals
BRVO- good vision= 4-6 weeks
BRVO - poor vision(6/12 or worse)- 2-3 weeks
all CRVO- less than 2 weeks
why do we not do routine referrals for vein occlusions
in all cases via the GP is too slow
national guidance sta