Final Maternity
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
Hormones during ovulation
High: FSH, LH (spikes), Estrogen
Low: Progesterone
GTPAL
Gravida, Term, Preterm, Abortions, Living
Estrogen placental hormone
Uteroplacental blood flow, growth
Progesterone placental hormone
Relaxation and maintenance
Human chorionic gondotropin (hCG)
"Pregnancy hormone," signals to body that pregnancy has taken place
Human placental lactogen
Stimulates maternal metabolism to supply nutrients for fetal growth
Estrogen function
stimulates development of female sex characteristics; helps regulate menstrual cycle
Progesterone function
stimulates development and maintenance of endometrium that prepares it for implantation
Fetal circulation shunts
ductus venosus, ductus arteriosus, foramen ovale
Ductus venosus
Liver
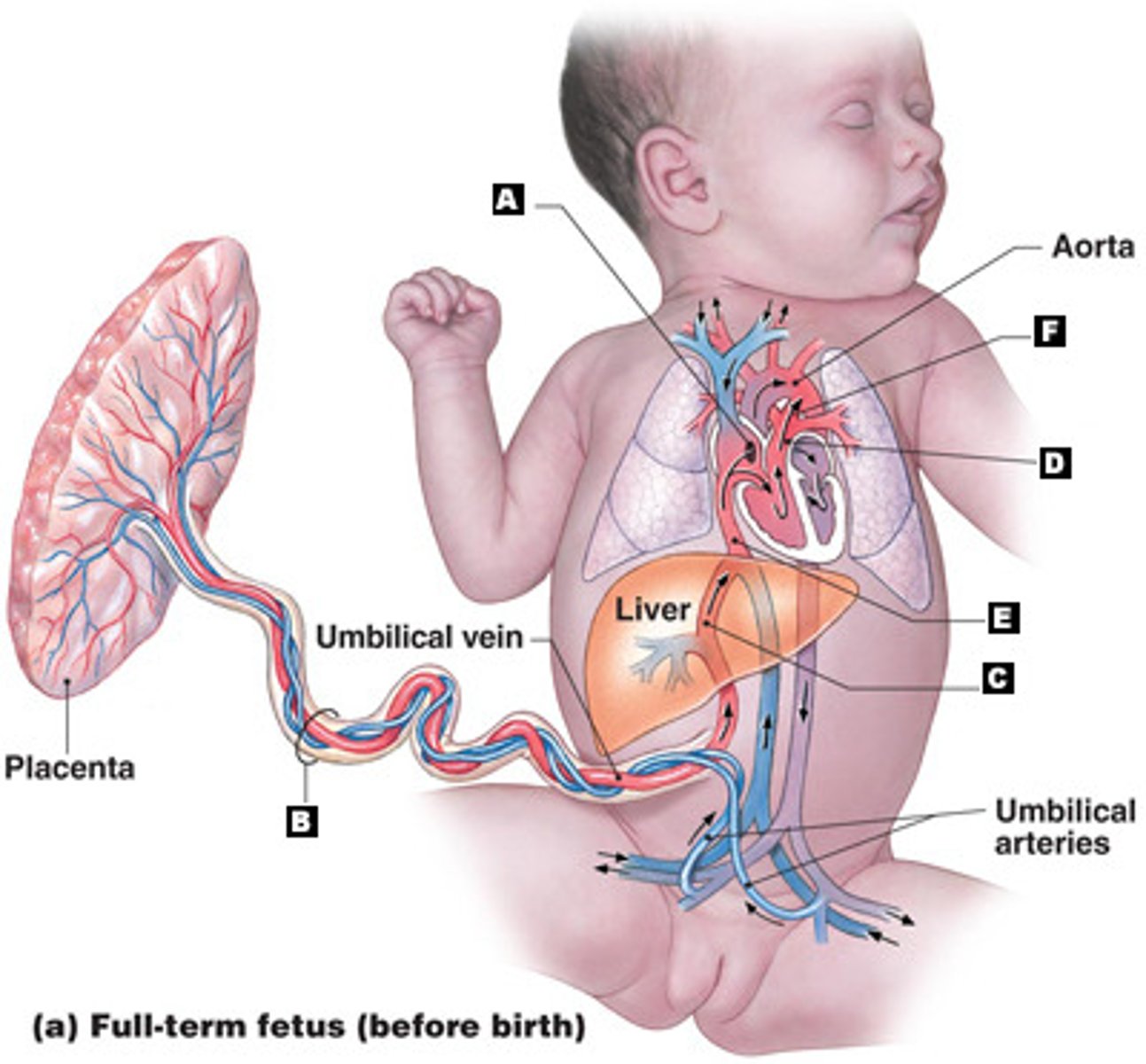
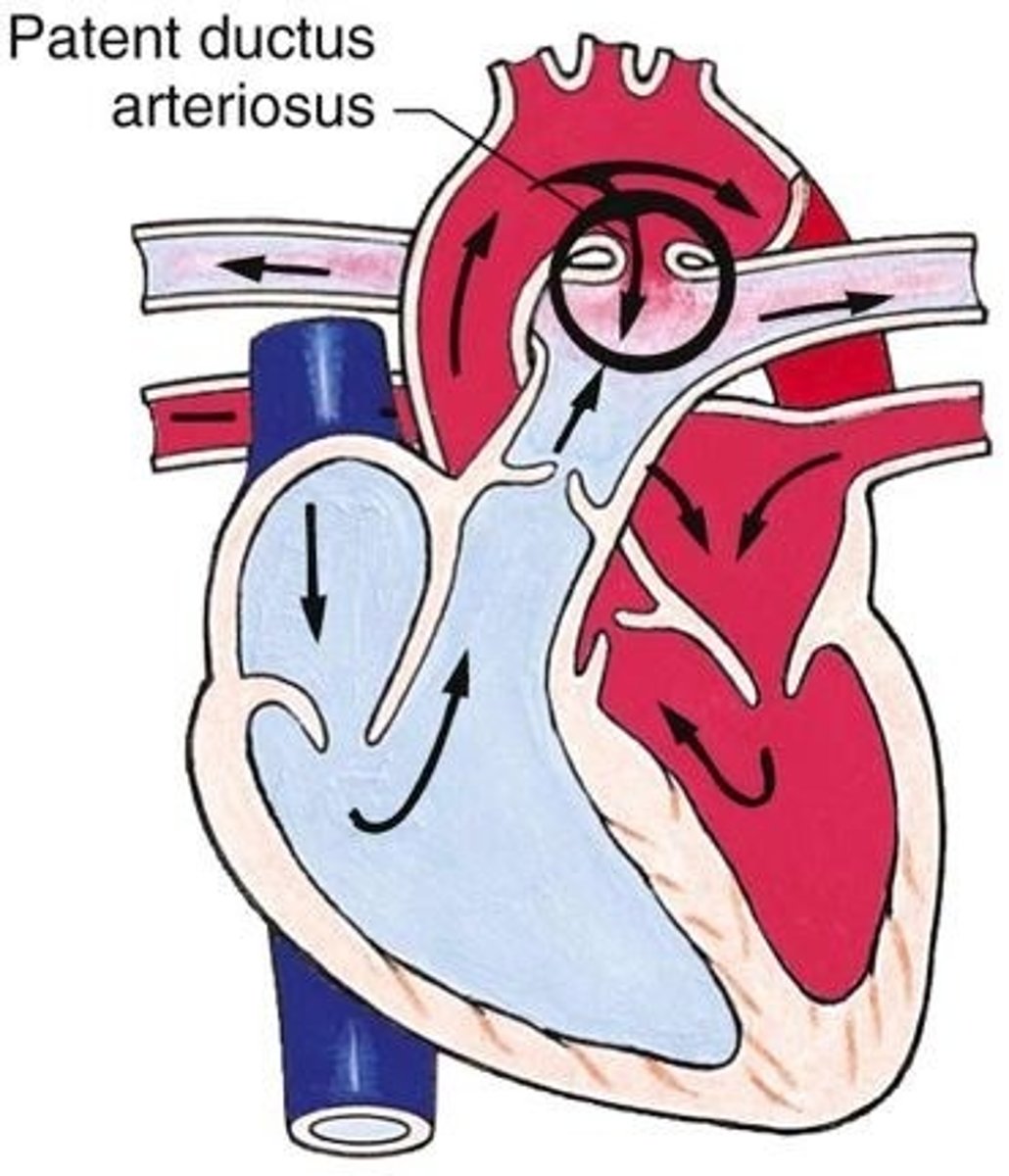
Ductus arteriosus
"Into the major artery," the aorta, bypassing fetal lungs
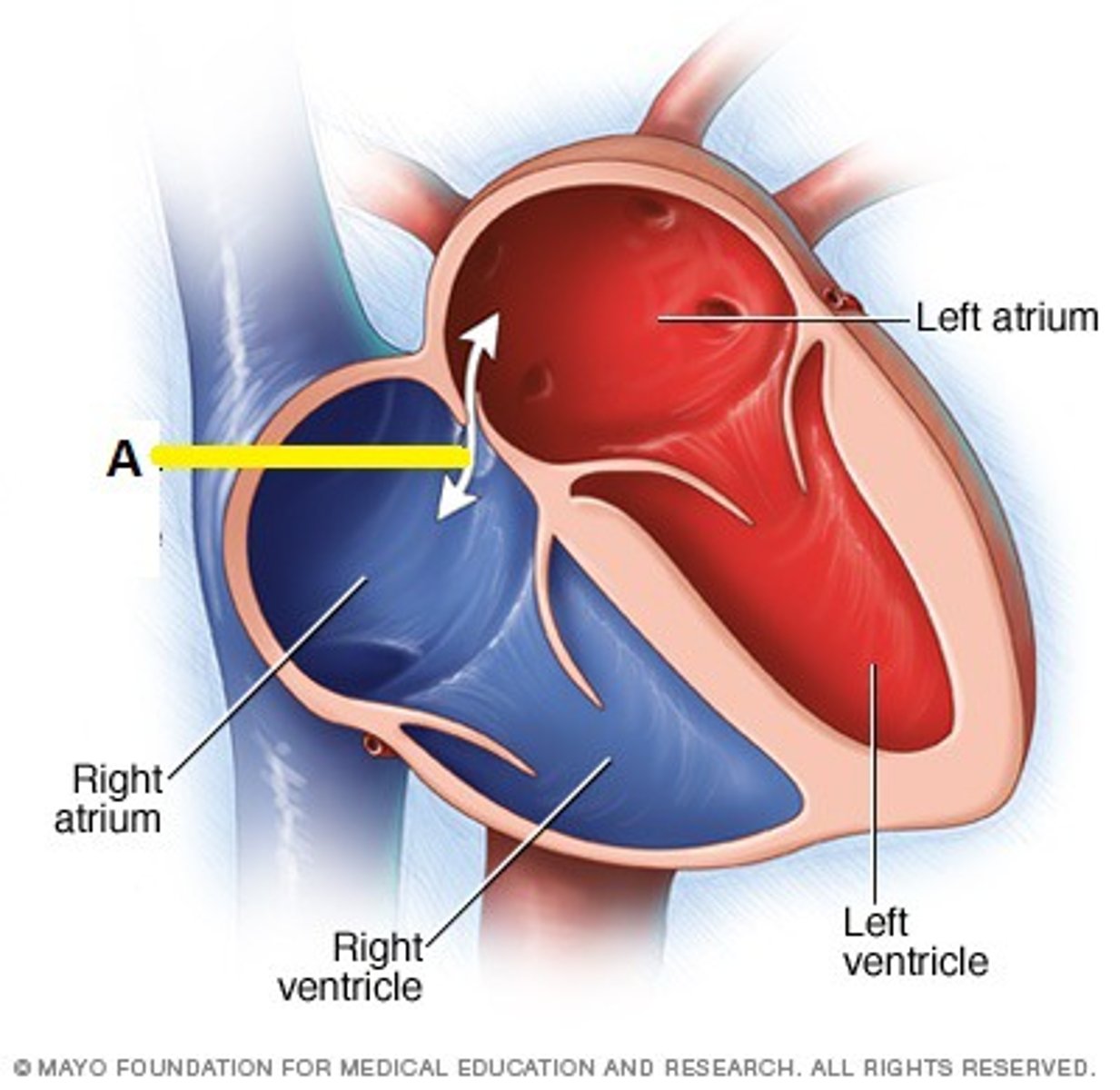
Foramen ovale
"Over the top" of the fetal heart from R atrium to L atrium
Placenta development
Begins at implantation, complete at 14 weeksChorionic villi burrow into decidua basalis
Placenta function
supply oxygen, remove wastes, immune protection, supply progesterone, estrogen and hCG
Postpartum hemorrhage (PPH)
>500 mL after SVD
> 1000 mL after C/S
PPH etiology
Tone: hypotonia (boggy uterus)
Trauma: lacerations, uterine inversion, hematoma
Tissue: retained placental fragments
Thrombin: clotting disorders
Hypertensive disorders of pregnancy (HDP)
BP > 140/90 mm Hg
Severe if > 160/110 mm Hg
Leading cause of maternal and perinatal morbidity and mortality
Preeclampsia
HTN develops at or after 20 weeks of gestation in previously normotensive woman without proteinuria d/t poor perfusion from vasospasm
What causes preeclampsia?
Poor perfusion from vasospasm
Preeclampsia symptoms
Swelling of face or hands
Fluid retention (decreased urine output)
Sudden weight gain
Persistent headache
Assessment of preeclampsia
Hypertension
Proteinuria
Cerebral disturbances (headache, visual disturbances)
RUQ epigastric pain
Eclampsia
Seizure activity or coma in woman diagnosed with preeclampsia
Gestational diabetes mellitus (GDM)
Hyperglycemia that is first recognized in pregnancy
Interventions for GDM
Antepartum: diet, exercise, blood glucose monitoring, insulin, fetal surveillance
Intrapartum: monitor Q1H, FHR, no glucose IV bolus
Postpartum: returns to normal, reoccurs, risk of NIDM
Interventions to stabilize newborn blood glucose
Skin to skin
BF
Blood sugar levels monitored
Supplementation
NICU for IV D10W
Stages of labour
Stage one: begins with regular uterine contractions, ends with full dilation
Stage two: begins with full dilation, ends with birth
Third stage: begins with birth, ends when placenta is expelled
Three phases of stage one labour
Latent: 0-3cm
Active: 4-7cm
Transition: 8-10cm
Two phases of stage two labour
Latent: passive descent
Active: pushing, urge to bear down
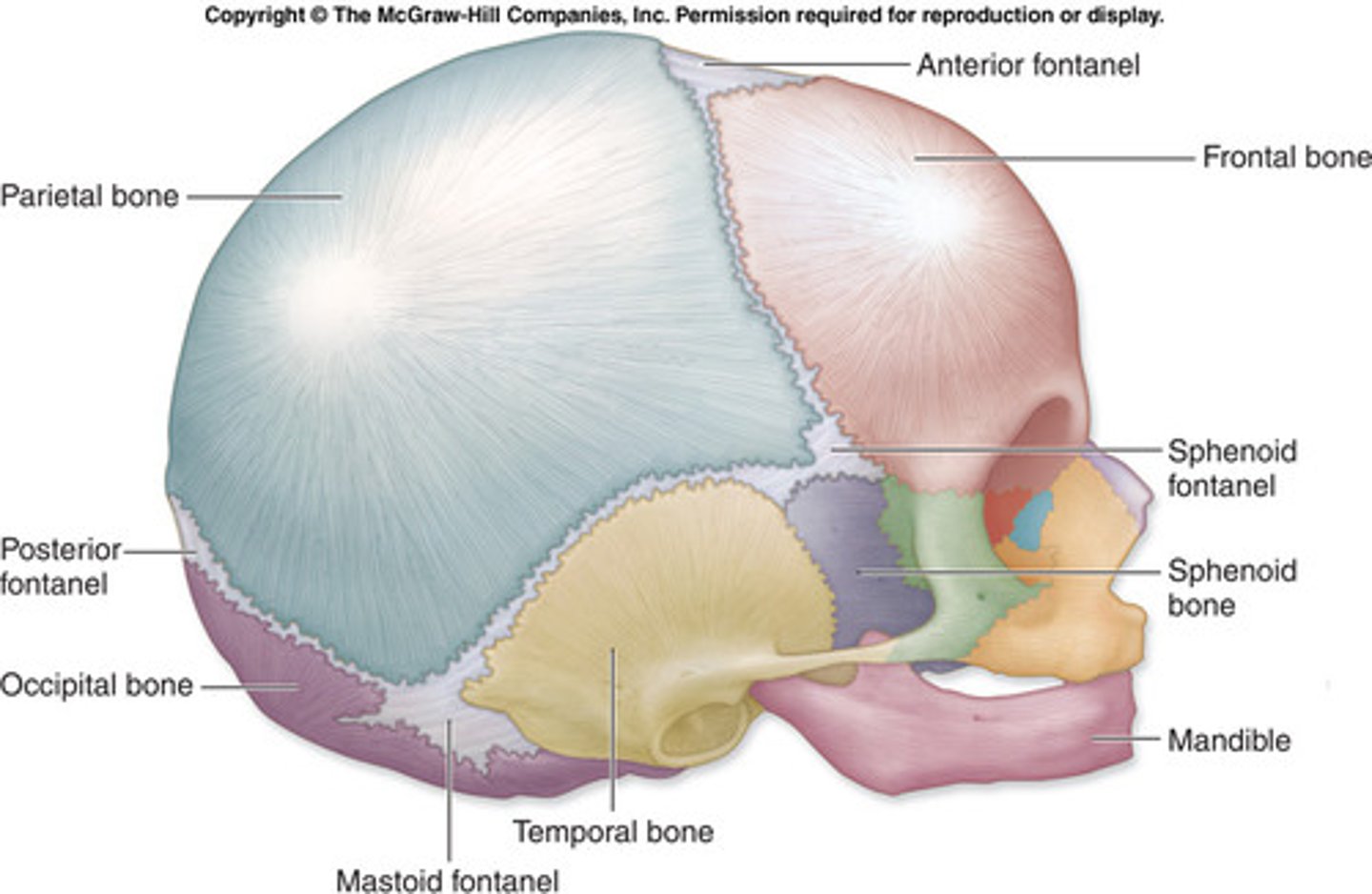
Fetal skull
Anterior fontanelle, diamond
Posterior fontanelle, triangle
Frontal, parietal, occipital, temporal bones
5 P's of labour
Passenger
Passage
Powers
Position
Psyche
5 P's: passenger
Size of fetal head
Presentation of fetus: cephalic, breech, shoulder
Cephalic presentation
birth position in which any part of the head emerges first

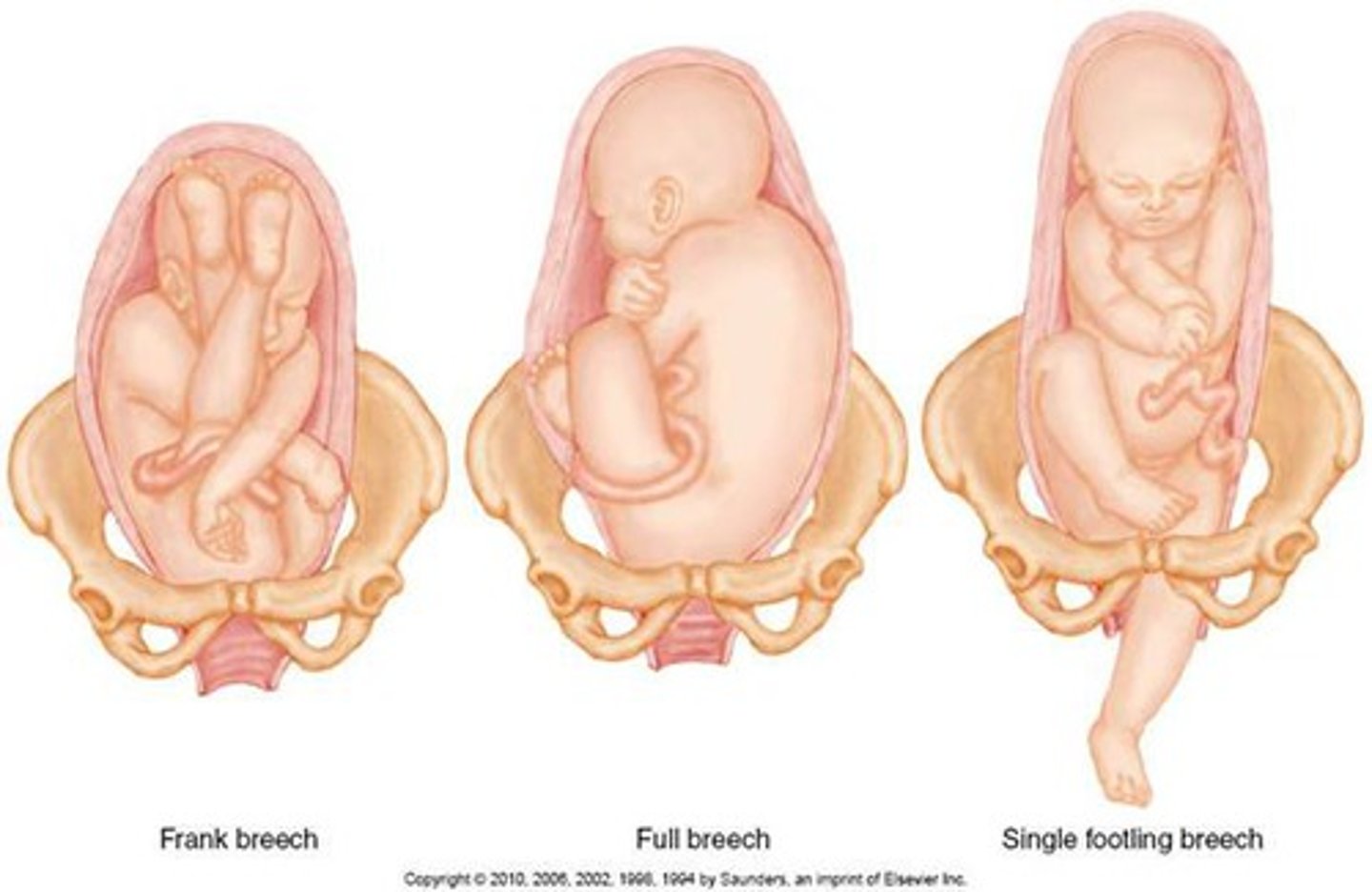
Breech presentation
birth position in which the buttocks, feet, or knees emerge first
Shoulder presentation
baby is in transverse position at delivery, must be turned

Fetal position
Lie: relation of spines, longitudinal or vertical
Presentation: vertex
Reference point: occiput (back of head)
Attitude: general flexion
5 P's: power
Primary powers: contractions
Secondary powers: bearing down efforts
7 mechanisms of labour
1. Engagement
2. Descent
3. Flexion
4. Internal rotation
5. Extension
6. Restitution and external rotation
7. Expulsion
(every dog feels intense, extreme, repulsion, everyday)
Fetal station
Measure of the degree of descent of the presenting part through the birth canal
Factors influencing contractions
Frequency, duration, intensity
Effacement
Dilation
Ferguson reflex
Valsalva maneuver (breath holding, forceful pushing)
Non pharmaceutical comfort measures
Preparation
Focusing and relaxation
Breathing techniques
Counterpressure
Touch and massage
Heat and cold
Aromatherapy
Music
Hypnosis
Pharmaceutical comfort measures
Sedatives: relieve anxiety, induce sleep
Analgesia: alleviation of pain
Anesthesia: encompasses analgesia, amnesia, relaxation, and reflex activity
Three stages of extra-uterine adaptation
1. First period of reactivity: first 30 minutes; infant is alert and responsive; HR peaks, irregular respirations
2. Period of relative inactivity: 1-2 hours; decrease in responsiveness and motor activity, sleeping; HR stabilizes, no signs of respiratory distress
3. Second period of reactivity: 4-6 hours after birth, 10 minutes to several hours; tachycardia and tachypnea; passing of meconium
Neonatal abstinence syndrome (NAS)
a condition in which a child, at birth, goes through withdrawal as a consequence of maternal drug use
Effect of alcohol on neonates
FAS, craniofacial features, microcephaly, hyperactivity developmental delays, attention deficits
Effect of cocaine on neonates
Preterm, SGA, microcephaly, poor feeding, developmental delays, congenital anomalies
Effect of heroin on neonates
LBW, SGA, irritability, tachypnea, seizures
Effect of tobacco on neonates
Preterm, LBW, risk for SIDS, risk for bronchitis and pneumonia, developmental delays
Risk factors for respiratory distress
Few alveoli
Lower levels of surfactant
Smaller lumen in airways
Greater collapsibility of airway
Weak gag reflex
Aspiration