trauma
1/36
Earn XP
Description and Tags
lecture given 6/8/2026
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
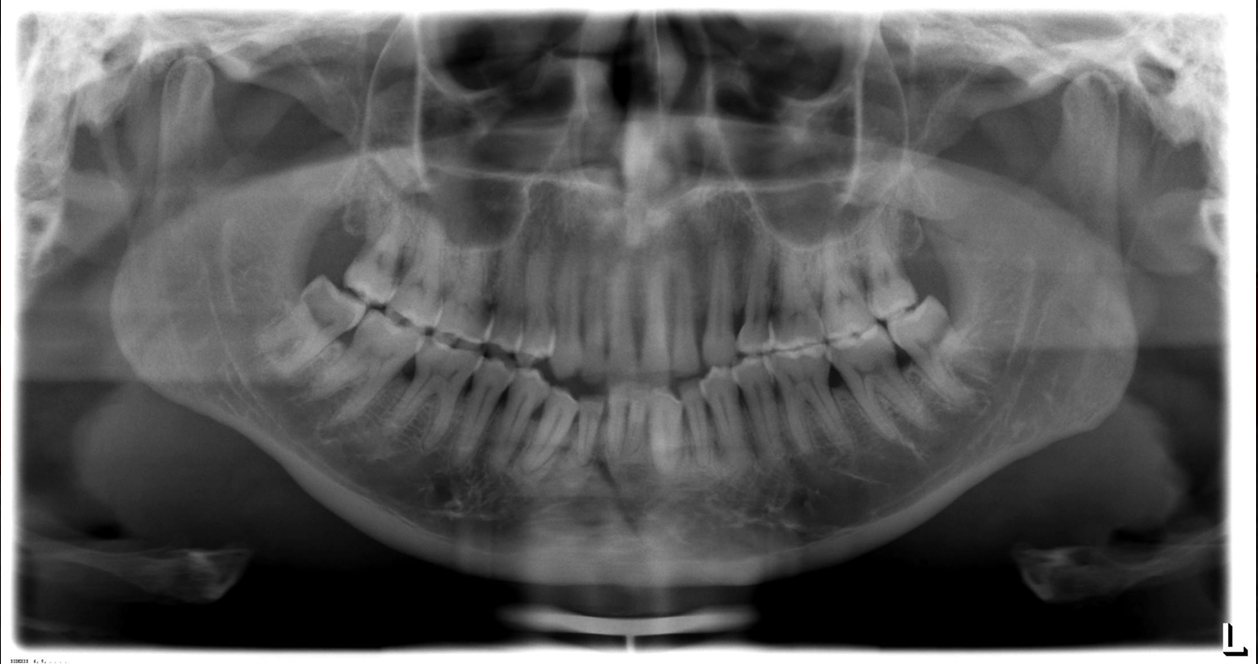
what imaging modalities are used for trauma?
panoramic- useful for localizing injuries to teeth and bone, lacks resolution and anatomic detail, esp mand anterior
periapical- always required for dentoalveolar fracture for adequate anatomical detail
occlusal- may be useful for mand body or alveolar process
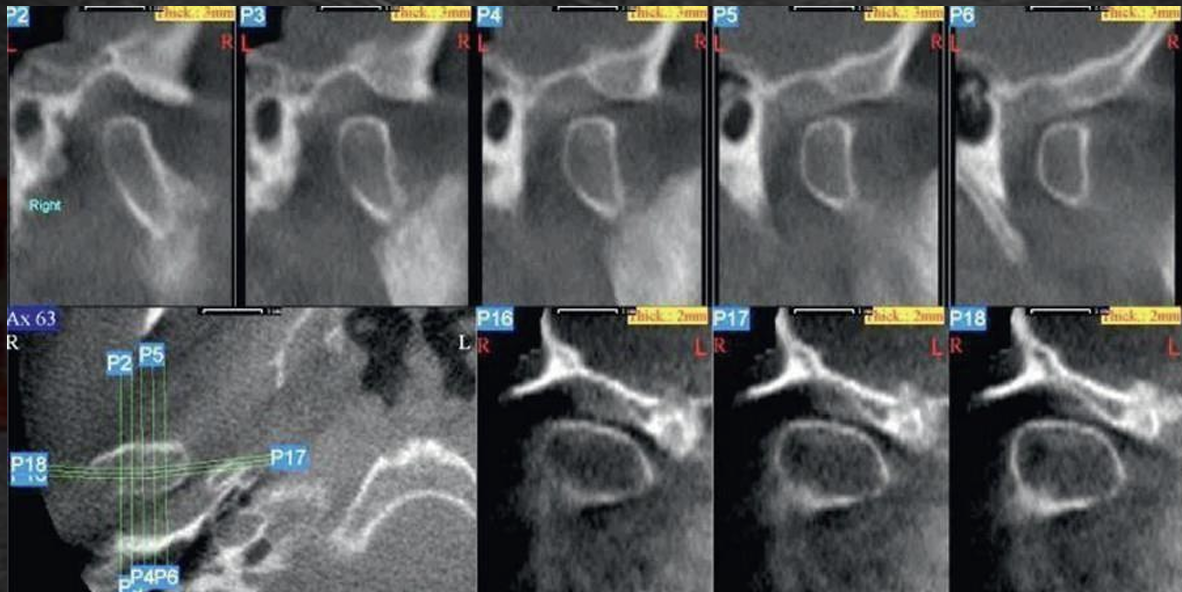
towne view- suspected trauma to the condylar head and neck areas
CBCT- method of choice for maxillofacial fractures, particularly multiple bone
*concussion
crushing injury to the tooth apex and PDL
minimal loosening or displacement
slight hyperocclusion
percussion sensitive
radiographically subtle, slightly widened PDL particularly in the apical 1/3
monitor with slight occlusal adjustment if necessary
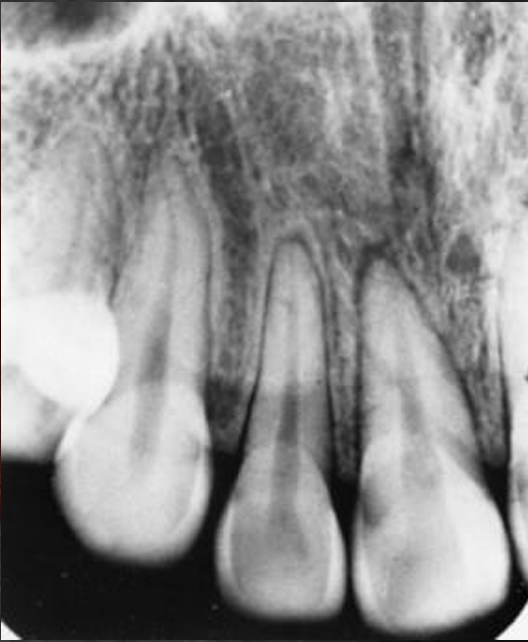
concussion
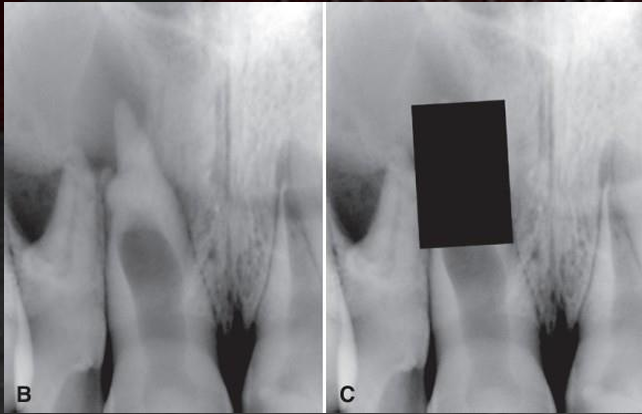
what is this, and what does it result from?
osteodentin cap, concussion
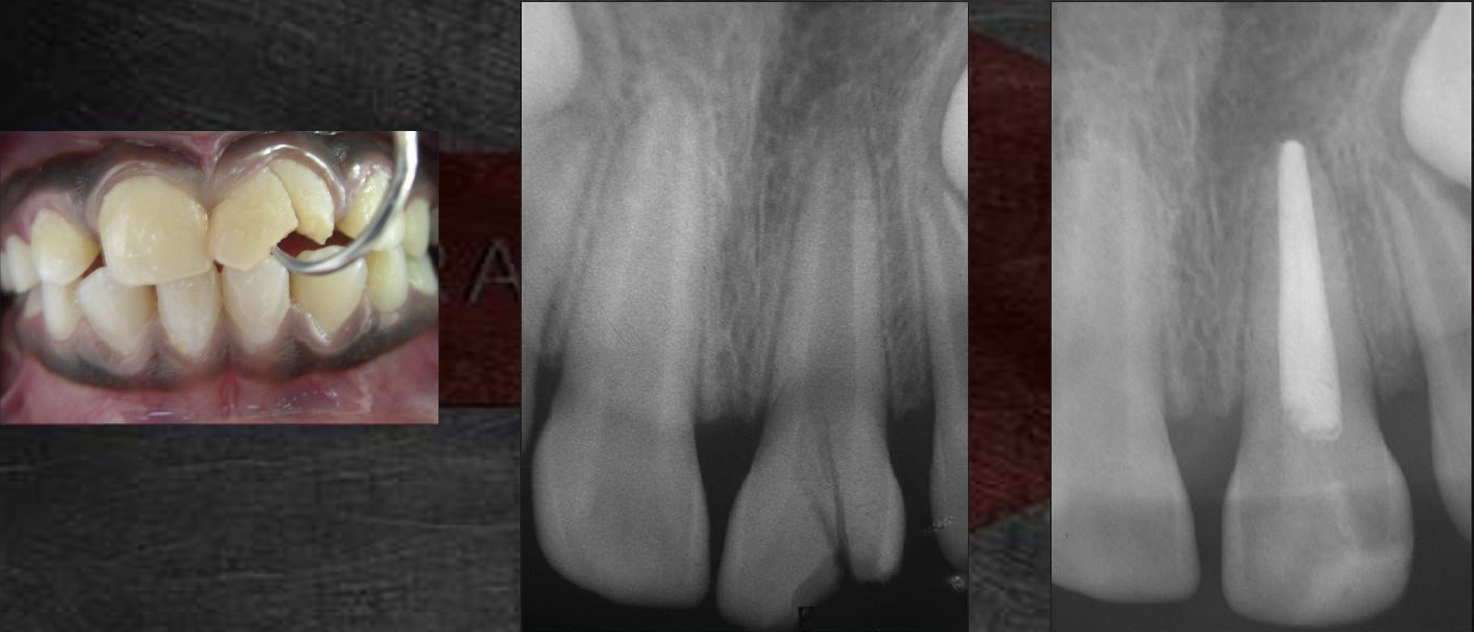
osteodentin cap
trauma results in pulpal necrosis
vital odontoblasts at the apex deposit tertiary dentin, coronal portion of the root remains open
*luxation
PDL is severed
teeth are displaced/mobile
subluxation implied the PDL is injured without frank dislocation
radiographically subtle, slightly widened PDL, similar to concussion but may show altered position of tooth, may require occlusal projections
management: reposition and splint, remove if in proximity to a developing adult tooth
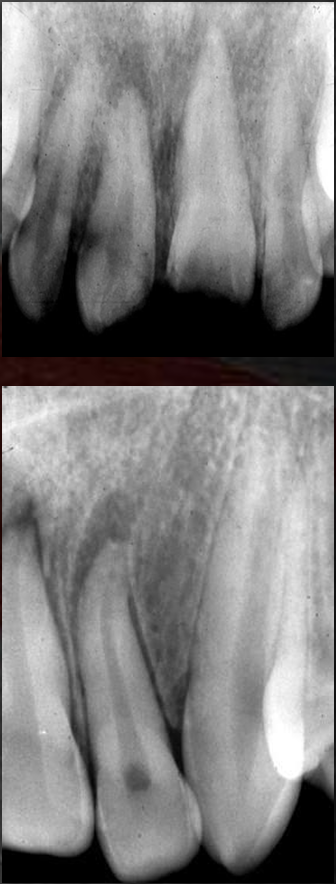
luxation
*avulsion
complete displacement from the alveolar process
fights are the most common cause, max central incisors are most common teeth
lamina dura often persists for up to several months
if the tooth is not found- chest radiograph to rule out aspiration
can attempt to reimplant if out of mouth for a short period of time, RCT ~2 weeks later

avulsion
re-implantation
the time outside of the socked for an avulsed tooth is the most critical factor for its survival
if the tooth in replanted within 30 min or kept in a physiological solution of specialized media or milk for a few hours, it has a fairly good prognosis
if the tooth has been dry for more than one hour, the PDL cannot be expected for survive and the tooth will likely become ankylosed
*class I crown fracture
involve enamel only (infraction or crack)
no treatment required, smooth edges, monitor with vitality tests, 2% pulp necrosis
*class II crown fracture
involve enamel and dentin (uncomplicated fracture)
horizontal better prognosis than oblique (due to less surface area of dentin exposed)
3% pulpal necrosis
*class III crown fracture
involve enamel, dentin, and pulp (complicated fracture)
pulp cap vs pulpotomy vs pulpectomy
deciduous teeth often extracted
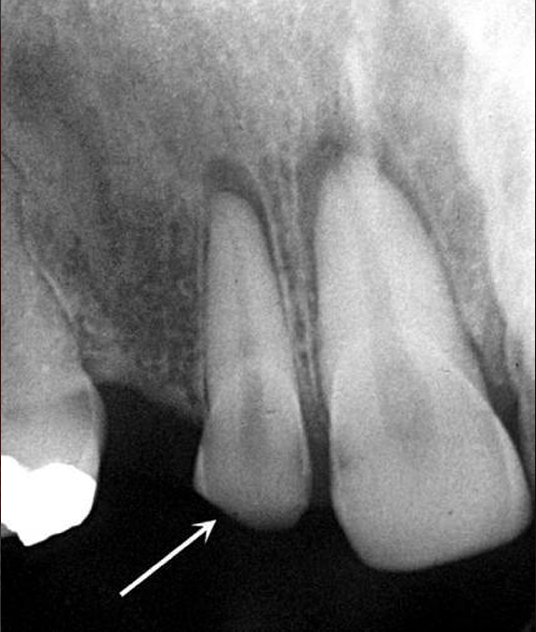
crown fracture
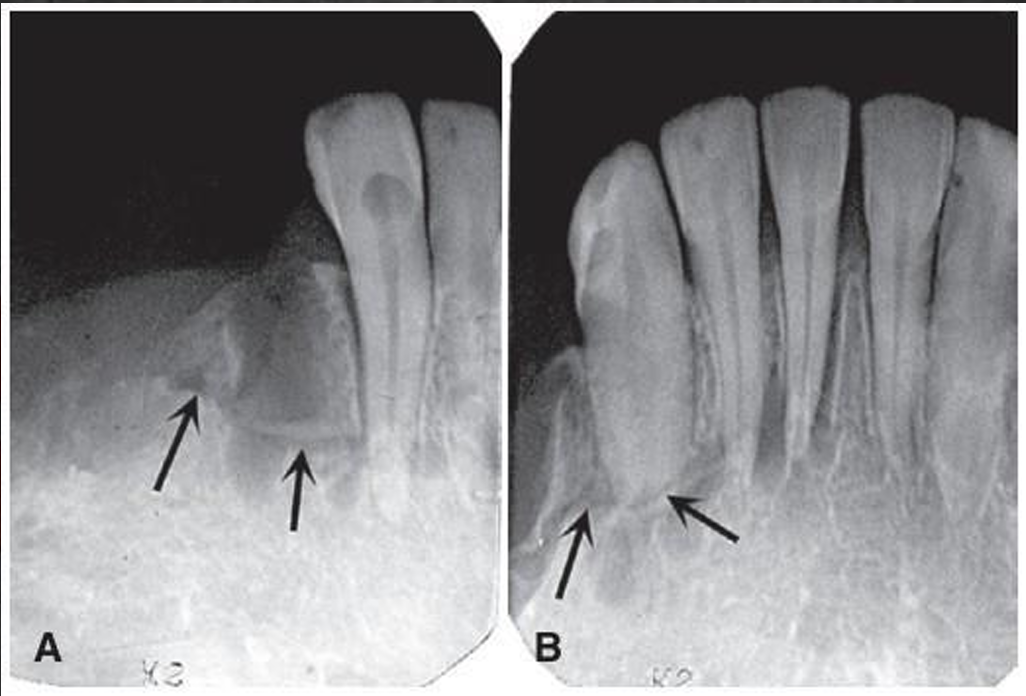
horizontal root fracture
uncommon- account for 7% or fewer traumatic injuries to permanent teeth
most occur in middle 1/3 of root
not always visible
can sometimes see increased PDL space size adjacent to fracture location
fracture in coronal 1/3 of root has poor prognosis, usually extract
fracture in middle or apical 1/3 of roots only 20-24% get pulpal necrosis
vertical root fractures
usually oriented in the facial-lingual plane
most frequently in posterior teeth, esp mand molars
usually iatrogenic following insertion of screws or pins
patient complains of persistent dull pain (cracked tooth syndrome)
extract single rooted teeth, hemisect multi-rooted teeth
crown-root fracture
just what the name implies
management: remove coronal fragment to evaluate the extent of the fracture if pulp involvement usually extract, if no pulp involvement and does not extend more than 3-4mm below the epithelial attachment, usually able to restore
crown-root fracture
*
alveolar process fracture
*radiographic signs of fracture
radiolucent line contained within the boundaries of a bone
a change in the normal outline or shape of a structure (bone or teeth)
loss of continuity of outer border; gap or **step defect
increased radiopacity in a structure (overlap)

normal anatomy!! space between tongue and soft palate from pt swallowing mid pano
where are the most common mandibular fractures?
condylar (29.1%), angle (24.5%, associated with extraction of impacted teeth), symphysis (22%)

**
mandibular fracture
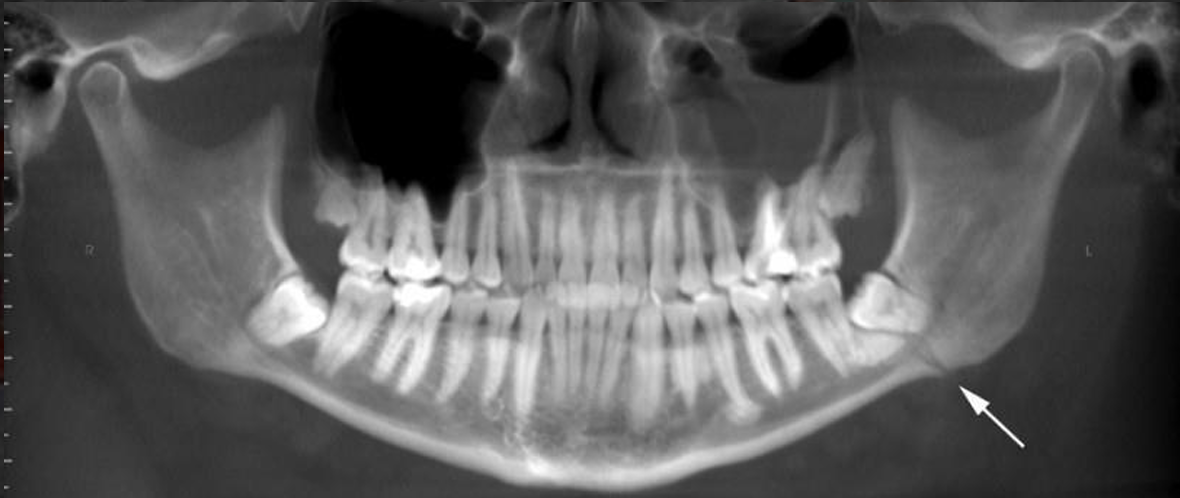
mandibular fracture
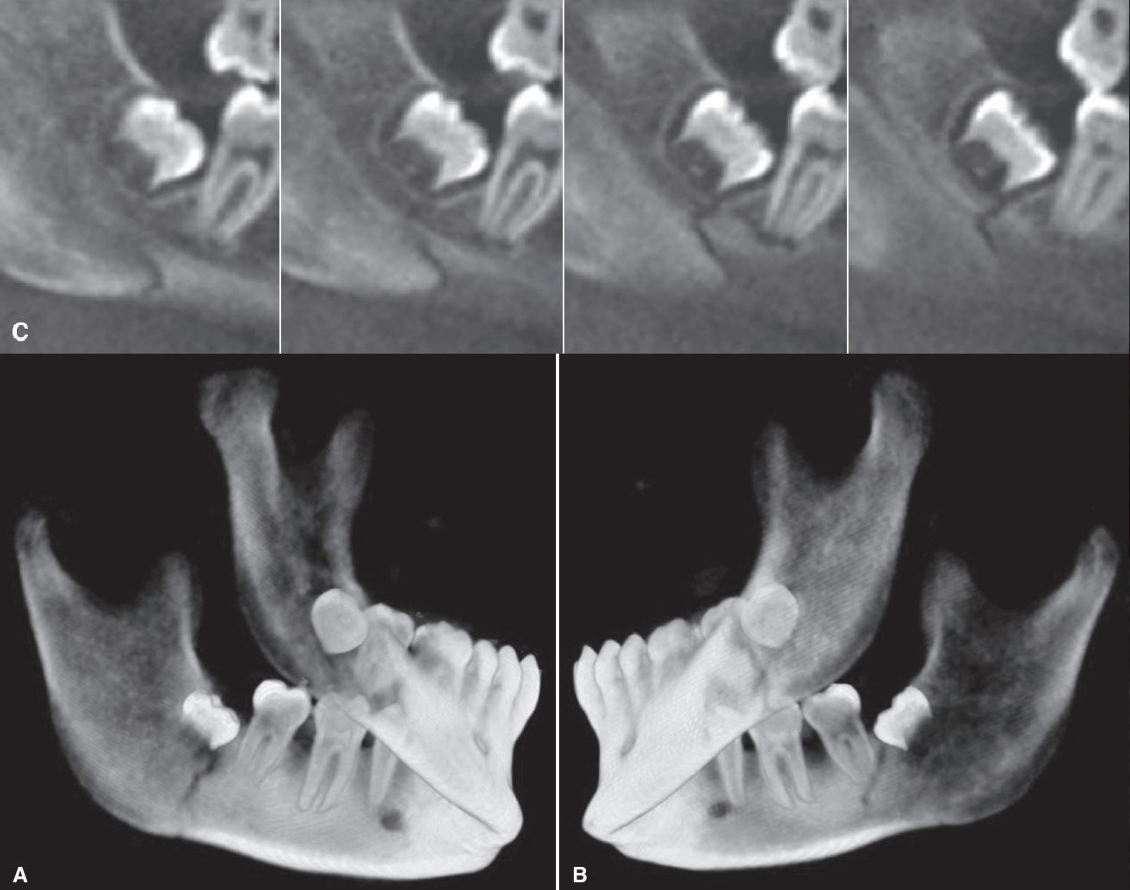
mandibular fracture
**
mandibular fracture
mandibular fracture
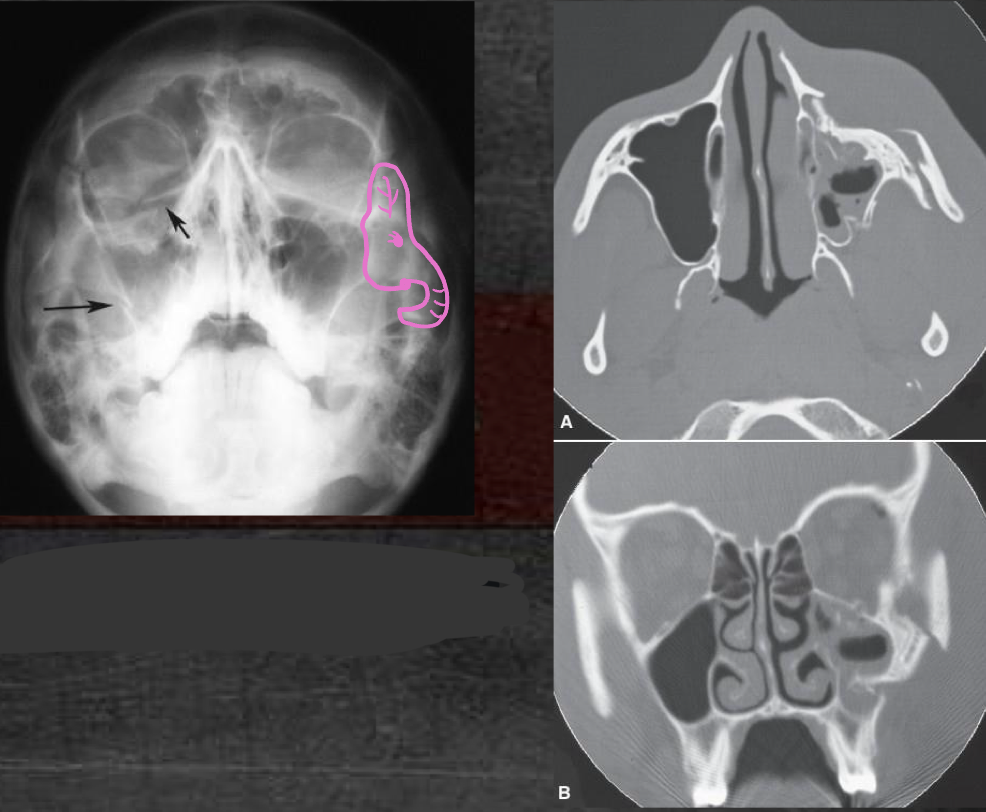
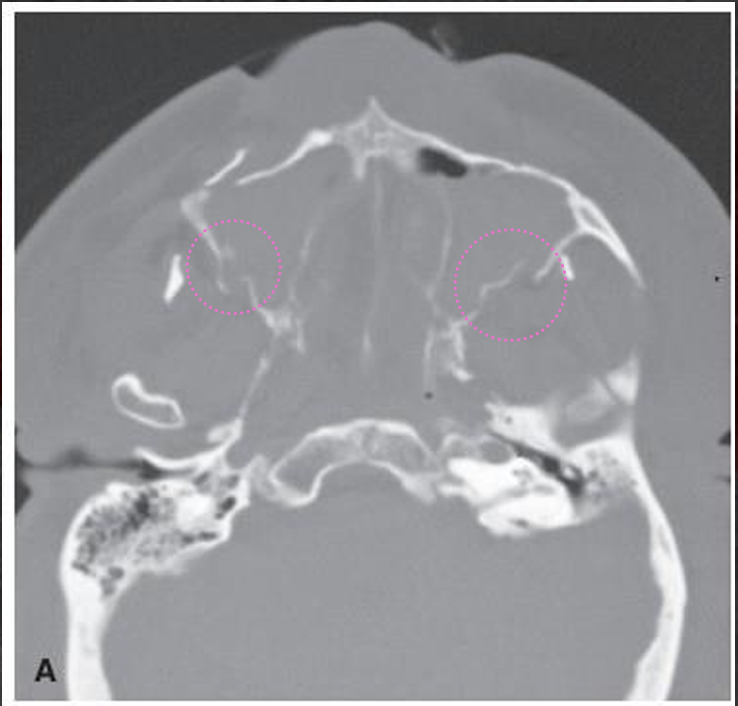
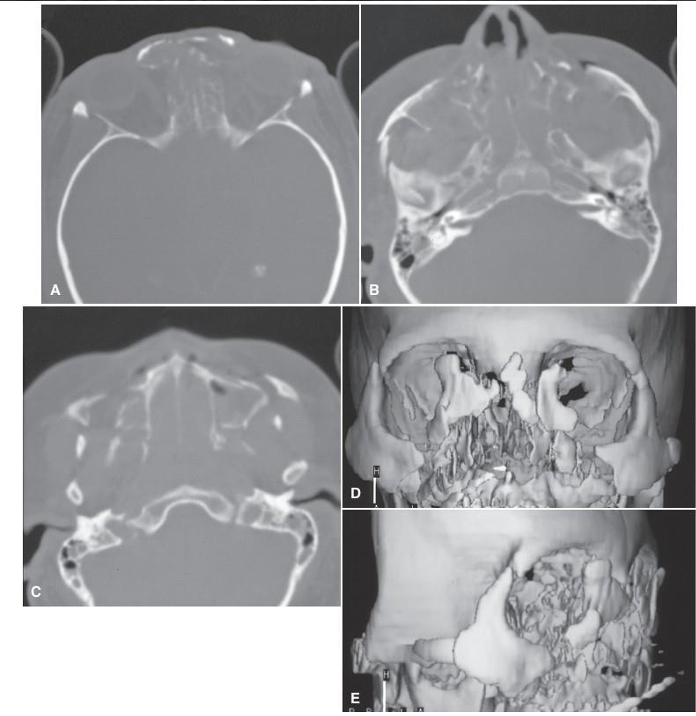
maxillary fracture
commonly orbital wall- lamina papyracea (medial wall) and floor
associated with domestic violence
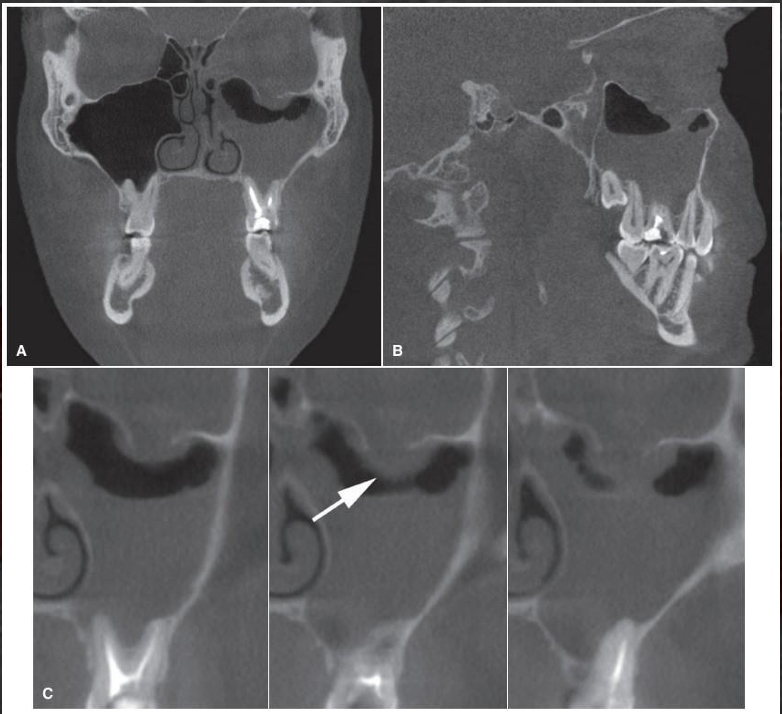
maxillary fracture
zygomatic tripod fracture- look for the elephant
lefort I fracture
horizontal
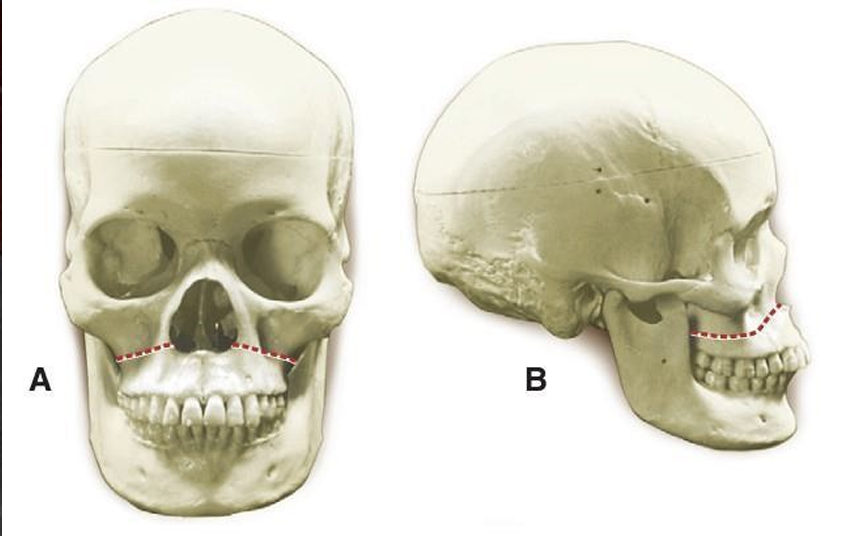
lefort I fracture
lefort II fracture
pyramidal
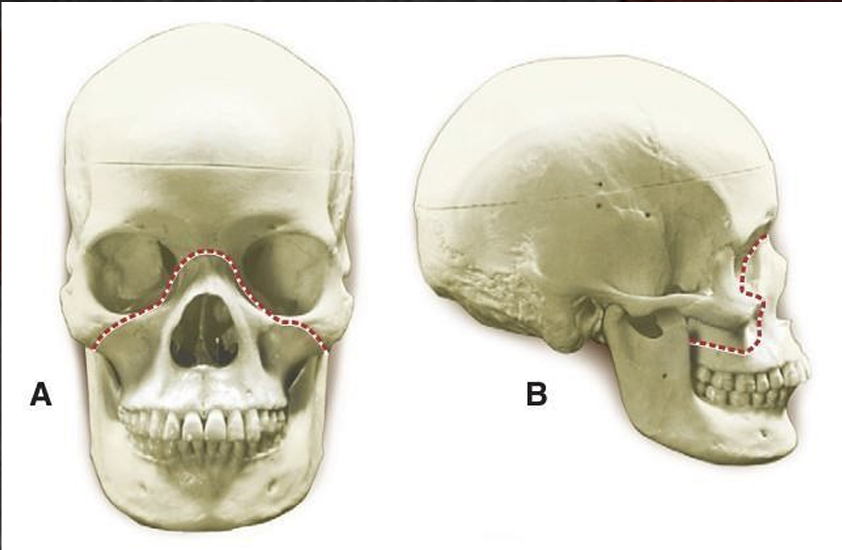

lefort II fracture
lefort III fracture
craniofacial disjunction
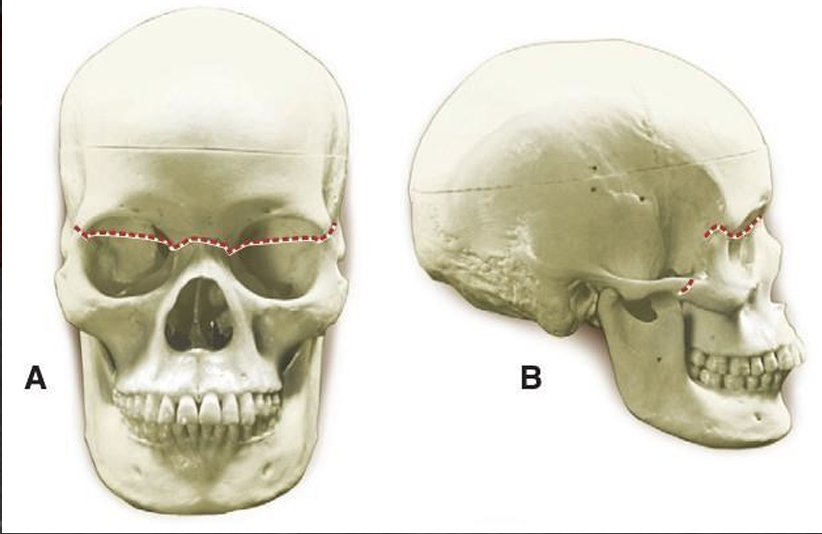
lefort III fracture
what is the monitoring/healing for lefort fractures?
examine alignment of cortical plates and remodeling/remineralization
fracture increased in width 2 weeks after reduction, remineralization occurs 5-6 weeks after treatment
obliteration of fracture line may take several months and occasionally it lasts for several years
look out for non-union and misalignment of fractured segments, inflammatory lesions associated with teeth in the area, osteomyelitis