Maternity Med Exam (in progress)
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
Tocolytics
given to stop labor contractions & cervical changes (stops and slows contraction)
No FDA approval, all off label
They do not prevent pre-term brits, just give more time
Maternal C/I to tocolytics
Preeclampsia with severe features or eclampsia
Bleeding with hemodynamic instability
Fetal C/I to tocolytics
• Intrauterine fetal demise
• Lethal fetal anomaly
• Nonreassuring fetal status
• Chorioamnionitis
• Preterm Prelabor ROM
Nursing Care for the Woman Receiving Tocolytic Therapy
explain purpose & S/E
Position the woman on her side to enhance placental perfusion and reduce pressure on the cervix
monitor vitals and FHR
asses for adverse reactions
asses fluid I&O
Limit fluid intake to 2500–3000 mL/day, especially if a beta2-adrenergic agonist or magnesium sulfate is being administered
offer support and other comfort measures
Magnesium Sulfate: Action
tocolytic
NS depressant
relaxes smooth muscles (uterus)
Magnesium Sulfate: Dosage & Route
IV fluid should contain 40g in 1000ml piggyback
Loading: 4-6 g over 20-30 Minutes
Maintenance: 1-4g per hour
d/c in 24-48 hours at maintenance dose or if adverse effects occur
Magnesium Sulfate: adverse effects in mom
hot flushes, sweating
burning @ IV site
nausea & vomiting
dry mouth
drowsiness/ dizzyness/ lethargy
diplopia (double vision)
headache
ileus (GI slowing)
muscle weakness
hypocalcemia
dyspnea
transient hypotension
Magnesium Sulfate: emergency adverse effects in mom
RR less than 12
pulmonary edema
Absent DTR
Chest pain
severe hypertension
Altered LOC
extreme muscle weakness
urine output less that 25-30ml/hr or less than 100ml/hr
serum levels 10 MEql (9mg/dl) or greater
Magnesium Sulfate: adverse effects in baby
decreased FHR and variability
decreased fetal movement
Magnesium Sulfate: Nursing considerations
asses baseline before giving med, and before & after each dose
usually IV but may be IM
therapeutic rane 4-7.5 mEq (5-8mg)
calcium gluconate: antidote
Total IV intake limited to 125ml/hr
C/I: myasthenia gravis, hypocalcemia, renal failure
Terbutaline (Brehtine) Class & action
tocolytic - inhibits uterine activity & causes bronchodilation
Beta-2 adrenergic agonist (beta-mimetic)
Terbutaline (Brehtine) Dosage & route
Sub Q .25 mg Q4hr
No longer than 24 hrs
d/c if adverse effects occur
Terbutaline (Brehtine) Adverse effects in mom (12)
most are mild and transient
tachycardia chest discomfort
palpitations
arrythmias
tremors
dizzy
nervous
headache
nasal congestion
nausea&vomiting
hypokalemia
hyperglycemia
hypotension
Terbutaline (Brehtine) Intolerable Adverse effects in mom
HR above 130 bpm
BP greater than 90/60
chest pain
arrhythmia
MI
Pulmonary edema
Terbutaline (Brehtine) Adverse effects in baby
tachycardia
decreased FHR variability
Terbutaline (Brehtine) C/I
known or suspected heart disease
diabetes of any kind
preeclampsia or s/s of eclampsia
hyperthyroidism
glaucoma
seizure disorders
Terbutaline (Brehtine) nursing considerations
asses glucose and potassium levels before giving and periodically
significant hyperglycemia - above 180 mg/dl (more likely when she is on corticosteroids)
propranolol (inderal) reverses S/E r/t cardiac function
Terbutaline (Brehtine): Notify OB if
HR over 130
arrhythmia or chest pain
BP over 90/60
s/s of pulmonary edema (dyspnea, crackles, decreased SpO2)
FHR over 180
Inodmethacin (Indocin) class & Action
tocolytitic - relaxes uterine muscle by inhibiting prostaglandins
Prostaglandin synthetase inhibitor (NSAID)
Inodmethacin (Indocin) dosage and route
loading: 50 mg PO
maintenance: 25-50 mg PO q6-8hrs
no more than 48hrs
Inodmethacin (Indocin) adverse effects on mom (3 common & 4 serious)
common: nausea/vomiting, heartburn, dizziness
less common & more serious : GI bleeding, prolonged bleeding time, thrombocytopenia, asthma in aspirin sensitive pts.
Inodmethacin (Indocin) adverse effects on baby
constricts ductus arteriosus
oligohydramnos - reduced fetal urine production
neonatal pulmonary hypertension
Inodmethacin (Indocin) C/I
renal/ hepatic disease
active peptic ulcer disease
poorly controlled hypotension
asthma
coagulation disorders
Inodmethacin (Indocin) nursing considerations
only used if gestational age is less than 32 weeks
long acting formulas decrease incidence of adverse effects
may mask maternal fever
asses AFV and fetal ductus arteriosus before giving and within 48 hours of d/c
give with food to lessen GI effects
monitor for s/s of pp hemorrhage
Nifedipine (adalat, Procardia) class & action
tocolytic - relaxes smooth muscle by blocking calcium entry
calcium channel blocker
Nifedipine (adalat, Procardia) dosage and route
loading: 10-20 mg PO q3-6 hrs until contractions are rare
maintenance: long acting 30-60 mg q8-12 hrs for 48 hrs with corticosteroids
Nifedipine (adalat, Procardia) adverse effects on mom
hypotension
headache
flushing
dizziness
nausea
Nifedipine (adalat, Procardia) adverse effects on baby
hypotension (questionable ??)
Nifedipine (adalat, Procardia) C/I
intrauterine infection
hypertension/ cardiac disease’
not used with magnesium - skeletal muscle blockade
not used with terbutaline - HR and BP effects
No sunblingual routes
Antenetal glucocorticoid therapy (betamethasone or dexamethasone) Action
stimulates fetal lung maturity
promotes release of enzymes that undue surfactant
also mature brain, kindly and gut
FDA has not approved for this use, its off-label for OB
Antenetal glucocorticoid therapy (betamethasone or dexamethasone) Indication
preventing/ reducing neonatal respiratory distress syndrome
accelerates lung maturity @ 24-34 wks gestation
infants are less likely to experience intraventricular hemorrhage, necrotizing enterocolitis or death.
Antenetal glucocorticoid therapy (betamethasone or dexamethasone) maternal effects
increases WBC and platelet count (transient 72hrs)
hyperglycemia
Antenetal glucocorticoid therapy (betamethasone or dexamethasone) fetus effects
decrease in breathing movement and body movements
transient - 48-72 hours after last dose
Antenetal glucocorticoid therapy (betamethasone or dexamethasone) Nursing considerations
deep IM injection in ventral gluteal or vastus laterals
alway IM, never PO
injection is painful
should not effect BP
asses blood glucose
diabetics may need increased insulin for several days
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) Action
ripens/ softens cervix
begins dilation and effacement
stimulates contractions
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) indications + C/I
for ripening the cervix before using Pitocin when bishop score is 4 or less
to induce labor or abortion
Not FDA approved for this use; used off label
C/I: hx of c-section or major uterine surgery
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) vaginal dosage
initial dose - 25 mcg
void before insertion
administer in or near brith unit (pills need to be spilt in pharmacy)
inset using fingers without lubricant
Redose if: cervix remains unchanged, uterine activity is minimal, FHR is normal (category 1), and at least 3hrs have passed since last dose
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) oral dosage
initial dose - 25 mcg
administer in or near brith unit (pills need to be spilt in pharmacy)
may increase labor satisfaction, comfort and convenience
administer in or near brith unit (pills need to be spilt in pharmacy)
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) adverse effects
dose dependent (higher risk with high, frequent doses)
uterine tachysystole (more than 5 contractions in 10 minutes) with or without abnormal FHR
Prostaglandin S/E
tachysystole
fever
chills
vomiting
diarrhea
Prostoglandin E1 (PGE1): Misoprostol (Cytotec) nursing considerations
obtained informed consent
asses: maternal vitals, FHR, cervical ripening, induction of labor, signs of impending labor, bishop score
asses before and during course of treatment (4hrs after each dose)
if adverse effects occur, administer 0.25 mg SubQ of terbutaline
oxytocin cannot be given until at least 4hrs have passed since last dose to induce labor
Prostoglandin E2 (PGE2); dinoprostone (cervadil insert/ prepidil gel) action
ripens and softens cervix → effacement and dilation
stimulates contractions
the onlyl med FDA approved for cervical ripening or labor induction
Prostaglandin E2 (PGE2); dinoprostone (cervadil insert/ prepidil gel) indications and C/I
used for pre induction cervical ripening (before pitocin when bishop score is 4 or less)
used for induction of labor or abortion
C/I - hx of c-section or other major uterine surgery
Prostaglandin E2 (PGE2); dinoprostone cervadil insert Dosage & route
10mg gradually released (0.3mg/hr) over 12hr
insert removed after 12 hrs, or at the onset of active labor, or if tachysystole and abnormal FHR occur
frozen until just before insertion , no warming needed
administer in or near brith unit
mom is in supine position with a lateral tilt, or side lying position for 2hrs after insertion
pull string and give 0.25 terbutaline SubQ if adverse effects occur
Prostaglandin E2 (PGE2); dinoprostone prepidil gel Dosage & route
0.5mg in a 2.5 mL syringe
bring gel to room temp, but do not force warming (can inactivate drug)
mom is in supine position with a lateral tilt, or side lying position for 30 min after insertion
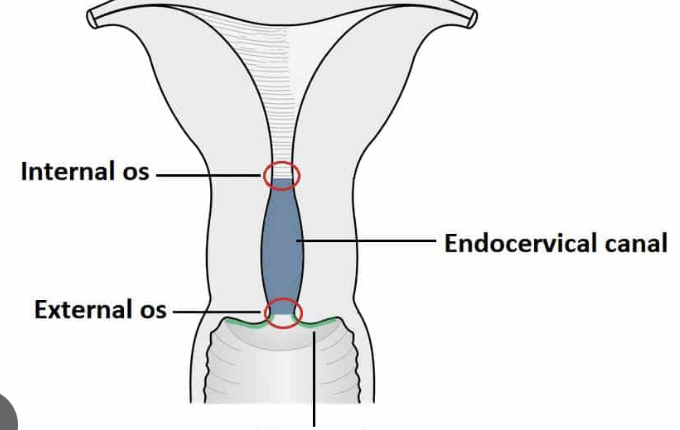
attached to catheter inserted into the cervical canal just below internal cervical os.
dose may be repeated q6 hrs PRN for cervial ripening
max dose of 1.5mg (3 doses) in a 24hr period
administer in or near brith unit
cant be effectively removed if adverse effects occur
Prostaglandin E2 (PGE2); dinoprostone (cervadil insert/ prepidil gel) adverse effects
headache
nausea/ vomiting, diarrhea
fever
hypotension
uterine tachystole w/ or w/o abnormal FHR
fetal massage of meconium
Prostaglandin E2 (PGE2); dinoprostone (cervadil insert/ prepidil gel) nursing considerations
informed consent
asses: maternal vitals, FHR, cervical ripening, induction of labor, signs of impending labor, bishop score
continuously monitor FHR and uterine activity while the insert is in after 15min after it has been removed
she can ambulate after initial period of bed rest is done and if continuous EFM telemetry is available
Gel: cant be effectively removed if adverse effects occur
delay Pitocin for 6-12 hrs after last dose of gel, and 30-60 min after removing insert
oxytocin (pitocin) action
hormone produced in the posterior pituitary gland
stimulates uterine contractions
aids in milk ejection
pitocin = synthetic form of oxytocin
oxytocin (pitocin) indications
labor induction and augmentation
controls pp bleeding
oxytocin (pitocin) dosage (Concentrations)
standard concentrations:
10 units in 1000ml
20 units in 1000ml
30 units in 500ml
always IV pump
oxytocin (pitocin) route and goal
always IV pump
begin at 1-2 milliuntis/min
increase by 1-2 milliunits/min, no more frequently than 30-60 minutes based on response
we want to use the lowest does possible to achieve adequate labor
signs of adequate labor include: progressive effacement, dilation of 0.5-1cm/hr after active labor has been achieved
oxytocin (pitocin) adverse effects on mom
uterine tachysystole
placental abruption
uterine rupture
oxytocin (pitocin) adverse effects on fetus
fetal compromise
progressive decline in oxygen status
neonatal acidemia
oxytocin (pitocin) nursing considerations
high alert med - causes harm if used incorrectly
teach mom and partner: why we use it, possible reactions (more intense contractions, longer peak, more regular and more often)
continue to tell her about her progress
women vary greatly in response to oxytocin
uterine response only takes 3-5 min after administered
oxytocin (pitocin) assessments
record uterine activity and FHR using EFM
evaluate at least every 15 minutes in 1st stage of labor and during passive fetal descent int he 2nd stage
5 minutes in the pushing (active) 2nd stage of labor
contractions should not occur any more frequently than 2 min
dose can be d/c or decreased by ROM and in active phase of 1st stage of labor
perform vaginal exams as indicated
oxytocin (pitocin) documentation should include ?
any time the oxytocin infusion has begun and each time it is increased, decreased or d/c
assessment data
interventions for tachystole and abnormal FHR
notification of OB and their response
s/s of uterine tachystole with pitocin
more than 5 contractions in 10 min (averaged over 30 min)
contractions that are 2 min or longer
insufficient resting tone between contractions
or intramnitoic pressure greater than 25mmHG between contractions measured via IUPC
Interventions for tachystole with normal FHR
reposition to sidelying
IV fluid bolus (at least 500ml of LR)
decrease oxytocin by at least half if uterine activity has not returned to normal in 10-15 minutes
if another 10-15 minutes goes by d/c oxytocin until contractions are lees than 5 in 10 minutes
Interventions for tachystole with abnormal FHR
d/c oxytocin immediately
reposition to sidelying
IV fluid bolus (at least 500ml of LR)
consider giving O2 at 10L/min via nonrebreather mask if above interventions fail
still no response after O2, give terbutaline 0.25mg Sub Q
Notify OB of actions taken and maternal/fetal response
resuming oxytocin after tachystole is resolved
if oxytocin was d/c for less than 20-30min, resume at no more than half the previous rate
if oxytocin was d/c for more than 30-40min, resume at initial dose