Micro E2 study guide pt. 1
1/102
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
103 Terms
What are the different methods of phenotypic bacterial identification?
macroscopic morphology, microscopic morphology, physiological/biochemical characteristics, chemical analysis
How does macroscopic morphology identify microorganisms? List examples.
colony appearance: texture, shape, size and shape, pigment, growth requirements
ex: direct antigen, DNA typing, rapid pathogen identification
How does microscopic morphology identify microorganisms? List examples.
fresh or stained microorganisms from specimen; shape, size, stain rxn, cell structure
ex: gram stain, acid fast stain, fluorescent ab stain, gene probes, FISH testing
How does physiological / biochemical characteristics identify microorganisms?
detects presence or absence of enzymes or metabolic pathways
How does chemical analysis identify microorganisms?
analyze specific chemical composition: cell wall peptides, cell membrane lipid
What differentiates a positive from a negative biochemical test?
the presence of an end product
positive = enzyme present (product formed)
negative = enzyme absent (no product formed)
What is the catalase test? What reaction occurs if biochemical test is positive? which gram positive bacteria is this test the main differentiator for?
tests for the presence of catalase which breaks down hydrogen peroxide into water and oxygen
bacteria is mixed in with hydrogen peroxide; if bubbles appear = catalase positive; no bubbles = catalase negative
staph and strep
What tests for the main biochemical differentiation between the gram positive bacteria staph and strep?
Catalase test
What does the oxidase test evaluate for?
tests for respiratory enzyme cytochrome oxidase (positive test = blue)
What does it mean when a bacterium is oxidase positive?
microorganism is aerobic, but does not have to be a strict aerobe
(negative = Anaerobic or Aerobe that uses a different oxidase than cytochrome C)
What does a coagulase test differentiate? Which staphylococcus species will clot on a coagulase test?
differentiates S. aureus from other staph species; S. aureus will clot.
(S. intermedius is also coagulase positive; but human infections are rare)
What does the genotypic test FISH stand for? What is visualized in a positive rxn?
Fluorescent in situ hybridization; provides rapid identification of unknown microbes
if cells in unknown sample contain target DNA or RNA, they will fluoresce = positive rxn and identification is made
Which genotypic test would best analyze a food poisoning outbreak?
pulse field gel electrophoresis PFGE
(restriction endonuclease create DNA profile of large sections of the bacterial genome; profiles of several isolates can be compared to determine if they came from same organism)
PCR tests amplify segments of DNA. If the sample being analyzed contains primarily RNA, what is used to produce a DNA template from the RNA? What is this test called?
reverse transcriptase will convert the RNA to DNA, and the DNA can then be amplified by PCR (RT-PCR)
What are serological tests based on? What are visible endpoints of these rxns?
antibodies binding specifically to an antigen; visible by clumps, precipitates, color changes, or release of radioactivity
What is observed when antibodies and antigens bind in an agglutination test? List common examples.
visible clumps;
Ex: ABO & Rh blood grouping, tube agglutination test (tidal test for salmonellosis), RPR for syphilis (treponema pallidum), cold agglutination for abs that react at lower temps (mycoplasma pneumonia)
What is observed when antibodies and antigens bind in a precipitation test? what type of medium are these tests typically performed on and why??
noticeable clumps or precipitates (cloudy zone);
carried out on agar gels bc precipitate easily disrupted in liquid media
What determines the band intensity on a western blot test?
amount of antibodies in pt’s serum (small amt yields light band; large amt yields dark band)
What generation is the current standard for HIV testing? What antibodies does this test evaluate for? How soon is the p24 antigen detectable after exposure?
immunoassay (HIV 4th gen test); evaluates for antibodies formed against HIV-1, HIV-2, and the p24; p24 detectable 14 days after exposure
What type of hemolysis is complement fixation based on? What represents a positive result and negative result?
lysin-mediated hemolysis;
positive = NO hemolysis occurs; complement was used by the immune complex in the first step, and Ab and Ag were a match (ab-ag complex present)
negative = hemolysis DOES occur; complement interacted w/ sheep RBCs and there was no immune complex formed b/t Ab and Ag during first step- no match; no ab ag rxn occurred
What does the ASO titer measure? What infections is this test best used?
levels of ab against streptolysin toxin (hemolysin made by GAS)
dx rheumatic fever, bacterial endocarditis, glomerulonephritis
What is the difference b/t direct and indirect fluorescent antibody testing?
direct- unknown ag from pt is mixed w/ known ab
indirect- known ag mixed w/ test serum composed of unknown ab content from pt’s serum
What does ELISA stand for? list the different types of ELISA
enzyme linked immunosorbent assay (relies on enzyme mediated color change to indicate binding of ab to ag);
direct, indirect, capture “sandwich”
How many screening antibodies are needed for direct ELISA?
only enzyme labeled primary antibodies; secondary antibodies are not needed
How many screening antibodies are needed for indirect ELISA?
both primary and secondary antibodies are used
Which ELISA has the highest sensitivity and is the most commonly used?
capture / “sandwich”
Between indirect and direct ELISA, which has a higher sensitivity? What is the main disadvantage of this type of ELISA?
indirect ; risk of cross-reactivity b/t secondary detection of abs
What is in-vivo serological testing? give examples
antigens introduced directly into body to determine presence or absence of antibodies → cell mediated rxn
ex: TB skin test, allergy testing, fungal testing
Why are gram positive and gram negative cocci referred to as pyogenic cocci?
due to the formation of pus caused by them
Which areas of the body are gram positive and gram negative cocci considered normal flora?
skin, oral cavity, and GI tract
Describe the morphology of staphylococcus
gram positive cocci in irregular grape like clusters; facultative anaerobic organisms
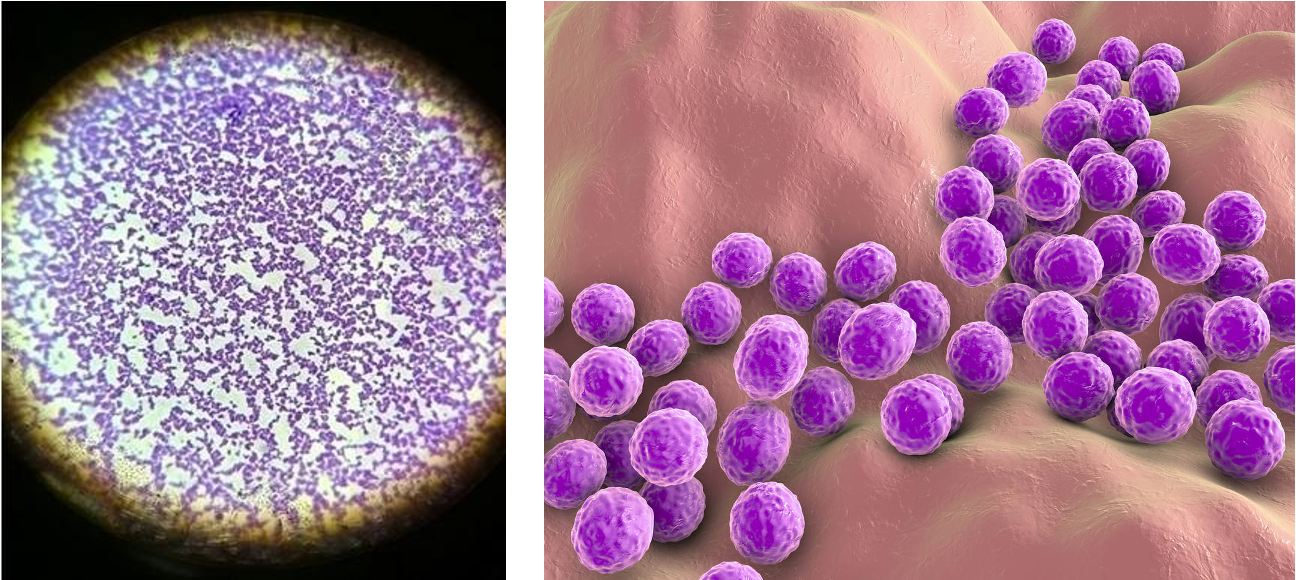
Which staphylococcus species is the most virulent?
s. aureus
Which biochemical test differentiates s. aureus from other species of staphylococcus?
coagulase test
Which biochemical test differentiates staphylococcus from streptococcus?
catalase test
List the toxins produced by s. aureus. which toxin lyses neutrophils and macrophages?
leukocidin (lyses neutrophils and macrophages), enterotoxin, exfoliative toxin, toxic shock syndrome toxin, hemolysins
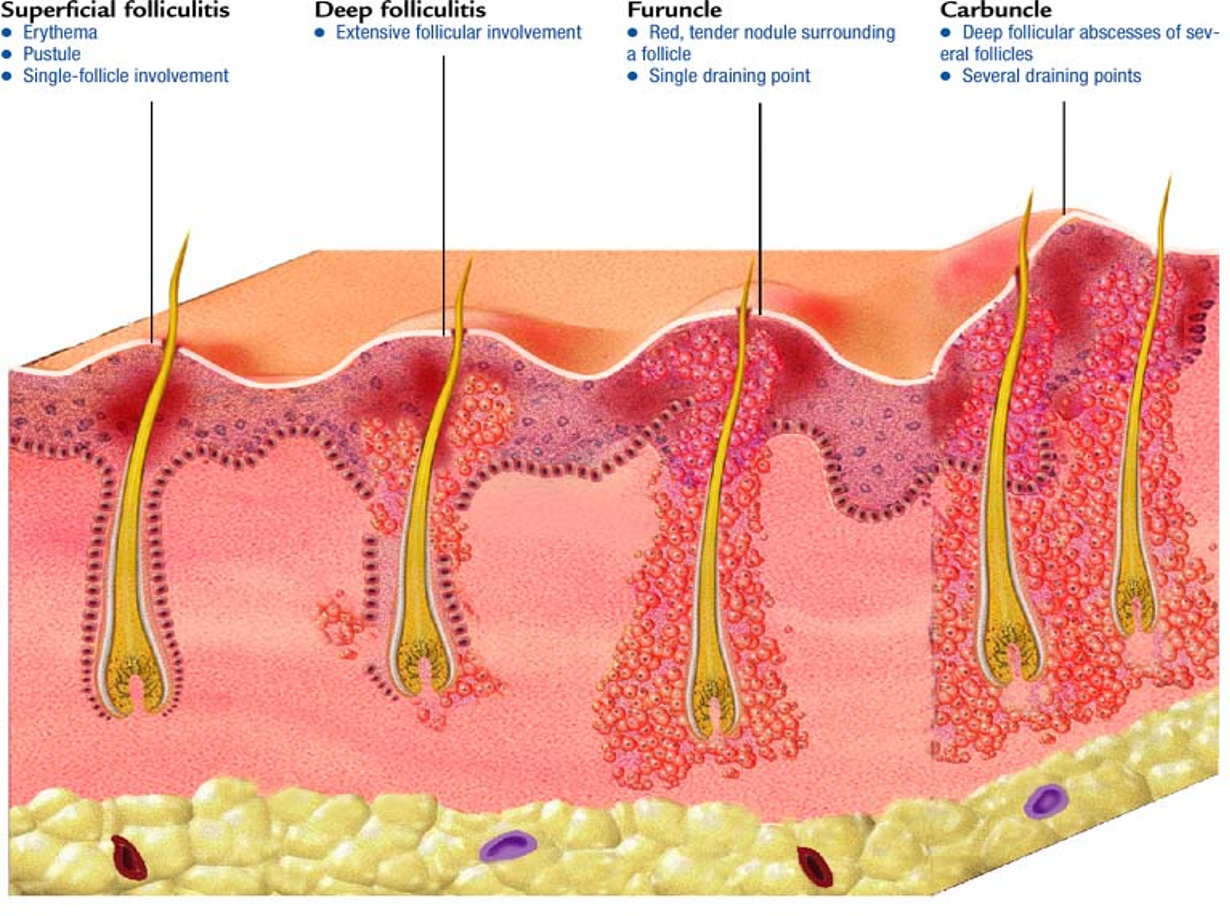
What is folliculitis? What are the non-pharmacologic tx for this condition?
superficial (epidermis) infection of hair follicles;
usually resolves on its own w/ sx care- warm compresses TID, avoid shaving

What is a furuncle/boil?
deep (epidermis, dermis, SC) infection of hair follicle or sebaceous gland; progresses into abscess or pustule

What are the predisposing factors and most common locations of a furuncle?
folliculitis, areas of skin w/ hair follicles that are exposed to friction/perspiration
nape of neck, back, buttocks, groin/thigh
What are common signs and sx of a furuncle?
erythematous, tender, inflammatory nodules that become fluctuant and may drain purple exudate; painful w/ pressure;
constitutional sx and fever are uncommon
What is a carbuncle? What does the treatment consist of?
multiple interconnected furuncles;
I&D + abx w/ activity against s. aureus (same as furuncle)

What are the signs and symptoms of a carbuncle?
large, erythematous, fluctuant, extremely painful area
What is the most common organism associated w/ these infections?
staphylococcus aureus
What is the best location to swab when testing for MRSA in preoperative patients? What is the decolonizing regimen for individuals who test positive?
anterior nares; intranasal mupirocin
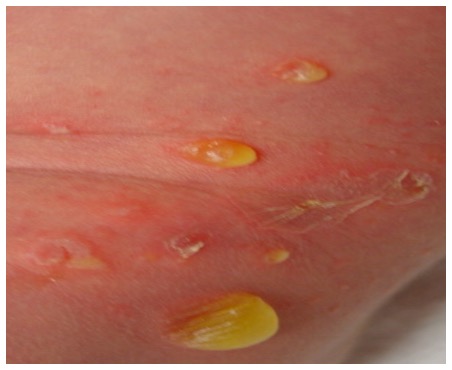
What is bullous impetigo?
vesicles that fill w/ yellow fluid, commonly on the trunk;
highly contagious; most common ages 2-5; s. aureus
What is non-bullous impetigo?
honey crusted plaques that spreads first to/from the nose; highly contagious; most common ages 2-5
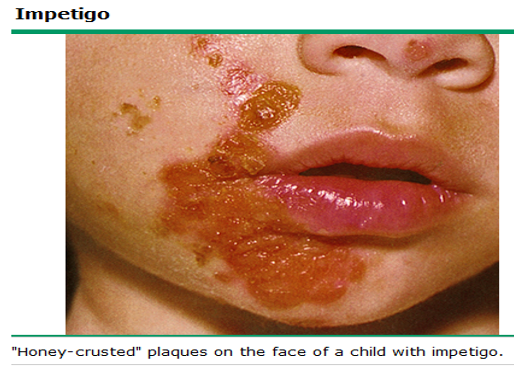
What is the second most common organism associated with non-bullous impetigo after S. aureus?
Group A B-hemolytic streptococcus / strep pyogenes
What is the recommended topical tx for non-bullous impetigo? What are the contact precautions, and when can a child return to school?
mupirocin TID x 5 days (bacitracin and neomycin NOT recommended)
contact precautions >24 hrs on abx, then can return to school
What are the risk factors for developing S. aureus bacteria?
hospitalized patients w/ chronic medical problems, injection drug use, recent skin and soft tissue infection, presence of FB (most common is intravascular catheter)
What are the 4 key components to treating S. aureus bacteria?
ID consultation, ABX, source control, repeat cultures until clearance
What is the recommended IV abx for MRSA bacteremia?
Vancomycin (alternative daptomycin)
What are janeway lesions?
painless, erythematous macule on palms of hands and soles of feet; sign of endocarditis
What are Osler nodes?
painful, erythematous nodules on fingers and toes; sign of endocarditis
What infection are janeway lesions and Osler nodes signs of?
endocarditis
What patient populations are at the highest risk for developing S. aureus osteomyelitis?
children, adolescents, and IV drug users (can also develop after a fracture or surgery)
What are sx associated w/ s. aureus osteomyelitis?
bone pain, fevers, chills, muscle spasms
Describe the onset and sx of food poisoning caused by S. aureus. Which type of toxin is responsible for these sx and what is the primary source of contamination?
rapid onset of acute sx of cramping, nausea, vomiting, and diarrhea that appear 2-6 hrs after ingestion and recover w/in 24 hours;
caused by preformed enterotoxins- carried by food handlers in their nose or on their hands
Which S. aureus toxin is responsible for scaled skin syndrome? What are sx associated w/ this condition?
exfoliative toxin
rapid, tender exfoliation of skin followed by re-epithelialization w/o any scarring; febrile, irritable; bull w/in 48 hours; desquamation (positive nikolsky’s sign)
What is nikolsky’s sign?
top layers of skin slip away from the lower layers when rubbed; indicates desquamation of staphylococcal scaled skin syndrome
What is the toxigenic disease associated w/ tampon use? What organisms cause this condition?
toxic shock syndrome caused by S. aureus and strep. pyogenes (group A strep)
What are the initial and late sx associated w/ TSS?
initial: rapid onset of diffuse red macular rash that starts on chest and feels like sandpaper, fever and flu like sx, hypotension
late: rash w/ desquamation of palms and soles, ulceration of vaginal mucosa, sepsis, altered mental status, multi system organ dysfunction
Which coagulase-negative staphylococci are commonly known to cause wound infections?
s. epidermis, s. hominis, s. capitis
Which coagulase-negative staphylococci are commonly known to cause UTIs?
s. epidermis and s. saprophytic
Describe the morphology of streptococci.
gram positive spherical / ovoid cocci in chains or pairs
non spore forming, non motile,
facultative anaerobes,
small, nonpigmented glistening colonies
What are the five species of streptococci associated w/ human disease?
s. pyogens (group A strep),
s. agalactiae (group B strep),
viridans strep,
s. pneumoniae,
enterococcus faecalis
What is the most resistant non-spore forming pathogen?
S. Aureus
Which test differentiates beta-hemolytic strep from group A and non-group A?
bacitracin test
Which species of group A strep is bacitracin sensitive?
S. pyogenes
Which test differentiates S. pneumoniae from other alpha-hemolytic strep species?
optochin test
Which bacitracin resistant beta hemolytic streptococci species does the CAMP factor test positively identify?
S. agalactiae
Which streptococcal species is highly virulent and commonly infects the throat, nasopharynx, and skin?
group A B-hemolytic streptococcus (GAS) / s. pyogenes
Besides erysipelas, impetigo, and strep throat, what other more severe diseases is caused by S. pyogenes (GAS)?
scarlet fever, rheumatic fever, acute glomerulonephritis, necrotizing fasciitis, streptococcal toxic shock syndrome
What is the clinical presentation of erysipelas?
painful, shiny, fiery bright red rash that is raised and well demarcated; non purulent; acute onset (mins-hrs);
most commonly on lower extremities, face will include nose and both cheeks most of the time

What is the typical clinical presentation of streptococcal pharyngitis? What other sx can be associated w/ this infection?
redness, enlarged tonsil, tenderness w/ swallowing, purulent exudates on tonsils
fever, HA, nausea, myalgias, tender cervical lymph nodes, abdominal pain, no cough
How do you document tonsillar swelling?
note the erythematous, edematous tonsils w/ exudates, palatal petechiae
1+ tonsils - take up <25% of space between pillars (occupy in the lateral dimension of the oropharynx)
2+ tonsils - take up b/w 25 and 50% of space between pillars
3+ tonsils - take up b/w 50 and 75% of space
4+ tonsils - 75% of space - kissing tonsils - narrowed airway -
What is scarlet fever a complication of? What is the clinical presentation? Where does the rash typically begin? Where will you not visualize the rash?
complication of strep pharyngitis caused by s. pyogenes;
bright red sandpaper like rash that covers body (scarlatina) and tongue dorsal w/ white exudate and projecting edematous papillae (strawberry tongue)
typically begins in axillae, groin, and neck and spares palms and soles
What is rheumatic fever?
inflammatory autoimmune disease(thought to be triggered by s. pyogenes) causes delayed inflammation of the joints, heart, and SC tissues
what are the most common cardiac conditions caused by rheumatic fever?
rheumatic heart disease- mitral valve insufficiency, stenosis, regurgitation
Describe the urinary findings of an individual with strep-induced acute glomerulonephritis. What percentage of patients will develop end-stage renal disease?
hematuria, proteinuria, azotemia; 10-15%
List the alpha-hemolytic streptococci that belong to the viridans group.
streptococcus mutant, s. salivarius, s. sanguinis, s. anginosus, s. mitis
Which alpha-hemolytic streptococci of the viridans group is commonly associated with dental caries and tooth abscesses?
s. mutans (produces slime layers that adhere to teeth; basis for plaque)
Why are individuals with congenital heart disease, a history of endocarditis, or who have prosthetic cardiac valves given prophylactic antibiotics before dental procedures?
to prevent bacteremia and subacute endocarditis
What is subacute endocarditis?
blood-borne bacteria settle and grow on heart lining or valves, forming thick biofilms called vegetations which gradually grow and release masses of bacteria called emboli into circulation, which can block circulation and cause organ damage
What are the signs and symptoms of subacute endocarditis? What is the gold standard for diagnosis?
fever, new heart murmur, weight loss, anemia
TEE- transesophageal echocardiogram (NOT by positive blood culture alone)
What common infection does Streptococcus pneumoniae cause when it gains access to the middle ear by way of the eustachian tube? What otoscopic findings would you expect to see in this situation?
otitis media
redness and bulging of TM indicate acute inflammation and internal pressure of a middle ear infection
Streptococcus pneumoniae causes 60% of all bacterial cases of pneumonia and is the most frequent pathogen identified in Community-Acquired pneumonia. Which individuals are predisposed to this infection? What should all individuals >65 years have to prevent this infection?
young children, elderly, immune compromised, persons living in close quarters;
pneumovax (PPSV23) vaccine
List common signs and symptoms of bacterial community acquired pneumonia
pleuritic chest pain, cyanosis, hypoxia, purulent blood tinged (rust colored) sputum, crackles/rales on lung exam, chills, shaking, rapid breathing, fever
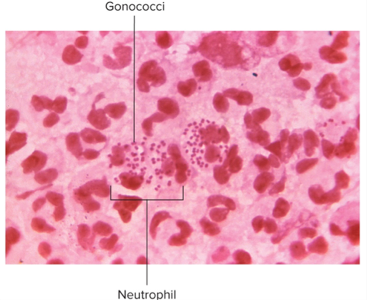
What two Neisseria species cause human infection? What is the morphology?
N. gonorrhoeae and N. meningitidis;
gram negative, bean shaped, diplococci; strict parasites that do not survive long outside of the host; aerobic or microaerophilic
What gender specific symptoms do men experience in gonorrhea?
urethritis, dysuria, yellowish discharge, scarring, infertility
What gender specific symptoms do women experience in gonorrhea?
urethritis, vaginitis, salpingitis (PID), mixed anaerobic abdominal infection, common cause of sterility and ectopic tubal pregnancies
What other STI is gonorrhea commonly associated with?
chlamydia
List the extragenital gonococcal infections we discussed in class.
proctitis, pharyngitis, gingivitis, conjunctivitis, chronic arthritis, rash on limbs, meningitis, endocarditis
Which extra genital gonococcal infection is most common in neonates?
gonococcal conjunctivitis
What is the CDC's recommended treatment for gonorrhea in adults without allergies who weigh less than 150kg?
single dose of 500 mg IM Ceftriaxone (Rocephin)
What is the CDC's recommended treatment for gonorrhea in adults without allergies who weigh more than 150kg?
single dose of 1g Ceftriaxone (Rocephin)
When treating gonorrhea, should you also treat them for chlamydia?
if it has not been excluded, yes - add doxycycline 100 mg BID for 7 days
Neisseria meningitidis(meningococcus) is one of the top three organisms associated with bacterial meningitis. (The other two are H. influenzae and S. pneumoniae.)
Which subgroups of young adults are most susceptible to meningococcal meningitis? What age group of young children are most commonly infected?
those who attend college, are in the military, live in close quarters;
6mos - 3yrs and 10-20 yrs
List signs and symptoms of meningococcal meningitis.
rapid onset of fever, sore throat, headache, stiff neck. convulsions, vomiting
severe cases- petechiae, delirium, cardiac failure, widespread ecchymosis, death
What are petechiae? Why do they develop in individuals with meningococcal meningitis?
endotoxin damages blood vessels leading to vascular collapse, hemorrhage, clotting disorders, and visible petechiae
What is the gold standard for diagnosis of meningococcal meningitis?
culture of CSF for identification and sensitivity (looking for gram negative diplococci)
Which third-generation cephalosporin is used for treatment of meningococcal meningitis?
IV Ceftriaxone (Rocephin) or IV Cefotaxime (Claforan); both cross blood brain barrier