GENDT830: Operative II Final ( Info Post-midterm)
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
What was often used to whiten teeth in the olden days?
limestone
eggshells
T/F: the teeth whitening market as increased drastically over the years in North America
TRUE
Extrinsic stains are located on the ___ of teeth
surface
How do you remove extrinsic stains?
mechanical means
Extrinsic stains can become ___ into the teeth over time if not removed
incorporated
Sources of Extrinsic Stains
wine
coffee
iron
fruits
smoking
Extrinsic Stain

Tobacco Stain

Iron Supplement Stain

Causes of Intrinsic Stains
aging
enamel microfractures
medications
excessive fluoride ingestion
medical
restorations
What is the most common cause of dark teeth?
aging
Tetracycline Stain
NEVER ADMINISTER TO PREGNANT WOMEN AND CHILDREN < 8 YO

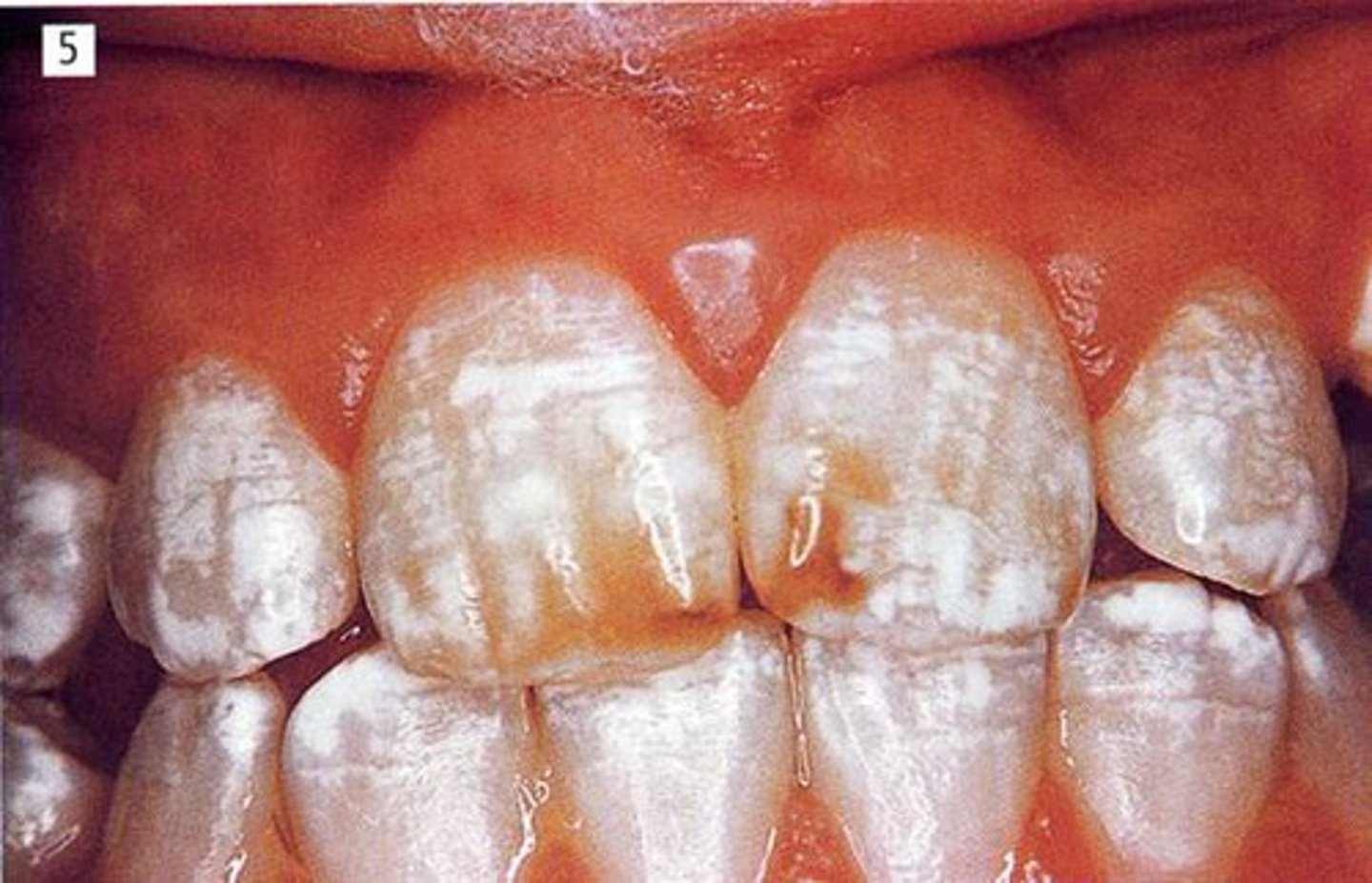
Fluorosis
too much F during amelogenesis--> porous enamel that is HYPOmineralized
Teeth Whitening Mechanism
H2O2 --> ROS --> high molecular weight molecules break down into smaller molecular weight molecules (lighter in color)
Chromophore
large stain molecule
Hydrogen Peroxide
Fast Action
Carbamide Peroxide
slow release
T/F: Carbamide Peroxide is very slow release up to 5 hours
TRUE
Which Peroxide is more likely to cause sensitivity?
Hydrogen Peroxide
In-Office Whitening
quick
high concentration
quick rebound
burns tissue
technique sensitive
need touch-ups
At-Home Trays
impression/scan
lower carbamide peroxide concentrations
last longer
less rebound
"touch-up" later
What whitening product does MUSC clinics use?
Opalescence
Non-Custom Whitening Kits
one size
inexpensive
good for teens
no dental supervision
misuse increases
Which brand is known to treat TETRACYCLINE STAINING?
Kor
Contraindications for Whitening
children with large pulps
cracks
exposed root
loss of enamel
pregnant/breastfeeding
hypersensitive teeth
decay
composite/porcelain restorations
T/F: You don't need radiographs when treatment planning whitening case
FALSE
2 Weeks 2 Treat
whitening should be done PRIOR to any esthetic restorative procedures and at least 2 weeks between whitening and restorative work as bonding is affected after whitening
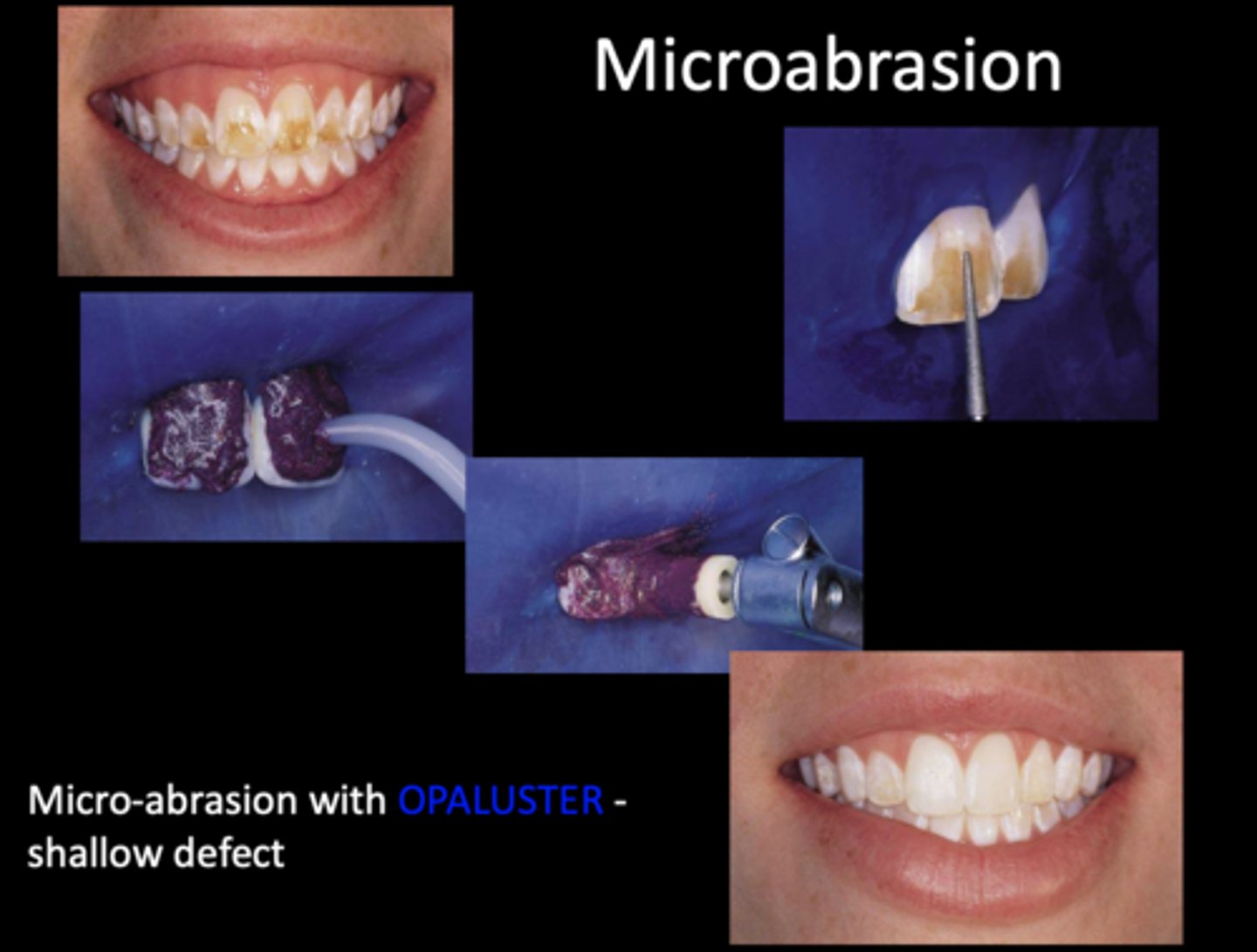
Microabrasion / Macroabrasion
Icon Resin Infiltration
acid/etch on white spots to light refract

What is the difference between extrinsic and intrinsic staining and causes of each?
Extrinsic stains are on the surface and caused by external substances
Intrinsic stains are within the tooth and caused by aging, medications, and systemic substances
What is the mechanism of action of whitening products?
the oxygenation of chromophores breaks down into smaller particles, resulting in lighter appearance
How does whitening affect bonding?
the free oxygen released by whitening hinders the polymerization of resin. Wait two weeks!
What are the types of whitening most commonly used and pros/cons of each?
In-Office: fast results/ quick rebound, expensive, increased chance of sensitivity
Take-Home Trays: slower results, less rebound, can touch up later/ takes longer, patient must be educated on tray placement and application of whitening gel
OTC: inexpensive, no dental visit requires, misuse
What is the difference between carbamide and hydrogen peroxide?
carbamide breaks down into hydrogen peroxide and urea , works slowly
There is a __:___ ratio of carbamide peroxide to hydrogen peroxide
3: 1
What is the most common side effect of whitening? How can you prevent/treat it?
sensitivity
use desensitizing toothpaste prior, decrease exposure time
What are alternatives to whitening?
microabrasion, macroabrasion, composite, porcelain restorations
What are the two components of glass ionomer?
Calcium Fluoroaluminosilicate glass
Polyacrylic Acid
Which type of reaction defines GI and RMGI? How log does it take to complete?
GIC: weak acid (poly acrylic acid) + base reaction 48 hours
RMGIC: polyacrylic acid + base glass + resin + camphorquinone. Light cure
What are the strengths of GI?
long term fluoride release
little to no net polymerization
shrinkage, moisture tolerant, self adhering w/ durable chemical bond
CTE the same as dentin
biocompatible
What are the weaknesses of GI?
vulnerable to fracture and can be difficult to handle (if you don't know how)
Know the steps of placing a GI
GIC: pumice, rinse, lightly dry. Activate capsule,. triturate, apply material, set, easy glaze, trim, easy glaze or Fuji coat
RMGIC: same, one less easy glaze or Coat & LC
What is the sandwich technique?
Open: glass ionomer exposed to the oral cavity
Closed: glass ionomer buried under other restorative material
GIC
conventional
self-cured
RMGIC
resin modified
light dual cured
Self Cure GIC brands
Triage
Fuji IX
RIVA
IonoStar Plus/Molar
Dual Cure RMGIC brands
Vitrebond
Fuji II LC
Riva LC
Ionolux
Polyacrylic Acid is a ___ acid
weak
Calcium Fluoroaluminosilicate Glass is a ___
base
The Glass Ionomer should include ___ too!
strontium
How GICs bond to tooth?
fuses to the tooth structure
bonds chemically
T/F: GIC and RMGIC create a hybrid layer
FALSE
***Create a interdiffusion zone
Composites methods of adhesion to the tooth
require a bonding agent
more esthetic
better physical properties
GIC methods of adhesion to the tooth
bonds to MOIST tooth
ultimately forma a union with the tooth
How long does GI take to "mature" ?
24-48 hours
initial acid pH --> demineralization
remineralization occurs with fluorapatite formation and fluoride release
T/F: GI can be bulk filled
TRUE
T/F: GI is bioactive
TRUE
GIC Strengths
release of fluoride
no polymerization shrinkage
moisture tolerant
durable chemical bond
CTE same as dentin
biocompatible
Ionic Bond of GI
-COOH from GI : Ca++ from Tooth
What is the shear bond strength of GI ionic bond?
8-10 MPa
What is the weakness of GI?
poor flexural strength
fracture toughness
wear resistance
What happens if there is too LITTLE water with GI? (application to a desiccated tooth)
inhibits GI maturation
failure
What happens if there is too MUCH water with GI?
GI absorbs excess water and SWELLS!!!
dilutes metal ions
T/F: GI require you to "coat" them with a resin based sealer both PRIOR to trimming and then AFTER all adjustments have been made to protect them from the impacts of moisture
TRUE
(does not apply when used as a liner)
Uses of GI
sealants
sedative restorations
high caries risk
liners/bases
pedo restorations
class V
NCCL
ART
Sealant GI Material
Fuji Triage
ART
Atraumatic Restorative Treatment
*only hand instruments*
RMGI is ___ ___
dual cured
1. acid/base reaction
2. LC via camphorquinone
Which teeth are best for RMGIC?
anterior teeth through 1st bicuspid with good isolation and esthetic demands
Which teeth are best for GIC?
second bicuspid to molars (poor isolation)
RMGI use an ___ resin on instrument
unfilled
GIC use __ on instrument
water
What is a bioactive material?
one that elicits a specific biological response at the interface of the material, which results in the formation of a bond between the tissues and the material
Bioactive Materials are __
dynamic
Examples of Materials with Potential for beneficial ion release
PulpDent
Septodont
Doxa
NovaMin
PulpDent
Bisco
Shofu
Biomineralization
how living organisms secrete inorganic minerals in an organized manner
Types of Bio-interactive Material
Biodentine
lime-lite enhanced
Activa Presto
NCCL
Non-Carious Cervical Lesions (Cervical Loss of Tooth Structure)

What contributes to NCCLs?
Cervical erosion
toothbrush abrasion
abfraction
**Star** Friction leads to wear via ___ (exogenous) and ___ (endogenous)
Abrasion
Attrition
**Star** Corrosion / Erosion leads to the manifestation of ____ or ____ degradation
chemical/ electrochemical
**Star** Stress (resulting in compression, flexure, and tension) leads to ___ and ___
microfracture
abfraction
Etiology of NCCL
multifactorial
Considerations for the etiology of NCCL
diet
habits
occlusion
Friction causes
dentrifice
toothbursh
oral habits
occlusion
Corrosion/ Erosion causes
medicinal
regurgitation
citrate content of saliva
idiopathic
*Star* Areas affected by NCCL
Facial/Lingual Surfaces
*Star* What is the most common tooth affected by NCCL?
maxillary premolars
Location of Erosion (Corrosion)
lingual, buccal, occlusal, incisal
Shape of Erosion
U shaped
Enamel surface of Erosion
smooth, polished
Margin of Erosion
smooth
Location of Abrasion
Buccal
Shape of Abrasion
wedge
groove
Enamel surface of Abrasion
smooth/ scratched
Margin of Abrasion
Sharp (but smooth)
Location of Abfraction
buccal
Shape of Abfraction
V shaped
Occlusal
Overlapping
multiple lesions
Enamel surface of Abfraction
Rough
Margin of Abfraction
Sharp
subgingival