Pharm 212 final
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
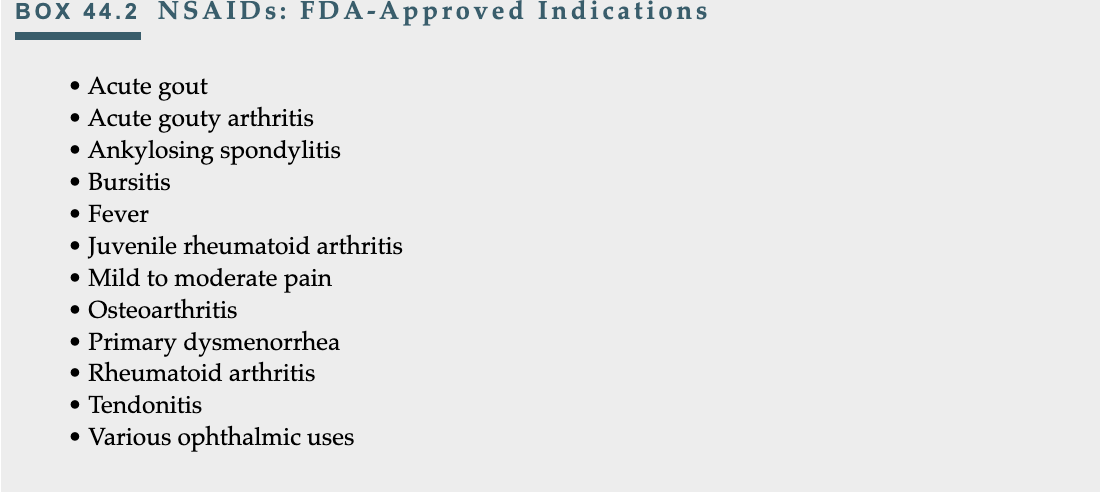
Nonsteroidal antiinflammatory drugs (NSAIDs) pain management
Indications
primarily used for analgesic, anti-inflammatory, & antipyretic effects, platelet inhibition
widely used for the treatment of rheumatoid arthritis
ceiling effect that limits their effectiveness
Risks
black box warning for CV(MI, stroke) and GI risk (bleeding, ulcers, perforation) except for aspirin
Nonsteroidal antiinflammatory drugs (NSAIDs) patient teaching pain management
CAUTION DRUMS
Cardiovacular effects
monitor for chest pain, sob, sudden weakness
Avoid alcohol
increases risk of gI bleed & liver damage
Understand “ceiling effect”
more pills doesn’t = more relief, effect is capped
it just increases more side effects
Tarry stools
report black tarry stools or emesis (bloody vomit)
Interactions
Always check before mixing with blood thiners or BP meds
On an empty stomach?
NO always take with food, milk, or antacids to protect lining
Not for everyone
considerations for pregancny, kidney, or liver disease
Don’t share
Report side effects
watch fro tinnitus, swelling, or blurred vision
Use for indication
treats pain, fever, inflammation
Maximize safety (follow dosing)
don’t exceed prescribed dose
Stomach irritation
can cause ulcers
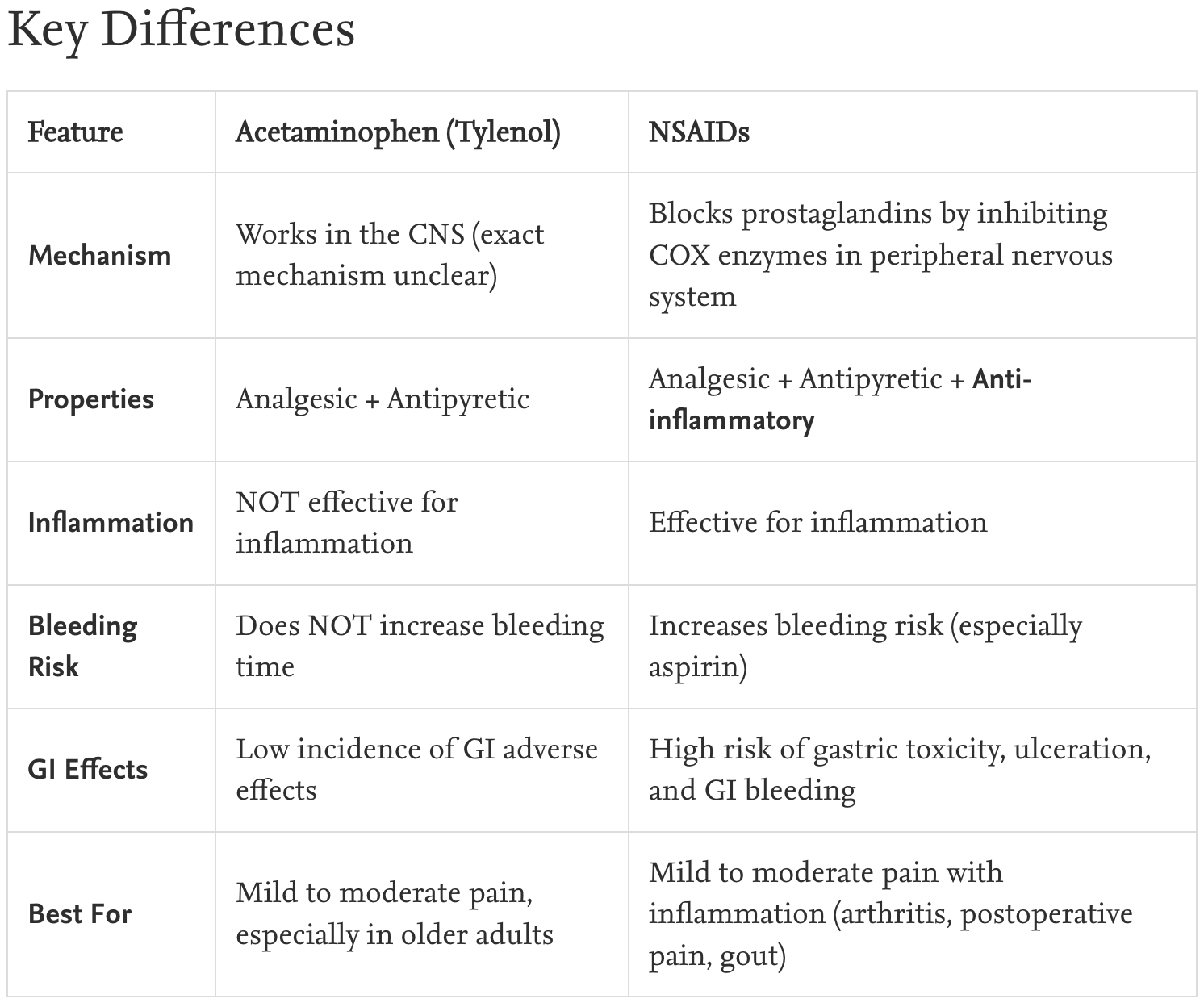
Tylenol vs NSAIDS pain management
Acetaminophen (tylenol)
analgesic choice for many
consider hepatic risks before admin
safer GI profile
no anti-inflmmatory effect
NSAIDs
examples; ibupuprofen, naproxen, keterolac
risk factors for adversre effect in >60 years, hx of pepetic ulcer, or CV disease
black box warning for risk of MI or stroke
want to use lowest dose for shortest time
Can be given together
Recommended for surgical patients
NSAID complications pain management
GI
gi bleed
melena or emesis
CV
BLACK WARNING BOX
MI or stoke
HF
Renal
acute renal failure
overdose toxicity
CNS effects
treated with activated charcoal
Bleeding risk
inhibit platelet aggregation (especially aspirin)
pt should stop taking 1 week before surgery
High risk patients
Age >60 years
History of peptic ulcer disease
History of cardiovascular disease
Dehydrated patients
Patients with vitamin K deficiency
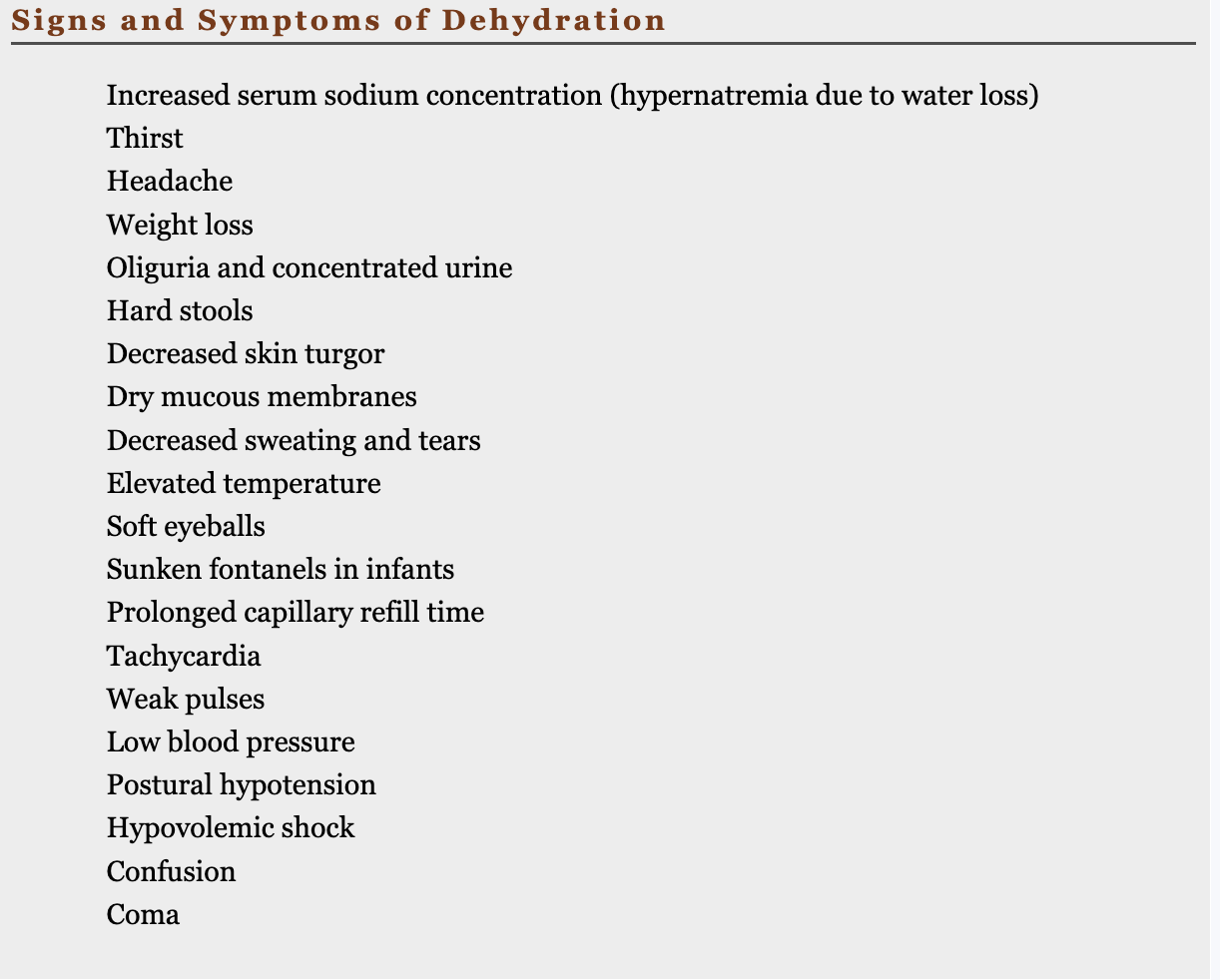
Dehydration diagnoses and cues Fluid and electrolytes
“I Think High Water Often Helps During Dry Episodes, So Some People Take Water Low, Providing Help Correcting Cells” for S/S
Priority nursing actions
Monitor:
Intake and output (I&O)
Daily weights
Vital signs with orthostatic measurements
Urine characteristics
Safety:
Fall precautions due to orthostatic hypotension and altered mental status
Fluid Replacement:
Oral rehydration solutions (ORS) for mild-moderate dehydration
IV crystalloids for severe dehydration or intolerance to oral fluids
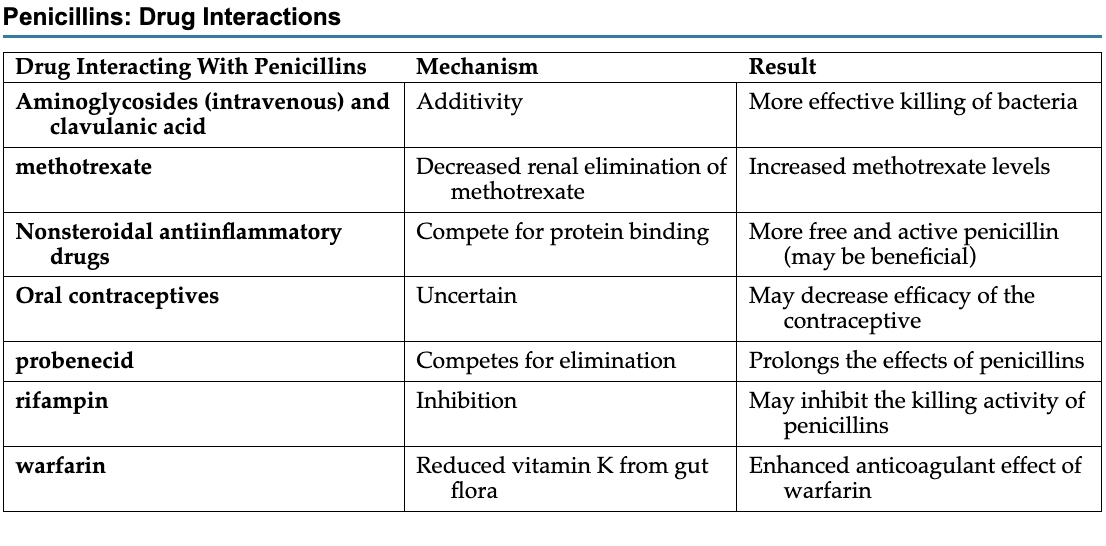
Penicillin drug interactions FINISH Antibiotics
classified as pregnancy category B drugs (very safe)
Nursing responsibilities when starting antibiotic therapy Antibiotics
Antibiotics have 3 uses
empiric (can best kill the microorganisms known to be the most common causes of the infection)
definitive (tailored to treat the identified organism by using the most narrow-spectrum, least toxic drug based on sensitivity results.)
prophylactic therapy
used to prevent an infection
"A Professional Learns Many Core Safety Actions."
A — Allergy History: Assess for hypersensitivity, ranging from mild rashes to severe anaphylaxis.
P — Physical Assessment before and after: Document age, weight, vitals, and neurological, GI, and immune status.
L — Laboratory/Diagnostic Studies: Review C&S, liver (AST/ALT), renal (BUN/Cr), cardiac, and blood counts.
M — Medication Review: Document all OTCs, herbals, and supplements; check for drug interactions.
C — Cultural Assessment: Consider ethnic responses to drugs and alternative healing practices.
S — Superinfection: Monitor for secondary infections (like fungal) due to flora destruction.
A — Antibiotic Resistance: Stay alert for resistance (like CRO), especially in pediatrics and facilities.
Tetracycline patient teaching Antibiotics
end in “cycline.”
choice of drugs to treat infections caused by Rickettsia, Chlamydia, and Mycoplasma
used to treat acne in teens/adults
Contraindiccations
known drug allergy, pregnancy, children younger than 8
“To Teach All Clients: Take Caution, Complete Daily Pills, Protect Personal Integument, Seek Speedy Vision Reports”)
Timing & Food
T — Take on an empty stomach (1h before/2h after).
T — Take with a full glass of water.
A — Avoid dairy, antacids, and iron (within 2 hours).
Consistency
C — Consistency: Take at evenly spaced intervals.
T — Total: Complete the full course of therapy.
C — Continuity: Do not skip doses.
Safety Information
D — Discoloration: Permanent yellow-brown tooth staining risk.
P — Pregnancy: Contraindicated (harms fetal bone/teeth).
P — Photosensitivity: Increased sensitivity to sunlight.
What to Report
I — Intracranial Pressure: Report severe headache or blurred vision.
S — Stomach: Report severe diarrhea or cramping (C.diff).
S — Superinfection: Report vaginal itching or discharge.
V — Visual: Report vision changes immediately.
R — Reaction: Report rash, hives, or difficulty breathing
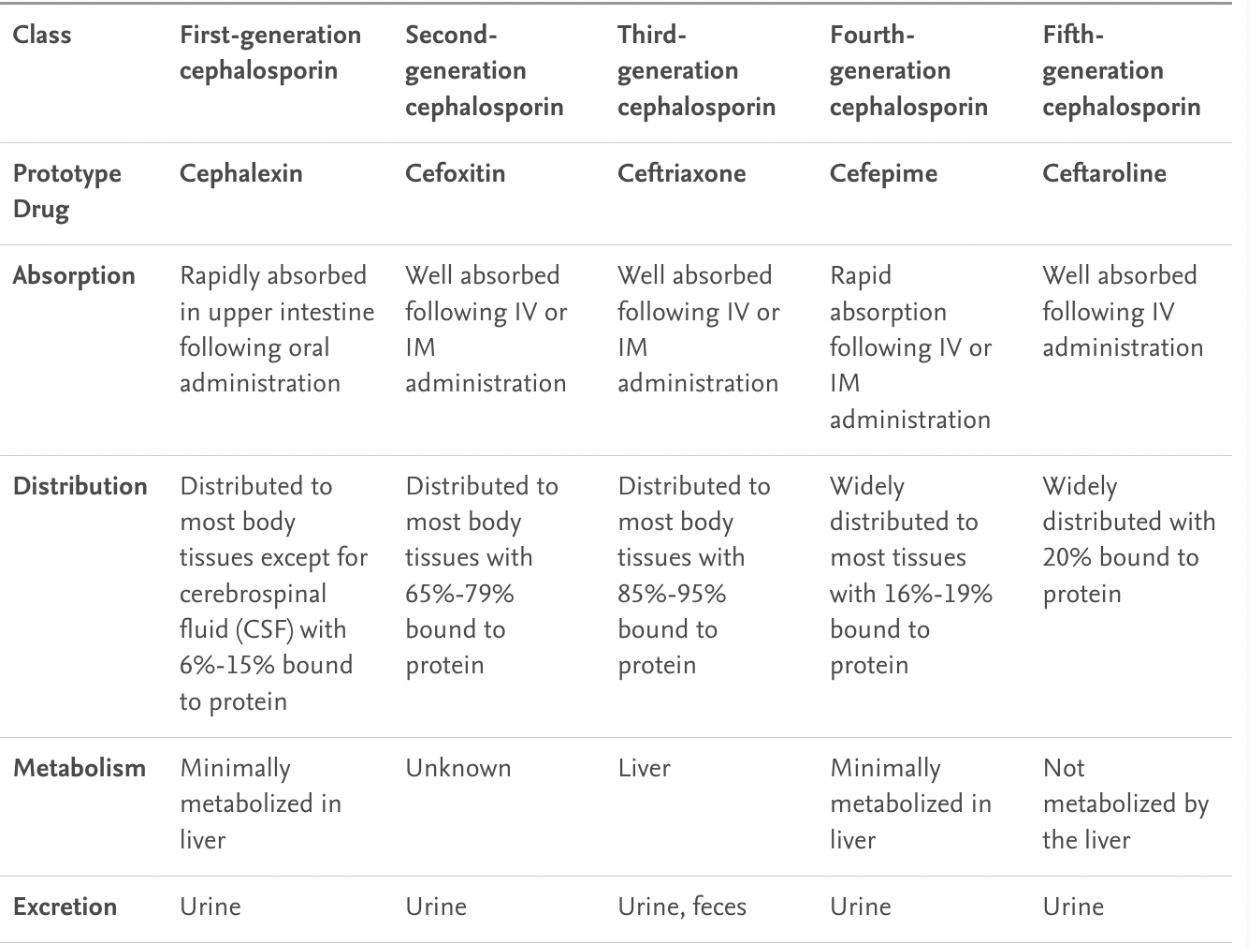
Cephalosporin contraindications finish later Antibiotics
penicillin allergies may have cross-sensitivity to cephalosporins
1-5 gens (cephalexin, cefoxitin, ceftriaxone, cefepime, ceftaroline)
Contraindications
hypersensitivity to cephalosporin or PCN,
jaundice
premature neonates
Antiseptic vs Disinfectant Antibiotics
Antiseptic
inhibits the growth and reproduction of microorganisms without killing them.
called static agents.
Disinfectant
applied to nonliving objects to kill microorganisms
called cidal agents.
Healthcare associated infection facts Antibiotics
infections acquired in the hospital hat were not present at time of admission.
Sources
Hands of healthcare workers
Medical tubes
Implants
Medical devices
Prevalence & Impact
Occur in 1 in 25 hospitalized patients
Cause increased healthcare costs and many deaths
preventable!!
Most Common Types
Urinary tract infections (UTIs)
Surgical site infections (SSIs)
Bloodstream infections - especially central-line-associated (CLABSIs)
Pneumonia - including hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP)
High-Risk Areas (immunocompromised)
Critical care units
Dialysis units
Oncology units
Transplant units
Burn units
Common causes
not following basic infection control
organisms are now multidrug-resistant
Best prevention = Hand washing
Aminoglycoside adverse effects Antibiotics
Nephrotoxicity (Kidney Damage)
Manifested by:
Urinary casts, Proteinuria, Increased BUN and CR
Risk increased with concurrent nephrotoxic drugs (cyclosporine, IV contrast for CT scans)
Ototoxicity (Ear Damage)
Often NOT reversible
Results from injury to CN VIII
Cochlear damage → hearing loss
Vestibular damage → disrupted balance
Symptoms include:
Dizziness
Tinnitus (ringing in ears)
Sense of fullness in the ears
Hearing loss
Other
Headache
Paresthesia
Vertigo
Skin rash
Fever
superinfection
Neuromuscular paralysis
-Neomycin patient teaching Antibiotics
ONLY oral aminoglycoside
used for preoperative bowel cleansing
other uses for for skin infections, bladder irrigation, and treatment of E. coli diarrhea, hepatic encephalopathy, and eye infections.
“Daily Hydration Can Tame Frequent Complications; Doctors Often Note Probiotics Yield Powerful Maintenance, Keeping Hearing Dependable”
Dosing
D — Duration: Do not skip doses or stop early
Hydration
H — Hydration: Drink plenty of fluids (up to 3000 mL/day).
What to Report Immediately
C — Change in hearing
T — Tinnitus: Ringing in the ears.
F — Full feeling: Pressure in the ears.
C — Changes in balance: Dizziness or vertigo.
D — Decreased urination: Changes in urine output.
Serious Risks
O — Ototoxicity: Permanent ear damage.
N — Nephrotoxicity: Kidney damage.
Preventing Superinfections
P — Preventing superinfections: Protect natural flora.
Y — Yogurt: Or buttermilk to maintain gut health.
P — Probiotics: Essential to avoid secondary infections.
Monitoring
M — Monitoring: Oversight of drug levels and health.
K — Kidney function tests: BUN and Creatinine.
H — Hearing tests: Needed for prolonged therapy.
D — Drug level monitoring: Checking peak and trough levels.
Treatment of MRSA Antibiotics
Antibiotic options
IV vancomycin
IV or oral linezolid
IV daptomycin
IV ceftaroline (only cephalopsorin approved)
Prolonged therapy often needed - more than 3 months
Community-Associated MRSA (CA-MRSA) Antibiotic options:
Minocycline (usually effective)
Doxycycline (usually effective)
Infection Prevention Measures
Nasal swabs and cultures for MRSA screening
Contact Precautions required
Bathing patients with chlorhexidine wipes
Administering nasal mupirocin ointment
Vancomycin infusion precautions Antibiotics
contraindicated in patients with a known hypersensitivity to it. It should be used with caution in those with preexisting renal dysfunction or hearing loss, as well as in older adult patients and neonates.
VANCO-SLOW
V - Vital signs (monitor BP - rapid infusion causes hypotension)
A - At least 1 hour infusion time (NEVER IV push)
N - Nephrotoxicity risk (ensure hydration og 2L fluids/day, monitor BUN/creatinine)
C - Compatibility check (multiple drug/diluent incompatibilities)
O - Ototoxicity monitoring (assess hearing, report ringing/roaring in ears)
S - Skin assessment (watch for red man syndrome - flushing of face, neck, upper trunk)
L - Levels - trough only (before 4th dose, within 30 min of next dose; goal 10-20 mcg/mL)
O - Over 1 hour minimum (slow infusion prevents red man syndrome)
W - Watch for reactions (if flushing occurs, SLOW the rate further)
Acyclovir indications/patient teaching Antiviral
applied every 3 hours, or six times daily, for 1 week
classified as a pregnancy category C drug
Indications
HSV-1 and HSV-2 infection, including genital herpes, mucocutaneous herpes, herpes encephalitis; herpes zoster (shingles); higher-dose therapy for acute episodes; lower-dose therapy for viral suppression
Adverse effects
Nausea, diarrhea, headache, burning when topically applied
Teaching
• don’t use in eyes or when there is no evidence of infection
• apply with glove to prevent further infection
• avoid use of OTC creams, ointments, lotions
• Advise hand washing before, after each application
• adhere strictly to regimen to maximize successful treatment
• Advise patient to begin taking product when symptoms arise
Oseltamivir indications/patient teaching Antiviral
Uses
Prevention and treatment of influenza type A or B
Contraindications
Hypersensitivity
Precautions: Pregnancy, neonates, infants, children, geriatric patients, renal/hepatic/pulmonary/cardiac disease, psychosis, viral infection
Teaching
• About all aspects of product therapy
• To avoid hazardous activities if dizziness occurs
• take as soon as symptoms appear; ake full course even if feeling better
• To take missed dose as soon as remembered if within 2 hr of next dose
• To stop immediately; to report to prescriber skin rash, delirium, psychosis, hallucinations (child)
• should not be substituted for flu shot
• will not treat the common cold
• To avoid other products
Oral thrush treatment Antifungal
Oral Thrush aka (Candidiasis)
Primary Treatment: Systemic Fluconazole
Oral fluconazole:
May be taken without regard to meals
Clear solutions only
IV fluconazole:
Use only if solution is clear
Protect from light
Diluted solutions stable for 24 hours only
Stop infusion immediately if itching or rash occurs; take vital signs and contact prescriber
Alternative Treatment: Nystatin
Nystatin is another antifungal option, available as:
Lozenges/Troches
Must be slowly and completely dissolved in mouth
Do NOT chew or swallow whole
Allows medication to coat affected areas
Oral Suspension
Swish thoroughly in mouth for as long as possible before swallowing
Maximizes contact with oral lesions
Miconazole schedule Antifungal
topical antifungal drug
inhibits the growth of several fungi, including dermatophytes and yeast, as well as gram-positive bacteria
For athlete’s foot, jock itch, ringworm, fungal infections are treated by
applying to cleansed, dry, infected area twice daily, in the morning and evening.
For treatment of yeast infections
one 200mg suppository is inserted into vagina once daily, at bedtime for 3 consecutive days
100mg administered intravaginally once daily at bedtime for 7 days
adverse effects
vulvovaginal burning and itching, pelvic cramps and rash, urticaria, stinging, and contact dermatitis.
pregnancy category C drug.
Fat and water soluble vitamins Vitamins
Fat soluable vitamins
Benzoyl peroxide Skin, hair, and nails
most common anti-acne drugs
effective in combating such infections because it slowly and continuously liberates active oxygen in the skin, resulting in antibacterial, antiseptic, drying, and keratolytic actions.
soften scales and loosen the outer horny layer of the skin are referred to as keratolytics.
pregnancy category C drug
-Diverticulitis -S/S to report SAT ??? Inflammatory bowel disease
represents inflammation of the diverticula and occurs in about 10% to 15% of cases of diverticulosis
cramping pain of the lower abdomen can accompany constriction of the thickened colonic muscles.
Diarrhea, constipation, distention, or flatulence may occur.
diverticula become inflamed or abscesses form, the individual develops fever, leukocytosis, and tenderness in the lower left quadrant.
-Pathophysiology of paralytic ileus redo Inflammatory bowel disease
cause of postoperative paralytic ileus remains unknown
-interaction between the autonomic and central nervous systems that disorganizes electrical activity and causes paralysis.
Antiemetics GI Disorder and therapy
meds used to treat N/V
chemotherapy, postop, or radiation induced N/V
hyperremsis gravidrum (pregnancy-related)
block receptors in the central nervous system (CNS), while some work directly in the gastrointestinal (GI) tract.
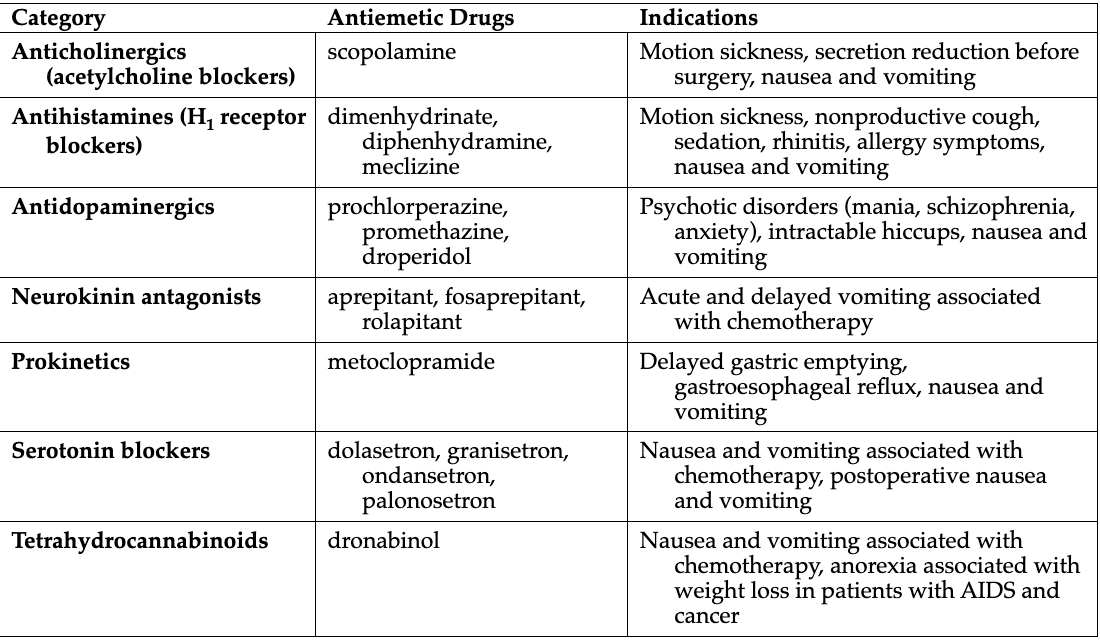
Different drug classes of antiemetics (7) GI Disorder and therapy
"All Anxious Actors Need Proper Stage Time"
All = Anticholinergics (scopolamine)
block receptors located in the reticular formation so that nausea-inducing signals can’t be trasnmitted
Anxious = Antihistamines (dimenhydrinate, diphenhydramine, meclizine)
prevent cholinergic stimulation
Actors = Antidopaminergics (prochlorperazine, promethazine, droperidol)
used for antipsychotic effects
Need = Neurokinin antagonists (aprepitant, fosaprepitant, rolapitant)
inhibit acute and delayed phases of chemotherapy-induced emesis.
Proper = Prokinetics (metoclopramide)
stimulate peristalsis in the GI tract. This enhances the emptying of stomach contents
Stage = Serotonin blockers (ondansetron, granisetron, dolasetron, palonosetron)
Time = Tetrahydrocannabinoids (dronabinol) THC
cause an alteration in mood and in the body’s perception of its surroundings,
Antiemetics and chemotherapy GI Disorder and therapy
Antiemetics are used to treat chemotherapy-induced nausea
give before chemo and neusea
continue even if n/v appears controlled
“SAN"
Serotonin Blockers (5-HT₃ antagonists)
Examples: Ondansetron, granisetron, dolasetron, palonosetron
Timing: Give 30-60 minutes before chemotherapy
Key role: First-line for CINV control
Adjunctive Agents
Dexamethasone (corticosteroid)
Lorazepam (anxiolytic) - Also blunts memory of the experience
Dronabinol (tetrahydrocannabinoid) - Give 1-3 hours before chemotherapy
Neurokinin Antagonists (NK₁)
Examples: Aprepitant, fosaprepitant, rolapitant
Use: Added for moderately and highly emetogenic regimens
Impact: Greatly improves CINV control
These work best in combination, especially for highly emetogenic chemotherapy.
-Peptic ulcer disease interaction warning GI Disorder and therapy
B = Bismuth + aspirin = salicylate overdose risk
black stools//tomhue are normal w bismuth
A = Alcohol - stimulates gastric acid secretion
N = NSAIDs - major contributor to ulcer formation
S = Smoking/tobacco - stimulates gastric acid secretion
P = PPI abrupt stop - causes rebound acid (step-down needed)
U = Uncrushable tablets (rabeprazole, pantoprazole - enteric-coated)
D = Don't forget corticosteroids increase ulcer risk
WARNING
"If you're taking bismuth (like Pepto-Bismol) for your ulcer treatment, NO ASPIRIN - it can cause a dangerous overdose!"
GERD treatment GI Disorder and therapy
Abnormalities in LES function, esophageal motility, and gastric motility or emptying can cause GERD
Nutrition Management
Foods to AVOID:
Decrease LES pressure: Peppermint, chocolate, fatty/fried foods, caffeine, carbonated beverages
Irritate inflamed tissue: Spicy foods, acidic foods (orange juice, tomatoes)
Eating Pattern Changes:
✓ Eat 4-6 small meals daily (not 3 large ones)
✓ Eat slowly and chew thoroughly
✓ Large meals increase stomach volume/pressure and delay emptying
Helpful apps: MyFitnessPal, MyPlate
Lifestyle Modifications
✓ Weight reduction
✓ Smoking cessation
✓ Elevate head of bed 6 inches
✓ Avoid tight clothing
✓ Eliminate drugs causing reflux (if possible):
Oral contraceptives
Anticholinergics
NSAIDs (ibuprofen)
Nitrates
Calcium channel blockers
Sedatives
Drug Therapy (Three Major Types)
1. Antacids
Neutralize stomach acid
2. H₂-Receptor Antagonists (Histamine Blockers)
Reduce acid production
3. Proton Pump Inhibitors (PPIs) ⭐ Agents of choice
Examples: Esomeprazole, pantoprazole, omeprazole
Benefits: Promote rapid tissue healing
IV form available for short-term use (stress ulcer prevention)
⚠ PPI Long-Term Use Risks:
Kidney, liver, cardiovascular disease
Dementia
GI tumors
Nutrient absorption difficulties
Increased susceptibility to respiratory/GI infections
Monitoring required during extended use
Recurrence common when stopped
4. Prokinetics
Example: Metoclopramide
Improves gastric emptying
Surgical Option
Laparoscopic fundoplication - Most common surgical treatment for severe cases
Use of bismuth subsalicylate GI Disorder and therapy
FOR Diarrhea management
an activated charcoal that coats walls of GI tract
Binds toxins and bacteria
Promotes elimination
will turn the stool black or gray.
Adverse effects
Increased bleeding time when combine with warfarin, aspirin, NSAIDs
constipation, dark stools, confusion, tinnitus, metallic taste, blue gums
risk for Reye’s syndrome, use cautiously in children & teenagers who are recovering from chickenpox or influenza
salicylate-based product, avoid other salicylates due to risk for toxicity
Asthma
chronic airway inflammation. It is
defined by hx of respiratory symptoms
wheeze, SOB, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation.”
Risk factors associated with adult-onset asthma prevalence include heredity factors, allergen exposure, changes in the microbiome, exposure to tobacco smoke and air pollution, occupational exposure, socioeconomic factors, diet, obesity, and certain medications.
Status asthmaticus s/s and treatment
Status asthmaticus is a severe, life-threatening acute episode of airway obstruction that intensifies once it begins and often doesn't respond to usual therapy.
Key clinical findings:
Extremely labored breathing
Wheezing
Use of accessory muscles for breathing
Distention of neck veins
Patient may be unable to speak more than a few words between breaths
Potential complications if not reversed:
Pneumothorax
Cardiac arrest
Respiratory arrest
Immediate Medications:
IV fluids
Potent systemic bronchodilators
Steroids
Epinephrine
Oxygen
Emergency Procedures:
emergency intubation
tracheotomy may be required
Once breathing improves
Control therapy drugs
Reliever drugs/rescue drugs
COPD
progressive respiratory disease characterized by airway obstruction that is not fully reversible
chronic bronchitis and emphysema.
S/S “COPD BREATH”
C - Cough (productive in chronic bronchitis, only with exacerbations in emphysema)
O - Orthopneic/tripod position (leaning forward, arms braced on knees)
P - Pursed-lip breathing (prevents airway collapse)
D - Dyspnea (on exertion → at rest as disease progresses)
B - Barrel chest (increased anteroposterior diameter)
R - Respiratory rate increased (tachypnea with prolonged expiration)
E - Enlarged neck muscles (from accessory muscle use)
A - Accessory muscles (used for ventilation)
T - Thin (muscle wasting in extremities, weight loss)
H - Hyperresonant chest (on percussion)
Genetic mutation for emphysema
involves alpha-1 antitrypsin (α₁-antitrypsin) deficiency.
enzyme that inhibits proteases—enzymes that break down lung tissue
suspected in individuals who:
Develop emphysema before age 40
Have never smoked but still develop emphysema
Have a family hx of early-onset lung disease
may also develop hepatic fibrosis (liver scarring)
smoking accelerates lung damage.
treatment: IV augmentation therapy using plasma-purified α₁-antitrypsin
Characteristic feature of emphysema
protease activity is increased and antiprotease activity is decreased
TRAPPED AIR
T - Tissue destruction (alveolar walls break down)
R - Recoil lost (elastic tissue can't spring back)
A - Alveoli enlarge (form bullae - big air spaces)
P - Proteases damage elastin
P - PaO₂ decreases (low oxygen in late stage)
E - Expiration difficult (air gets stuck)
D - Diaphragm flattens (hyperinflation pushes it down)
A - Accessory muscles needed (neck, chest, abdomen work hard)
I - Increased work of breathing
R - Respiratory acidosis (CO₂ retention in advanced disease)
"CUP" for emphysema types:
Centriacinar = Upper lungs
Panacinar = lower lungs (think "P" for "Pottom")
Cause of chronic bronchitis
SMOKER'S COUGH
S - Smoke (cigarette smoke is #1 cause!)
M - Mucus hypersecretion (thick, tenacious)
O - Obstruction of airways (especially on expiration)
K - Kick-starts inflammation (irritants trigger cascade)
E - Edema (mucosal swelling)
R - Respiratory acidosis (↑ PaCO₂)
S - Sputum production (productive cough)
C - Chronic cough (≥3 months/year for ≥2 years)
O - Organisms breed (mucus = infection risk)
U - Upregulation of mucus glands (↑ number and size)
G - Goblet cells increase
H - Hypoxemia (↓ PaO₂)
3 months of productive cough
2 consecutive years
= Chronic bronchitis diagnosis
Arterial blood gasses
Normal Values
pH: 7.35–7.45
PaCO₂: 35–45 mm Hg
PaO₂: 80–100 mm Hg
HCO₃⁻: 22–26 mEq/L
Respiratory = Opposite
Metabolic = Equal
Respiratory: pH and PaCO₂ move in opposite directions
↑ CO₂ = ↓ pH (acidosis)
↓ CO₂ = ↑ pH (alkalosis)
Metabolic: pH and HCO₃⁻ move in the same direction
↑ HCO₃⁻ = ↑ pH (alkalosis)
↓ HCO₃⁻ = ↓ pH (acidosis)
SaO₂: 95–100%
Tuberculosis cause
Mycobacterium tuberculosis (MTB)
charcterized by granulomas in the lungs
Tuberculosis-Related Injections
Purified protein derivative (PPD):
diagnostic injection given intradermally in doses of 5 tuberculin units (0.1 mL) to detect exposure to the tuberculosis
Bacille Calmette-Guérin (BCG):
vaccine injection from an inactivated strain of Mycobacterium bovis.
not normally used in US because the risk is not as high, is used in much of the world to vaccinate young children against tuberculosis.
does not prevent infection, but reduces
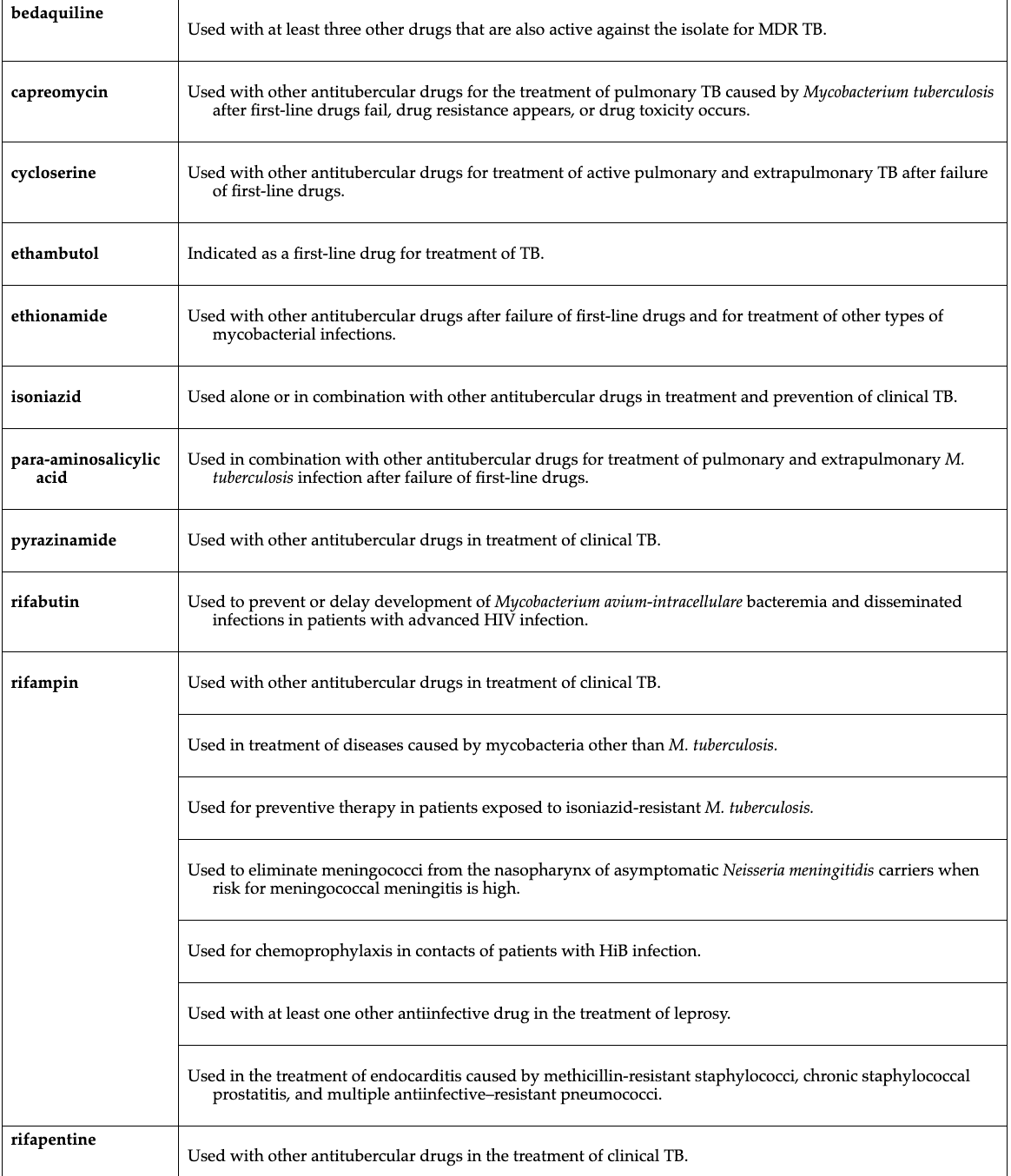
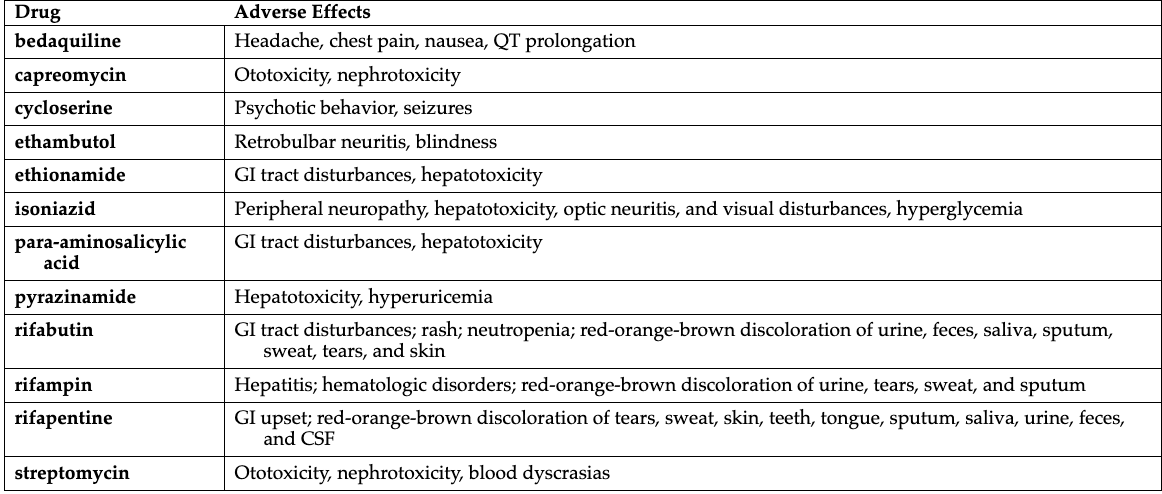
Tuberculosis treatment(1st and 2nd lines)
RIPE
First line drugs
Rifapentine
Isoniazid (INH): primary drug used
Pyrazinamide (PZA)
Ethambutol
Rifabutin
Rifampin
Streptomycin
"The fruit is RIPE for TB treatment"
INH is #1:
Think: Isoniazid = Important = Initial choice
Used alone for prophylaxis OR combined for active TB
All the "Rif-" drugs:
Rifampin, Rifabutin, Rifapentine = all rifamycins
They all turn body fluids orange-red
They're all enzyme inducers (drug interactions!)
Ethambutol = Eyes:
Ethambutol affects Eyes (optic neuritis)
Monitor vision regularly
PZA = Problem for liver:
Contraindicated in severe hepatic disease
BLOCK
2nd line drugs for (MDR-TB/XDR-TB)
B - Bedaquiline
For multidrug-resistant TB
Black box warning: QT prolongation, increased mortality
Must take with food
Avoid alcohol and QT-prolonging drugs
L - Levofloxacin
O - Ofloxacin
C - Cycloserine
K - Kanamycin
P - Para-aminosalicylic acid (PAS)
E - Ethionamide
K - Kapreomycin (Capreomycin)
Drug-Resistant TB
MDR-TB (Multidrug-Resistant):
Resistant to isoniazid AND rifampin
Requires second-line drugs
XDR-TB (Extensively Drug-Resistant):
Resistant to first-line AND best second-line drugs
Much less effective treatment options
Duration of TB treatment
Traditional Regimen: 6-9 months
RIPE: rifampin, Isoniazid, pyrazinamide, and ethambutol
Most common duration: 6 months
May extend to 9-12 months depending on severity and response
Typical schedule:
First 2 months: All 4 drugs (RIPE)
Next 4 months: Rifampin + isoniazid only
New Shortened Regimen: 4 months (2022)
rifapentine, Isoniazid, pyrazinamide, and moxifloxacin
Approved for drug-susceptible TB
Significantly reduces treatment burden
Drug-Resistant TB: Much Longer
MDR-TB and XDR-TB:
Requires higher doses for longer periods
Often 18-24 months or more
Uses second-line drugs with more side effects
Lower cure rates
Drug combinations purpose
1. Kill organisms as quickly as possible
Multiple drugs attack bacteria through different mechanisms
Faster bacterial elimination = faster symptom relief
2. Prevent drug resistance
Using multiple drugs simultaneously reduces the chance resistant strains will emerge
3. Most effective treatment method
TB antimicrobial medications
Antitubercular combination therapy priority teaching
Medication Adherence:
Take medications exactly as prescribed for the full duration
Don't stop early, even if you feel better
Skipping doses reduces effectiveness
Monitoring:
Attend all follow-up appointments to monitor progress
Report any concerning symptoms immediately
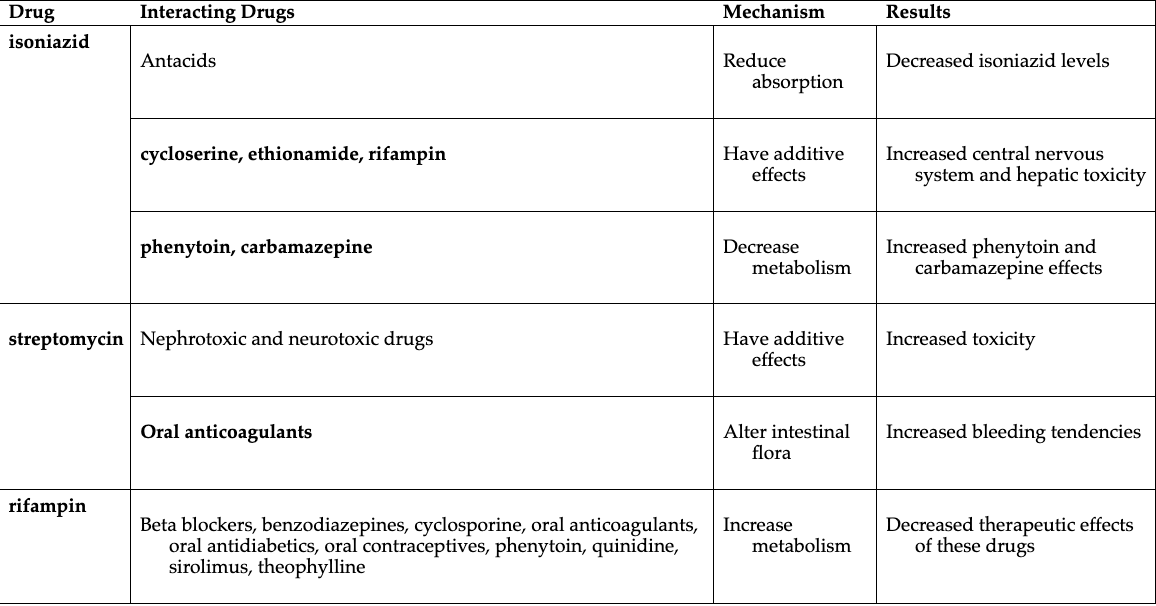
Drug Interactions:
Avoid antacids, phenytoin, carbamazepine, beta blockers, benzodiazepines, anticoagulants, antidiabetics, oral contraceptives, and theophylline
Get a complete interaction list before starting
Isoniazid Side Effects to Report:
Numbness/tingling in extremities
Abdominal pain, jaundice, vision changes
May need vitamin B6 supplementation
Rifampin Side Effects to Report:
Fever, nausea, vomiting, loss of appetite
Jaundice or unusual bleeding
General Tips:
Use sunscreen (photosensitivity risk)
Women on oral contraceptives need alternative birth control with rifampin
Practice good hygiene (hand washing, cover cough/sneeze)
Maintain rest, nutrition, and general health
Keep medications away from children
Wear medical alert identification
Isoniazid labs to be monitored
Isoniazid patient teaching
Bedaquiline indications and side effects
TB patient teaching
Antitussives Indications and mechanisms of action
Antitussives potential complications
What are 1st line drugs for nasal congestion
Patient teaching of an adrenergic decongestant
Antihistamines
Non-sedating histamines patient teaching
Antishitamine contrainidncations
Diphenhydramine patient teaching