Vascular Technology- 5th Edition Textbook
1/63
Earn XP
Description and Tags
Practice questions from Vascular Technology by Claudia Rumwell and Michalene McPharlin
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Which of the following deep veins is usually paired with another vein?
a. brachial vein
b. subclavian vein
c. femoral vein
d. popliteal
As blood flows through a stenosis, which of the following observations is most likely?
a. overall blood flow remains stable
b. kinetic energy is decreased
c. laminar flow is preserved
increased velocities are evident
Which statement below correctly describes transmural pressure (P)?
a. Transmural P is a measurement of the difference between the intraluminal P and the interstitial P.
b. Transmural P is a measurement of P inside the vein compared to P inside the artery.
c. Transmural P does not have an effect on the cross-sectional shape of the vein.
d. The higher the transmural P is, the lower is the intraluminal P.
A venous duplex study provides important information to help determine if venous ablation would be a viable treatment option for venous reflux. Which of the following factors is least important for a successful outcome?
a. caliber and depth of the vein
b. duration of the reflux
c. presence of venous stasis change
d. course of the vessel
A patient complains of aphasia, left hemiplegia with facial and arm weakness instead of (or more severe than) leg weakness, and behavioral changes. You suspect a blockage in which artery?
a. right middle cerebral artery
b. left anterior cerebral artery
c. vertebrobasilar vessels
d. bilateral posterior cerebral arteries
Angeriography reveals a stenotic right internal carotid artery with a residual lumen of 3 mm. If the true lumen is 9 mm, the diameter is:
a. 33%
b. 50%
c. 67%
d. 78%
For duplex scanning, the criterion for determining a >50% diameter reduction of the femoral artery is:
a. peak systolic velocity (PSV) of 150 cm/sec
b. prestenotic monophasic signal
c. ratio of stenotic to prestenotic PSV > 2:1
d. increased end-diastolic velocity >20%
Which of the following situations is least likely to results in a continuous-wave venouse Doppler exam that is falsely positive?
a. patient positioning
b. severe peripheral arterial occlusive disease
c. presence of bifid deep veins
d. obesity
The antecubital fossa is a triangular region located where in the body?
a. below the subclavian but anterior to the axillary artery
b. anterior to and below the elbow
c. medial to the major psoas muscle
d. distal to the knee but posterior to the fibular
Which of these statements is correct about primary Raynaud’s phenomenon?
a. it results from ischemia caused by distal arterial spasm
b. it relates to vasodilation of a healthy vessel
c. it can be the first manifestation of thromboangiitis obliterans
d. it is often evident after an acute arterial occlusion
What are the three branches of the aortic arch?
a. right subclavian, right common carotid, left common carotid
b. right subclavian, left common carotid, left subclavian
c. left common carotid, left subclavian, innominate
d. right common carotid, left common carotid, left subclavian
Which of the following vessels is not a branch of the opthalmic artery that exits the orbit?
a. supraorbital artery
b. nasal artery
c. infraorbital artery
d. frontal artery
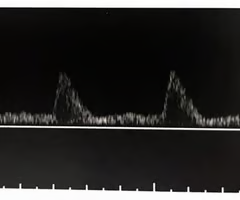
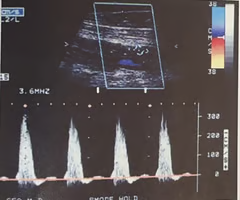
What would be the significance of finding this waveform in a peripheral artery?
A. Blood is flowing into a low-resistance vascular bed rather than the expected high-resistance bed
B. The arterioles of the distal vascular bed are vasoconstricted
C. This waveform is consistent with a distal occlusion
D. This flow pattern suggests a proximal arteriovenous fistula
A
Your department includes auscultation as part of your limited physical exam. Which of the following is true about that technique?
A. You can auscultate the aorta, femoral, popliteal, and tibial arteries
B. The absence of a bruit excludes disease
C. The presence of a bruit indicates turbulent flow
D. Auscultation provides an objective evaluation of blood flow patterns
C
Ms. Morris presents to the vascular lab for arterial testing because she has a six month history of pain in her calf muscles when she walks. If she has vascular disease, what is the most likely cause?
A. Atherosclerosis
B. Embolism
C. Thromboangiitis obliterans
D. Arteritis
E. Raynaud's phenomenon
A

What do these common femoral artery waveforms most likely represent?
A. Acute occlusion of the aorta
B. The waveforms are within normal limits and exclude proximal disease bilaterally
C. Believe the patient may have inflow disease in the right lower extremity
D. The waveforms are consistent with a distal embolism bilaterally
E. Believe the patient has Buerger's disease
C

Based on the waveforms, what is the most significant arterial disease of the left lower extremity?
A. Aortoiliac disease
B. Pop-infrapop occlusive disease
C. Outflow disease bilaterally
D. Tibial occlusive disease
B
Which of the following is an advantage with the four-cuff method of obtaining segmental pressures?
A. The high-thigh pressure more accurately reflects the patient's systemic blood pressure
B. The four pressure measurements are more reliable in the evaluation of a diabetic patient
C. The technique is better tolerated in the morbidly obese patient population
D. The method allows the ability to differentiate proximal superficial femoral artery (SFA) disease from distal SFA disease
D
With the three-cuff method, how should the thigh pressure compare to the brachial pressures to exclude proximal disease?
A. Expect the thigh pressures to be lower than the brachial pressures to exclude proximal disease
B. Thigh pressures are expected to be at lease 30 mmHg higher than the highest brachial pressure to indicate the absence of inflow disease
C. Thigh pressures are expected to be similar to brachial pressures in the absence of aortoiliac occlusive disease
D. The three-cuff method is not accurate in the evaluation of proximal disease when brachial pressures are high
C
After the brachial pressures have been obtained, which of the following represents the proper order of obtaining the lower extremity pressures?
A. The order can vary depending on the patient's comfort level
B. The proper order is proximal cuff to distal cuff on each extremity
C. The proper order is distal cuff to proximal cuff on each extremity
D. The order can vary from one extremity to the other depending on the vascular technologist / sonographer's preference
C
When interpreting segmental pressure measurements, which of the following factors is the least helpful?
A. Comparison of the most proximal pressure reading with the higher of the two brachial pressures
B. Evaluation of the pressure gradient between adjacent cuffs
C. Calculation of the ankle / brachial index
D. Identification of the horizontal pressure difference at the ankle level
D
Your next patient is a 35-year-old male, Mr. Nichols, who complains of pain in his feet with discoloration of his toes. Which of the following is the most significant of his risk factors?
A. He has high blood pressure
B. He smokes 3 packs of cigarettes a day
C. He has high cholesterol
D. He has a family history of cardiovascular disease
B
Based on your knowledge of Mr. Nichol's symptoms, as well as his risk factors, which of the following disease processes does he most likely have?
A. Chronic arterial occlusive disease
B. Acute arterial occlusion
C. Thromboangiitis obliterans
D. A vasospastic process, eg, Raynaud's
C
Your next patient, Ms. Peters, presents to your department with a bluish discoloration of her right big toe. All pulses are palpable. She denies any history of pain in her legs with activity or pain that wakes her up at night. She has no risk factors associated with arterial disease. What do you suspect is the most likely cause of her problem?
A. Atherosclerosis
B. Aneurysmal disease
C. Raynaud's phenomenon
D. Coarctation of the aorta
E. Thromboangiitis obliterans
B
Based on your assessment of Ms. Peters, what additional noninvasive testing might provide an explanation for her signs and symptoms?
A. Pressures before and after the treadmill
B. Duplex imaging
C. Tracings before and after immersing feet in cold water
D. Reactive hyperemia
E. Repeat tracings after wrapping toes in warm towels
B
What toe pressures would you likely obtain based on Ms. Peters' current history?
A. 110 mmHg on the right and 124 mmHg on the left
B. 90 mmHg on the great toes bilaterally
C. 86 mmHg on the great toes bilaterally
D. 0 mmHg on the right great toe and 94 mmHg on the left great toe
E. 28 mmHg on the right toe and 34 mmHg on the left
D
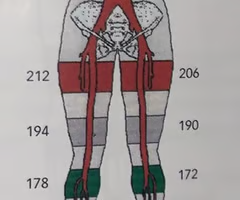
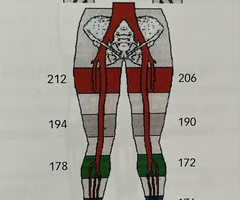
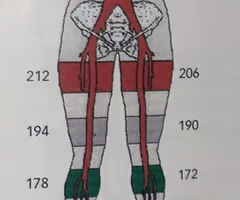
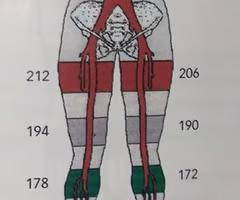
Calculate the ankle / brachial index (ABI) using the pressure measurements in the image:
A. Rt: 174/162 and Lt: 176/158
B. Rt: 174/158 and Lt: 176/162
C. Rt: 174/162 and Lt: 176/162
D. Rt: 178/158 and Lt: 172/162
C
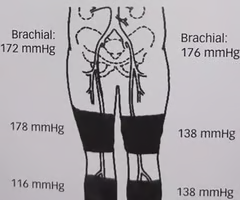
What is the significance of the thigh pressure in the image?
A. They indicate bilateral aortoiliac disease, left side greater than the right
B. The pressures are consistent with proximal disease on the left
C. This study demonstrates bilateral inflow disease
D. This patient has significant right common iliac disease
E. You suspect the patient has incompressible vessels
B
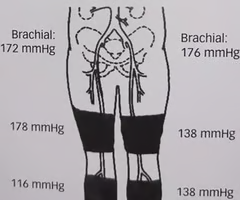
What information do the below-knee / calf pressure measurements in the image provide?
A. This patient has hemodynamically significant disease of the femoral-popliteal segment bilaterally
B. You suspect an occlusion of the left tibial arteries
C. Your patient has femoral-popliteal disease of the right lower extremity
D. The measurements exclude arterial occlusive disease
E. This patient has occluded popliteal arteries bilaterally
C
Your patient has been complaining of pain in his left calf every time he climbs a flight of stairs. Because the ABI was within normal limits, you will have the patient complete some form of exercise. Which of the following is lease likely to affect the decision to utilize a constant-load treadmill?
A. Recent history of severe cardiac arrhythmias
B. History of hyperlipidemia
C. A past total hip replacement resulting in a limp
D. The patient walks with a cane
E. 10-year history of severe hypertension
B
After completing the exercise study, you believe the patient has single-level arterial disease based on which of the following conclusions?
A. The patient takes 2 - 6 minutes to return to his pre-exercise pressures
B. Recovery time is 6 - 12 minutes
C. Recovery time is >12 minutes
D. The patient never returns
A
If your patient cannot walk on the treadmill, your protocol is to complete reactive hyperemia. Which of the following is true about that procedure?
A. It provides the same stress on peripheral circulation as a constant-load treadmill
B. 12 cm - wide ankle cuffs are inflated to 30 mmHg above the higher brachial pressure
C. The proximal cuffs are inflated per protocol and the high pressure is maintained for 1 - 3 minutes. Upon deflation of the cuffs, ankle/brachial indices are obtained
D. For normal response, an increase in the ankle pressure following cuff deflation must be evident
E. An abnormal response is 50% or greater decrease in the ankle pressure following the cuff deflation
E
Your next patient is scheduled for a coronary artery bypass graft (CABG), and the surgeon wants to use the right radial artery for the bypass. Which of the following is true about the test you will complete?
A. You will evaluate flow to the right digits, with the arm in a variety of positions to ensure the right radial artery can be used for the bypass
B. The most frequently performed test in this case is the modified Allen test, which determines the patency of the radial artery
C. You will evaluate flow to all of the right digits. If normal PPG waveforms are documented, no further action is required
D. During compression of the radial artery at the wrist, you document flow to digits #2 and / or #4. Maintenance of flow to the digits is the desired finding and allows the radial artery to be used for the bypass
D
As you evaluate the plethysmographic waveforms form a patient complaining of bilateral hip / thigh pain with activity, you notice the amplitudes of the waveforms are fairly normal but there is no notch on the downslope at any level bilaterally. What might these findings suggest?
A. This is an expected finding
B. The lack of reflection rules out vascular disease
C. The finding means the vessels are incompressible
D. The finding is likely based on the result of collateral arterial branches
D
A patient presents with left lower extremity claudication. The right lower extremity has normal plethysmographic waveforms and Doppler pressures. The exam results on the left show rounded, broad plethysmographic waveforms at the thigh level, which are similar in quality at the and ankle levels. The Doppler pressures are as follows: Bilateral Brachial = 150; Lt Thigh = 100; calf = 90; ankle = 90. These findings suggest:
A. Multilevel disease of the left lower extremity
B. Significant lesion of the aortoiliac system
C. Suspected left iliofemoral arterial obstructive disease
D. Suspected left tibial vessel arterial stenosis
C
Mrs. Emerson, 35 years old, presents with worsening bilateral finger pain. numbness and coldness, which she has experienced intermittently of the pas t 15 years. Bilateral digital PPG pressures and waveforms are obtained bother before and after cold stress. Before the cold, the waveforms have sharp upstroke, a narrow peak, and a reflection on the downslope. After cold, the waveforms change to a slow upstroke and downslope, a severely rounded peak, and disappearance of reflection on the downslope. These findings remain for 5 minutes after cold immersion. The post-cold waveforms are most consistent with:
A. Embolic process
B. Thromboangiitis obliterans
C. Primary Raynaud's
D. Phlegmasia cerulea dolens
E. Atherosclerosis
C
Your next patient, Mrs. Ricardo, is scheduled for a lower extremity bypass graft. Which of the following choices would make the most suitable bypass material?
A. A small saphenous vein that measures 1.5 mm x 1.8 mm
B. A great saphenous vein with a diameter of 3.2 mm x 3.4 mm
C. A cephalic vein that measures 1.9 mm x 1.9 mm
D. A basilic vein with a diameter of 1.6 mm x 1.8 mm
E. A femoral vein measuring 2.4 mm x 2.6 mm
B
A 71-year-old male presents to the vascular laboratory for the immediate postoperative evaluation of his right femoral-posterior tibial reverse saphenous vein bypass graft. At rest, the ankle / brachial index is 0.92. The biphasic Doppler velocities are 85 cm / sec in the native common femoral artery, 100 cm / sec in the proximal anastomosis, and 50 cm / sec at the knee posterior tibial artery. No post stenotic turbulence is observed. What is the most likely cause of the decrease in velocities?
A. Proximal obstruction
B. Collaterization
C. Arteriovenous fistula
D. Increase in graft diameter
D
IF the peak systolic velocity (PSV) in the region of stenosis is measured at 300 cm / sec, what would the prestenotic PSVs have to be for this stenosis to be considered >75% diameter reduction?
A. 150 cm / sec
B. 400 cm / sec
C. 75 cm / sec
D. 200 cm / sec
C
What would your preliminary report include if your next patient has the upper extremity pressure measurements shown in the image?
A. The pressures are consistent with a right subclavian / axillary stenosis
B. You suspect the patient may have occlusive disease involving the aortic arch
C. Although pressures in the right upper extremity are slightly reduced, they are still considered to be within normal limits
D. This patient may have some type of obstructive process in the right radial and ulnar arteries
D
Your next patient, Mr. Richards, is being evaluated for impotency. Which of the following noninvasive studies is least helpful in this situation?
A. Obtain plethysmographic recording at the thigh, calf, ankle, and toe levels bilaterally
B. Document Doppler waveforms of the common femoral artery, posterior tibial artery, and dorsalis pedis artery bilaterally
C. Use the Doppler to obtain ankle / brachial indices
D. Obtain penile pressures with either PPG or Doppler
E. Calculate the penile / brachial index
A
Mr. Richards has an ABI of 0.8 bilaterally using both the posterior and tibial artery and dorsalis pedis artery, with a penile / brachial index (PBI) of 0.38. What is your impression of these findings?
A. Mr. Richards has some large-vessel disease, but his PBI is within normal limits
B. Mr. Richards may be impotent due to vascular disease of his aortoiliac arteries
C. You suspect blockage of the vessels feeding the penis but can exclude more proximal disease
D. The PBI rules out poor blood flow to the penis as a source of the problem
E. Mr. Richards has a vacsculogenic impotence from internal iliac artery occlusive disease
B
A 32-year-old male presents to your diagnostic facility to evaluate pain in his right calf while jogging. His risk factors include hypertension and hyperlipidemia. He has a 15-year history of smoking two packs of cigarettes a day. What do you suspect is the most likely basis of his symptoms?
A. Popliteal artery entrapment
B. Atherosclerosis
C. Thromboangiitis
D. An embolic process
E. Cystic advential disease
A
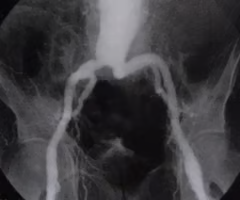
What pathology is evident in the image?
A. Aortoiliac occlusive disease (AIOD)
B. Infrarenal abdominal aneurysm
C. Coarctation of the aorta
D. Fibromuscular dysplasia (FMD)
E. Pseudoaneurysm of the distal aorta
B
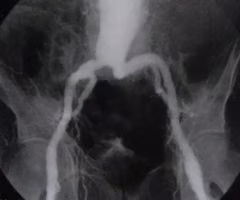
Of the following choices, what is the most frequent complication from the disease process represented in the image?
A. Vasospasm
B. Rupture
C. Acute occlusion
D. Compartment syndrome
B
Mr. Deeds is status post endovascular repair of his abdominal aortic aneurysm. Which of the following findings in the post-op surveillance duplex requires attention?
A. Peak systolic velocity of 76 cm/sec in the aorta proximal to the endovascular graft
B. Biphasic Doppler signals throughout the endograft
C. Unchanged amount and contour of mural thrombus in the aneurysmal sac
D. Complete color filling in the iliac branches of the stent
E. Increasing size of the aneurysmal sac
E
A referring physician asks you to document just the flow velocities in the dialysis graft, rather than performing a complete evaluation. What is the significance of a peak systolic velocity of 85 cm/sec in this case?
A. This is normal flow for a dialysis graft
B. You suspect the patient has an arterial inflow problem
C. This is accelerated flow and is consistent with graft stenosis
D. You are concerned that the graft is too large and shunting too much blood from the patient's arterial system into the venous system
B
If peak systolic velocities are >400 cm/sec in the superficial femoral artery, the probable diameter reduction is:
A. <50%
B. 50%
C. =>75%
D. =>90%
C
As you evaluate a reversed saphenous vein bypass graft, which of the following findings is considered to be within normal limits postoperatively?
A. ABI is reduced by >0.15 compared to previous exam
B. Some retrograde Doppler flow in the native vessel at the distal anastomosis
C. A peak systolic velocity of 384 cm/sec is evident at the proximal anastomosis
D. Decreased PSVs that are evident in the smallest graft diameter
B
Your next patient is a thin, frail-looking 90-year-old female scheduled for an abdominal duplex. As you begin her evaluation, which transducer will you most likely choose to start the exam?
A. 10 MHz CW probe
B. Higher frequency curved array
C. Lower frequency curved array
D. Lower frequency phased array
B
Which of the following qualities is most consistent with an abdominal aortic aneurysm?
A. A diameter measurement of >3 cm
B. An increase in diameter of 25%
C. A longitudinal measurement of 5 cm
D. A diameter measurement of <2 cm
E. A longitudinal measurement of >3 cm
A
High-resistance flow patterns are expected in which of the following arteries?
A. Preprandial superior mesenteric artery
B. Postprandial celiac artery
C. Renal arteries
D. Preprandial hepatic artery
E. Splenic artery
A
What would be the significance of finding PSVs of 48 cm/sec in the aorta and 172 cm/sec in the left renal artery?
A. Consistent with a 50% diameter reduction of the left renal artery
B. Within normal limits
C. Documents a = or > 60% diameter reduction of the left renal artery
D. Consistent with a = or > 70% diameter reduction of the left renal artery
E. Suggests a 30% diameter reduction of the left renal artery
C
As you evaluate the cause for the flow acceleration in the celiac artery, which of the following will most likely help you figure out what is going on?
A. Comparing PSVs with inspiration and exhalation
B. Determining if there are flow changes postprandially
C. Determining if the flow is different when the patient fasts
D. Comparing PSVs with the patient in a slightly different position
E. Helping the patient relax and then retaking the velocity measurements
A
A 69-year-old patient presents with a one-year history of uncontrollable hypertension. Duplex findings include elevated, low resistance PSVs (130 - 150 cm/sec) throughout the right renal artery without post stenotic turbulence, as well as a cystic right kidney, absence of flow in the left renal artery, and a small left kidney with PSVs of 8 cm/sec. What is the most likely significance of the velocities in the right renal artery?
A. Accessory renal artery
B. Within normal limits
C. Hydronephrosis
D. Contralateral nephrosclerosis
B
A 65-year-old patient presents to the vascular lab complaining that for the past several months she has experienced crampy abdominal pain after eating. During this time, she has lost 15 lbs. A pre / postprandial duplex study yields the following findings. Which of these findings is considered to be within normal limits?
A. The EDVs of the SMA are approximately 2 cm/sec pre and postprandially
B. The celiac artery's PSVs are > 280 cm/sec with spectral broadening
C. The SMA and celiac artery branch off a common trunk
D. The IMA's PSVs are approximately 280 cm/sec followed by turbulence
C
An angiogram reveals significant aortoiliac occlusive disease in a 55-year-old male. Vascular laboratory findings show resting ankle/brachial indices of 0.4 on the right and 0.3 on the left. All of the following situations could be possible EXCEPT:
A. The patient complains of impotence
B. The patient has 1/2 block claudication
C. The patient has palpable pedal pulses
D. The patient experiences ischemic rest pain.
C