Abnormal Psych Exam 4
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Who is Peter Lang?
a graduate research professor who is known for his theory and research in the area of emotion and is the creator of the “Three-Systems View”
What is the “Three-Systems View”?
a framework for assessing emotions, particularly fear and anxiety, by dividing them into three distinct, yet loosely coupled, response systems:
Self-Report measures: asking questions in an interview
Benefits: subjective / Limitations: people lie lol (embarrassed), repressive coping → difficult to tap into emotions
Behavioral measures: valid observational state, see how people act while in sessions, lack eye contact / stimming
Benefits: see how often they occur, sometimes hard to hide / Limitations: some will show in other ways such as physiologically → MASKING
Physiological measures: heart rate, skin response, muscle tension
Benefits: can't entirely ide (although we have more control than we think) / Limitations: individual response stereotypy Everyone has different ways to respond to anxiety, not everyone has high heart rate
Who are Lacey and Lacey?
They were researchers in psychophysiology who studied how physiological measures relate to psychological function. They defined "Individual Response Stereotypy" (IRS) as the tendency for a person to react to various stressors with a consistent, unique pattern of physiological arousal (e.g., sweating, racing heart, or muscle tension).
Everyone has different physiological channels primarily responds to anxiety → not everyone has high heart rate… need multiple samples to measure.
What is generalized anxiety?
“Free floating anxiety” (Freud)
6 months
Excessive worry all the time, need to worry / invent a problem to be worried about
Sometimes get treatment through physiological symptoms
Treatment recommendations:
Anti-anxiety/depressant meds
Relaxation training: have to be careful, can INDUCE anxiety
Cognitive-Behavioral Interventions: help them realize how little their worries are real / occur
what is a specific phobia?
Extreme fear to certain stimulus (spiders, clowns)
6 months
Situationally bound panic attack
Out of proportion, most people don't know why they have it in the first place
Treatments:
Relaxation training
Systematic desensitization (relax patient, gradually do steps to exposure, VIVO = REAL LIFE PHYSICAL)
Participant modeling (be with phobia together)
Learning coping statements
what is social anxiety disorder?
Marked fear or anxiety about one or more social situations in which the individual is exposed to possible scrutiny by others.
The person fears acting in a way or show anxiety symptoms that will be negatively evaluated (e.g., humiliating, embarrassing, lead to rejection, or offend others).
The fear/anxiety is out of proportion to actual danger and this pattern typically lasts for at least 6 months or longer
DIFFERENTIATE FROM AVOIDANT PERSONALITY DISORDER: fear of all social situations
Treatments: (same as specific phobia)
Relaxation training, Systematic desensitization (relax patient, gradually do steps to exposure, VIVO = REAL LIFE PHYSICAL), Participant modeling (be with phobia together) Learning coping statements
What are obsessions regarding OCD?
Persistent ideas, thoughts, impulses, or images that are experienced, at some time during the disturbance as intrusive, senseless, and unwanted, and in most individuals, causes marked anxiety or distress.
The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some thought or action (i.e., performing a compulsion
what are compulsions regarding OCD?
Repetitive behaviors (e.g., handwashing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to the obsession or according to rigid rules.
The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation. However, the behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent (or they are clearly excessive).
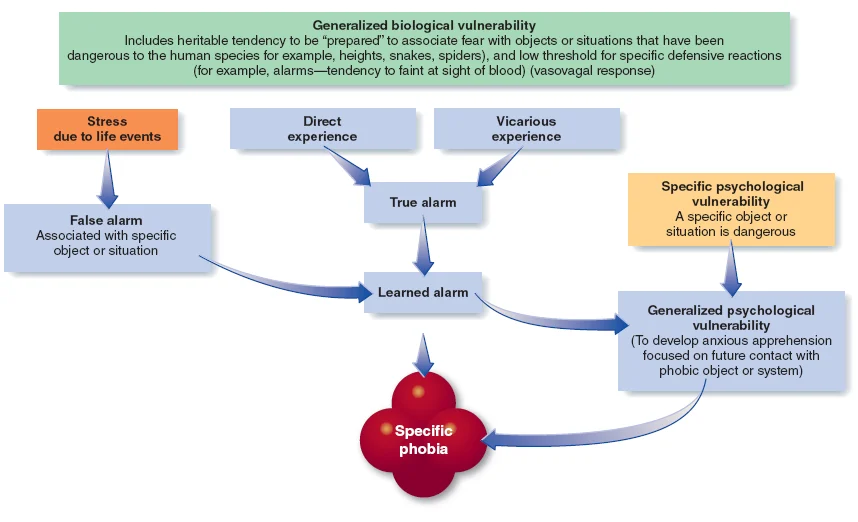
what is this etiology for?
specific phobias
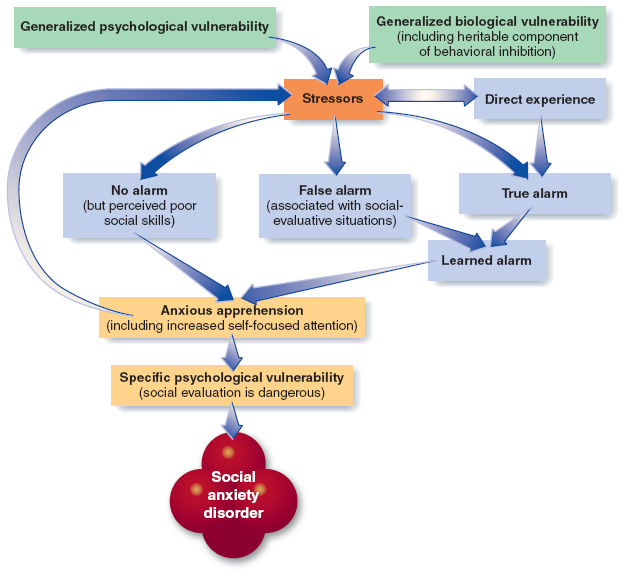
What is this etiology for?
social anxiety
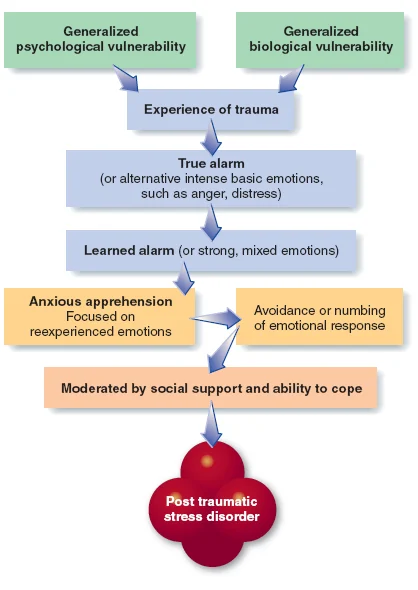
what is this etiology for?
PTSD
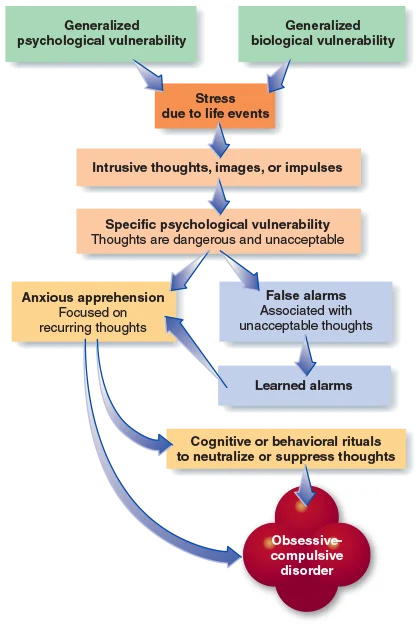
what is the etiology for this?
OCD
what is the general etiology of anxiety disorders? what are treatment recommendations?
it is the integrative (biopsychosocial) approach, and was greatly influenced by Barlow’s work
treatment recommendations include common used medications and psychotherapy approaches like response prevention techniques or Barlow’s Panic Control Therapy.
what is a panic disorder?
An anxiety disorder marked by unpredictable minutes-long episodes of intense fear/discomforts in which a person experiences four or more of the 13 symptoms:
Palpitations, pounding heart, or accelerated heart rate, Chest pain or discomfort, Nausea or abdominal distress, Sensations of shortness of breath or smothering, Feeling of choking, Sweating, Trembling or shaking, Feeling dizzy, unsteady, lightheaded, or faint, Paresthesia (numbness or tingling sensations), Chills or hot flushes, Derealization (feelings of unreality) or depersonalization (feeling detached from oneself), Fear of losing control or going crazy, Fear of dying
what are the types of panic attacks?
Situationally-Bound – characterize Specific Phobia and Social Phobia
Unexpected – characterize Panic Disorder
Situationally-Predisposed – can also characterize Panic Disorder, as when a person is more likely to experience a Panic Attack in certain situations but can (and do) experience them in other situations.
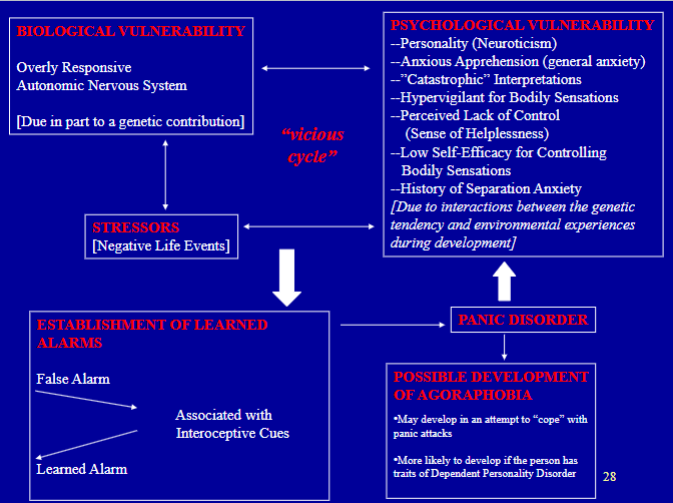
What is agoraphobia? Know that Agoraphobia seems to develop in some individuals as a way of coping with Panic Disorder, and please understand that Agoraphobia is more likely to develop in this secondary way if the person has dependent personality traits.
Connection between panic disorder, fear of the world, embarrassed of having panic attack and get help after
Beings great fear of going alone → need companion
Get groceries at night / all duties in one day → won't have to do for another month
NON-ADAPTIVE coping
Treatments:
Anti-anxiety / depression meds
Panic control therapy: exposure to bodily sensation with relaxation training → desensitize to sensation as panic
What is Relaxation-Enhanced Anxiety (also called: Relaxation-Induced Anxiety)? In discussing the percentage of people who experience it, the lower percentage on the range likely represents the general population, whereas the higher percentage in the range likely represents the population of patients with severe anxiety in an anxiety disorder clinic. When it is experiences, what are some of the physiological mechanisms involved? Why is it important for clinicians to be aware of the issue of Relaxation-Enhanced Anxiety?
Relaxation-induced anxiety is defined as an increase in physiological, behavioral, and/or cognitive components of anxiety during relaxation training.
RIA may be fairly common among individuals who suffer from very severe chronic anxiety (15%-40%)
Potential mechanisms include fear of loss of control, aversion to self-confrontation, fear of anxiety, and aversion to tension-release experiences (Some of these sensations may be due to the shift from sympathetic nervous system dominance to parasympathetic nervous system dominance/ Also, the “rebound effect” between sympathetic and parasympathetic nervous system dominance may be involved)
what is the low to high severity of the continuum of disorders?
V-Codes
Adjustment Disorder
Acute Stress Disorder (ASD)
Posttraumatic Stress Disorder (PTSD)
Complex PTSD
Dissociative Disorders
What is cognitive behavioral intervention?
help patient realize how little their worries are real / occur
what is systematic desensitization?
relax patient, gradually do steps to exposure
VIVO = REAL LIFE PHYSICAL
what are the two ways agoraphobia is formed?
Typically develop from biological and psychological vulnerabilities
Biological: over responsive autonomic nervous system
Psychological: dependent personality traits, perceive lack of control, low self-efficacy for controlling body sensations, history of separation anxiety (needing partner)
Can be someone with panic disorder getting worse and developing agoraphobia
what are v-codes?
NOT mental disorders - just someone who needs to talk about issues such as divorce, extreme poverty
they are stressors, conditions, or problems that may be a focus of clinical attention or may affect the diagnosis, course, prognosis, or treatment of a mental disorder (may be diagnosed in addition to an actual mental disorder)
Some insurance companies do not pay for v-codes / Some exaggerate v-code to get mental disorder to get insurance = UNETHICAL Doesn’t belong on medical record if not actually true
what are adjustment disorders?
Least severe mental disorder
V-code → adjustment disorder (adjusting to new issues) 3 months of onset of stressor (ex. Divorce)
Distress that is out of proportion to typical life (social / occupational)
Stressor interfere life → psychotherapy → if resolved in 6 months → done → if not go back to therapy
what are acute stress disorders?
MILD PTSD
Trauma was not as horrible as PTSD (car crash, mugging)
Last only one month
If persist longer than 1 month + PTSD criteria are met… diagnosis can change
what are the 6 criteria of PTSD?
Exposure to Trauma: Non-normal human experience and a sense of horror to self / others
Intrusive symptoms after trauma
Only need 1 / 5 (typically have more): No control (happens with reminders), dissociative flashback (in moment all over again)
Avoidance to stimuli
When encounter stimuli → completely avoid
Anniversary effect: season / time come back, increase of symptoms
Negative alterations in mood
Need 2 / 7: Belief nervous system ruined, blame self, numb / shell shock, restrict social / spiritual life, maybe cant help because repression
Alterations in arousal and reactivity: issue concentrating (keep self busy to not think)
Duration of disturbance = more than 1 month
what are specifications associated with PTSD?
Depersonalization: feeling detached from one’s mental / body
Derealization: experience unreality of surroundings
***IMPORTANT TO KNOW THAT SYMPTOMS TAKE TIME TO DEVELOP → not exactly right after trauma
who is judith herman?
Researcher in trauma and recovery
what is complex PTSD?
NOT ever in DSM
Traumatic event that happened multiple times over time (ex: physical/emotional/domestic/sexual abuse)
what is dissociative disorder?
Disrupt every area of psychological functioning (not normal in consciousness, memory, identification, emotion, perception, body rep, motor control, and behavior)
Was multiple personality disorder → changed cause having multiple people inside of you didn’t make as much sense
Symptoms that are NOT associated with PTSD
Amnesia
Dissociative flashbacks
Disruptive intrusions (unrelated to trauma) in identity
Full-blown change among identity
what are the treatment options for PTSD?
Anti-anxiety / depressant meds
Prolonged / gradual exposure therapy
More gradual from systematic desensitization (only focuses on one stimulus vs. PTSD when there’s lots)
Cognitive therapy
Emotional journal writing (Pennebaker)
Relaxation training (with warning)
Family therapy → social support . advocate for patient
Community-based treatment → ACT go and find homeless
What does it mean to say that the major mood disorders can be categorized into: episodic mood disorders VS. less severe and chronic mood disorders?
Easier to compare and contrast between the different disorders
Episodic (more severe)
Major Depressive
Bipolar Disorders I and II
Chronic (less severe)
Dysthymic Disorder
Cyclothymic Disorder
what are mood episodes?
something occur within few week period → depend on if treated
what is a primary mood episode?
comprehensive psychosocial history: Manic, hypomanic, or mixed episodes
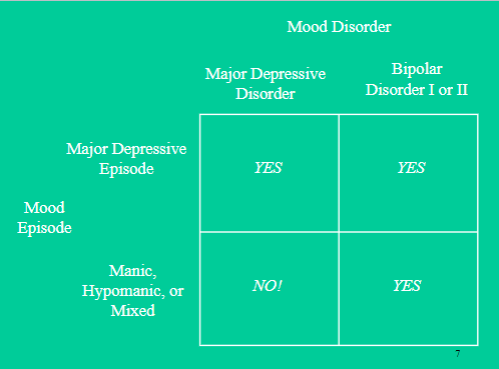
What does it mean to say that the severe and episodic mood disorders are defined by the type(s) of mood episodes experienced by the patient?
Yes? → Bipolar Disorder I or II
No? → Major depressive
Please be familiar with the symptoms of the Major Depressive Episode?
Roughly speaking, symptoms of these two mood episodes are opposite of one another - specific symptoms of the episodes (9 Factors)
Mood
Interest in activities
Energy
Sleep
POV self
Psychomotor behavior
Concentration
Weight and appetite
Suicide
Mood: depressed (nothing)
Interest in activities: no pleasure
Energy: fatigue, no energy
Sleep: insomnia (no sleep), hypersomnia (oversleep)
POV self: feelings of worthlessness / excessive guilt → take responsibility for things not at their fault
Psychomotor behavior:
Agitation: energy but nervy
Retardation: extreme lack energy, immobile
Concentration: indecisiveness (connects to insomnia)
Weight and appetite: significant weight loss / change in appetite, go with hypersomnia
Suicide: recurring thoughts of death, plan or no plan, have attempt → doesn’t have to be present
Please be familiar with the symptoms of the Major Manic Episode?
Roughly speaking, symptoms of these two mood episodes are opposite of one another - specific symptoms of the episodes (9 Factors)
Mood
Interest in activities
Energy
Sleep
POV self
Psychomotor behavior
Concentration
Weight and appetite
Suicide
Mood: elevated, expansive, irritable, (negative cloud-9, no respect for boundaries)
Interest in activities: excessive pleasure seeking → typically interest everyday life but extreme
Energy: increase goal-oriented, over determined, unrealistic goals, claim the impossible
Sleep: decreased need for sleep, hypomania (feel good w/ 4 hrs), diagnosable, w/ antidepressant (confused when it can only be given to patients with major depressive disorder???)
POV self: inflated self-esteem, exaggerate capabilities, might believe narcissistic personality however with depression only happen during mania
Psychomotor behavior: talkative, pressure to keep convo, energy bursting, “pressured speech”
Concentration: racing thoughts, cannot stay on one idea long enough to comprehend
Weight and appetite: no equivalent, depends on person, can overeat excessively during mania
Suicide: no equivalent, in mixed ep, can be dangerous
Compare Major Depressive Episode and the Manic Episode for a patient… How do they meet number of criteria from a list for but at the same time, certain criteria must be met?
Major Depressive
5/9 during same 2 week period
Presence of depressed mood, lose interest / pleasure in activities
Manic
3/7 symptoms, 4 if mood is only irritable???
Abnormality and persistently elevated, expansive, or irritable mood → last 1 week (any duration if hospitalization is necessary)
Please know which mood episodes define the following disorders: Major Depressive Disorder
Acute
Severe
Accompanied by psychotic features and psychomotor retardation
Please know which mood episodes define the following disorders: Bipolar I Disorder
Classic: have both depressive and manic
Lack stability, could have both extremes
Rapid-cycling: predicts poor long-term prognosis, hard, fast, switch of emotions, high rate for suicide
Please know which mood episodes define the following disorders: Bipolar II Disorder
ONLY hypomanic ep. (“up-times”) → hard to discover '
More likely to get miss diagnosed with major depressive
In what major way can Major Depressive Disorder appear similar to Bipolar I Disorder or Bipolar II Disorder?
Both have major depressive episodes but only bipolar has manic, hypomanic and mixed episodes
How is Major Depressive Disorder different from Bipolar I Disorder and Bipolar II Disorder? Why is it so important to make a correct “differential diagnosis”? That is, what type of problem can occur if Major Depressive Disorder is misdiagnosed as a Bipolar Disorder? Which type of Bipolar Disorder (Bipolar I Disorder or Bipolar II Disorder) is most likely misdiagnosed as Major Depression? And why? What must the clinician be careful to do in order to prevent such a misdiagnosis?
Have to understand the patient's background!!
No mania → Major Depressive
Antidepressant, Zoloft (if given wrong diagnosis can cause mania → antidepressant challenge)
Mania → Bipolar
Lithium (mood stabilizer), anti-seize meds can also work (not as extreme)
Bipolar II is more likely to get misdiagnosed since there are hypomanic ep. → seen as a ride of high
If not diagnosed correctly, and patient with bipolar gets antidepressant → can give mania (antidepressant challenge - if give mania on antidepressant and react, clear bipolar)
Don't give lithium to a patient with major depressive because it has many side effects and have to get blood drawn to check toxicity level
Bipolar II → only have hypomanic ep, hard to discover without a full history comprehension
Hypomanic to patient is seen as positive since they’re in their “up times” but it is hard to keep up with their mood changes
Careful in their psychosocial history!!!!!
What are the major neurotransmitters involved in the different mood disorders, and what are the different types of medications typically used for the different mood disorders? Similar to the note directly above, why is it important to get the diagnosis and the medication prescription correct? (As you know, a psychologist does not prescribe medications but often the diagnosis sets the stage for a psychiatrist to prescribe the medication).
Serotonin and Norepinephrine
Major Depressive: underactive, deficit
Antidepressant → Zoloft
Manic Episode: overactive, lack stability
Lithium, mood stabilizer → MANY side effects and have to check toxic levels
Could also possibly take anti-seizure meds
If give Antidepressant, Zoloft to patient with Bipolar (if given wrong diagnosis can cause mania → antidepressant challenge