X-ray interactions / filtration / beam restriction / grids
1/232
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
233 Terms
attenuation
the reduction in the number of x-ray photons in the beam (getting soaked up in the body)
Attenuation is a result of
X-ray photons interacting with matter, therefore giving up their energy to the matter with which they interact
Exponential attenuation
50% for every 4-5cm (1-2in) of tissue thickness
(lose 50% of photons to attenuation)
to compensate, radiographic technique must be roughly doubled for every 4cm (2'') increase in part thickness
compensating for attenuation
to compensate, radiographic technique must be roughly doubled for every 4cm (2'') increase in part thickness
for every 4cm (2'') increase in part thickness
technique doubled
x-rays can be
transmitted without interaction
or
interact with
-entire atom (low energy)
-orbital electron (moderate energy)
-nucleus of an atom (high energy)
low energy photons interact
with whole atom (usually too low x-rays, arent useful enough for us)
moderate energy photons interact
with orbital electrons (mainly live here and useful for us)
high energy photons
interact with nucleus
dont deal w has as much in x-rays
atomic structure
nucleus
orbital electrons (bound vs more free, binding energy)
Higher atomic number
more energy required to remove a K-shell electron from atom
We would rather have
-photons fully pass through unscathed
or
-interact with tissue fully (fully attenuate)
X-ray interactions with matter
Coherent scatter/classic (low)
Photoelectric absorption (PE)
Compton Scattering
Pair production (high energy)
Photodisintegration (high energy)
low, moderate, moderate, high, high
Coherent scattering involves
low energy photons (below 10 keV)
we dont want these
types of coherent scattering
1. Rayleigh Scattering (all electrons of atom)
2. Thomson Scattering (single outer shell electron)
Produce same result
coherent scattering
electrons are excited and vibrate at photon frequency (makes atom wiggle)
no electrons are ejected
no ionization takes place
atom will stabilize itself by releasing a photon equal in energy to the incident photon, but in a different direction
so low energy, it will most likely not leave the patient
overall, mainly just waves at atom
Which x-ray interaction do we prefer to happenn
photoelectric absorption
What happens in photoelectric absorption?
Incident photon energy completely absorbed by inner shell electron
Ionizes so it causes a photoelectron
overall
-incident energy photon completely absorbed by inner shell electron
-emits photoelectron
When is photoelectric absorption most likely to occur?
When x-ray photon has just slightly more energy than the binding energy of a K or L shell electron (reminds of characteristic)
In photoelectric, an ion pair is formed when
-an electron is ejected from the atom (becomes a photoelectron)
-remaining atom has a vacancy inn its inner electron shell
this will cause a characteristic cascade
photoelectron energy equation
Ei = Eb + Eke
incident photon= BE + Kinetic energy
photoelectron characteristics
-Kinetic energy (Eke)
-Mass
-Reabsorbs quickly
>>Within 1-2mm of tissue
Ionized atom
inner shell electron vacancy makes atom electrically unstable
Causing
characteristic cascade
-vacancy filled by an outer shell electron
-electron undergoes change in energy level
-emits characteristic photon
for PE interactions, incident photon energy
must be greater than or equal to binding energy (Eb) of inner shell electron
PE absorption interaction more likely to occur
if incident photon energy (Ei) and inner shell electron binding energy (Eb) are close to each other
As photon energy increases
Chance of PE interaction decreases dramatically
INVERSE CUBED RELATIONSHIP
-cannot be too much
Photon energy and chance of PE interaction has what kind of relationship?
Inverse cubed relationship (1/n3)
example
Ei= 120 keV
Eb= 36 keV
PE interaction will likely not take place
Only transmission will occur due to too big of energy differences
Higher atomic numbers (so higher binding energies)
will result in higher PE absorption interactions
Atomic number and PE absorption relation
Direct cubed relationship (n3)
Higher likelihood of PE with increased atomic number
If you double the atomic number
You increase chance of PE absorption by a factor of 8
Lower atomic numbers experience PE absorption with the
K shell
Higher atomic numbers experience PE absorption in
K, L, or M shell
Secondary radiation
Radiation that originates from irradiated material outside of x-ray tube
Comes from characteristic photons emitted from atoms of patient after PE absorption has occurred
Will most likely not reach the detector, not really high energy, overall it is most likely getting absorbed in the body
Low atomic number in tissue
Low energy secondary radiation
High atomic number in contrast agents
Higher energy secondary radiation (more total absorption)
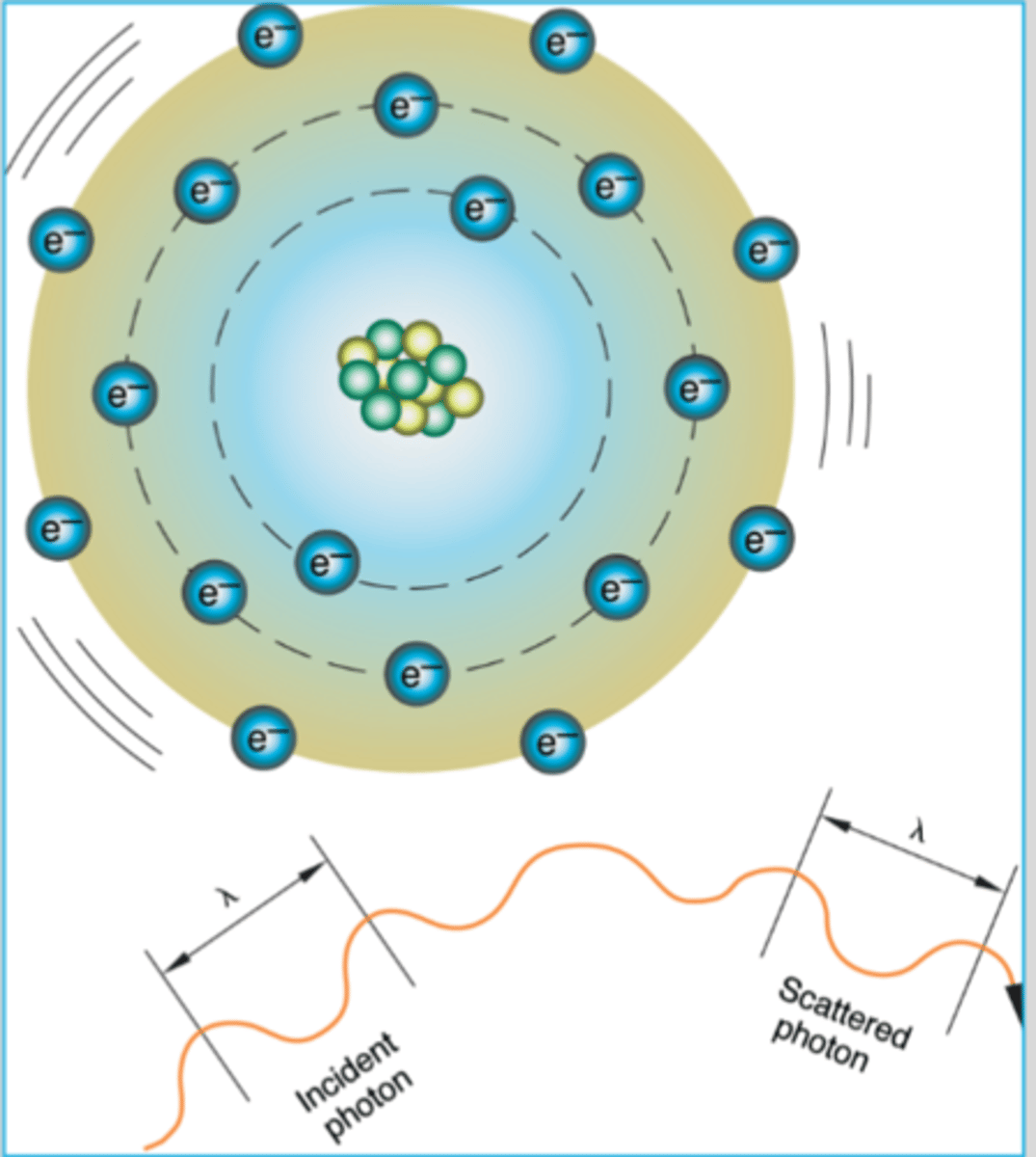
Compton scattering
incident photon (Ei) interacts with outer shell electron and ejects it
Ion pair is formed
Photon will transfer some of its kinetic energy to the recoil (compton) electron, and continues on in a different direction
Produces scatter
-which could hit detector but has less fidelity/truthfullness
97% comes from compton
Incident photon energy in compton is distributed
between recoil electron (Eke) and scattered photon (Es)
The angle and energy of scattered photon affected by
The energy transferred to recoil electron (Eke)
therefore, it affects the frequency and wavelength of the scattered photon
The recoil electron from compton will
travel until it fills a vacancy in another atom
Scattered photon will continue to interact until
aborbed photoelectrically
Compton scattering is the source of
occupational exposure and radiation fog
For a scattered photon
the amount of energy retained is dependent on the initial energy of photon and its angle of deflection from recoil electron
At lower energy (coherent)
scatter goes forward or backward (as back scatter) with less at a 90 degree angle
At moderate energy in diagnostic range (50 keV) so compton
less will be backscatter and more will be in forward direction
as energy increases outside of diagnostic radiography range
scatter is almost entirely in a forward direction
relative contribution of PE and compton on detector exposure
Pair production
high energy levels (radiation therapy)
The incident photon energy must be 1.02 MeV or higher
photon energy absorbed by the nucleus
-the nucleus will become unstable
What does the nucleus release as a result of pair production
a positron and negatron to stabilize itself
the positron will be attracted to some electron and annihilate
Negatron and positron both have
equal masses but will opposite charges
Negatron
acts like free electron and will combine with nearby atom
functions same way as normal electron
Positron
unstable antimatter
will combine with nearest electron and an annihilation reaction occurs
matter of particles is converted to energy
-results in two photons of .511 MeV (511 keV) traveling at 180 degrees to each other
Pair production is more significant in
radiation therapy
does not occur in diagnostic range of energies
Pair production is not a significant interaction until energies of
10 MeV are being used
Photodisintegration
Extremely high energy photon (10 MeV or greater)
Absorption of photon by nucleus
What does the excited nucleus do in photodisintegration?
Releases an alpha particle
Photodisintegration is not significant
in diagnostic imaging range
Most of the x-ray beam is
attenuated while some is transmitted
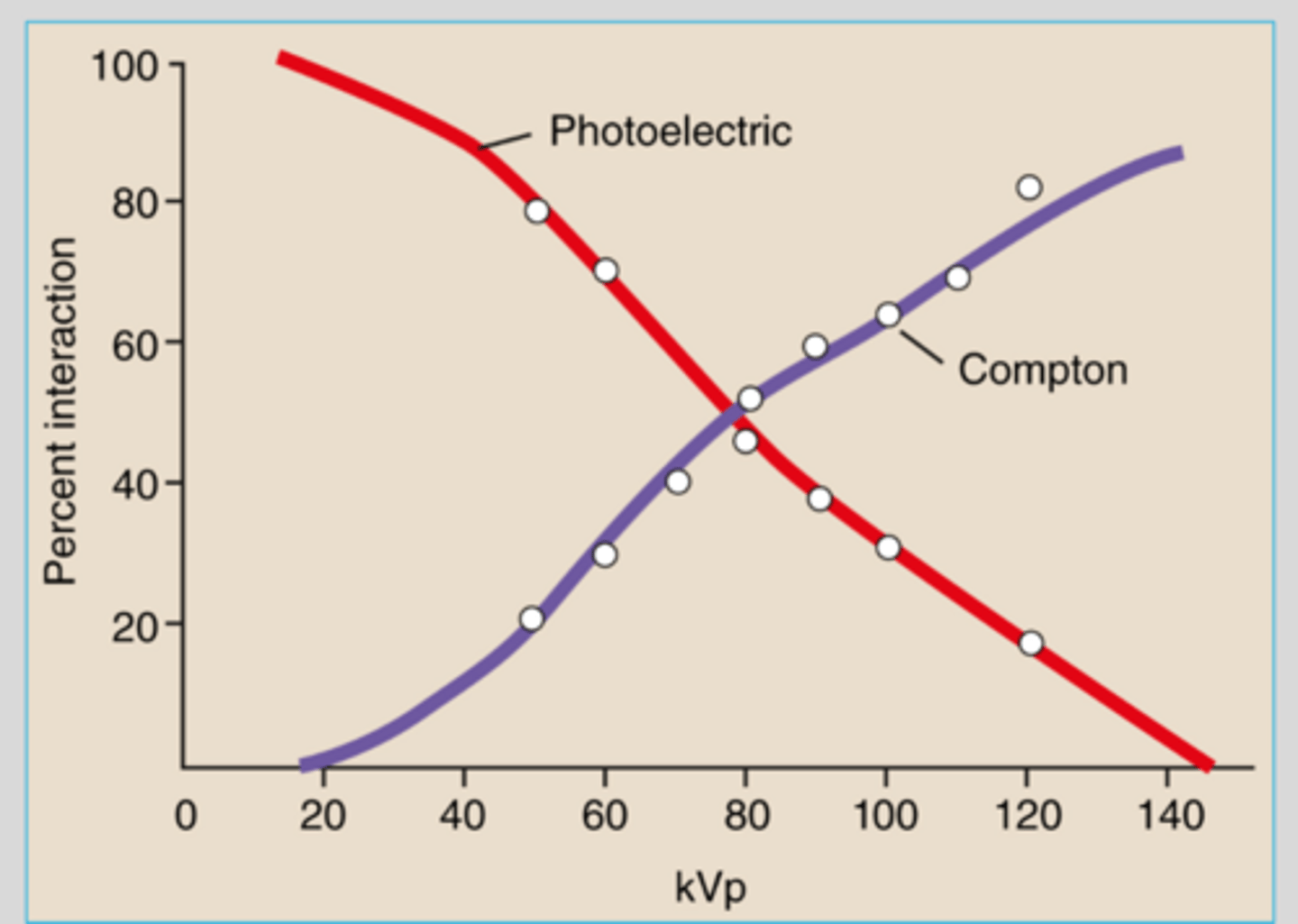
As kVp increases
the number of photons transmitted without interaction increases (reduces PE much faster than compton)
so it
-decreases probability of PE absorptionn and compton interactions
Within the attenuated beam as kVp increases
PE absorption decreases
Compton effect increassed
Increased percentage of scatter and decreased percentage of absorption
Compton scatter typically
predominates within diagnostic x-ray energy range
-reason as why we add grids when we increase in tissue density
If we increase kVp
we get more scatter
PE absorption interactions predominate in
-lower energy ranges (25-45 keV produced by 40-70 kVp techniques)
-in elements with higher atomic numbers
introduction of contrast agents result in increase of PE absorption as well
When PE absorption predominates
-resulting image will have short scale contrast (high contrast)
-low kVp
-high mAs
when compton interactions predominate
Resulting image will have long scale contrast
High kVp and low mAs
Photoelectric effect with its all or nothing absorption of x-rays is responsible for
PRODUCTION OF SUBJECT CONTRAST
Scatter radiation destroys
subject contrast in remnant beam
Photoelectric effect occurs only in
inner atomic shells when the energy of the incident x-ray photon is slightly higher than the shell binding energies
compton effect occurs
in outer shells when the energy of incident x-rays is much higher than binding energies
compton effect responsible for
97% of scattered x-rays
As the angle of deflection from scattered x-rays increases away from the central ray
we find higher amounts of scatter but at lower energies
coherent scatter can be produced by
thompson effect (single outer shell electron) or rayleigh effect (all electrons)
x-ray photon temporarily excited an entire electron or an entire atom and is then reemitted 3%
Coherent scatter
DOES NOT IONIZE so it only occurs at very low photon energies
Compton is more uniform because
it relies on electron density
probability remains relatively constant
Compton scatter contributes least
to patient dose and image formation
Increaassing patient thickness
increases the probability of attenuation
Filtration
Process of eliminating undesirable, low-energy photons from the primary beam
Provides dose reduction to patient
Filtration is also known as
hardening the beam
making it strong!!
What is considered the standard filtering material
Aluminum
How is filtration expressed
Aluminum/equivalence (Al/Eq)
Half-value layer (HVL)
amount of absorbing material that will reduce intensity of primary beam to one-half its original value
Required HVL
2.5 mm of Al
Types of filtration
Inherent
Added
Compound
Compensation/compensating
Total
Inherent filtration
filtration that is a result of the composition of the tube and housing
-glass or metal envelope x-ray tube
-insulating oil
Value of inherent filtration in general purpose tubes
0.5mm to 1.00 mm Al/Ew
Tube degradation will increase
the value of inherent filtration due to vaporization of tungsten, reducing efficiency
HVL tests recommended as part of QC program
Added filtration
Any filtration that occurs between outside of tube/housing and the patient
It is outside tube housing but before it reaches the patient
Added filtration composed of
1.0 mm Al/Eq from variable-aperture light-localizing collimator
-due to reflective silver surface of mirror in collimator
an additional 1.0 mm Al filter inserted between the tube housing or collimator (to meet required total filtration of 2.5 mm Al/Eq)
Technologies will have no control over these sources of filtration (cant change thickness of filtration)
Some systems have added filtration capabilities
Button/mechanism on collimator
Example: copper filtration
Compound filtration
composite filters using two or more materials to absorb photons of different energy levels
layered with highest atomic number material ON TOP
lowest atomic number will go on bottom
designed so that subsequent layers absorb characteristic photons produced by previous layer
example: Thoraeus filter
There has been a renewed interest in
copper filters for digital diagnostic imaging (our GE digital machine has Cu filtration capabilities)
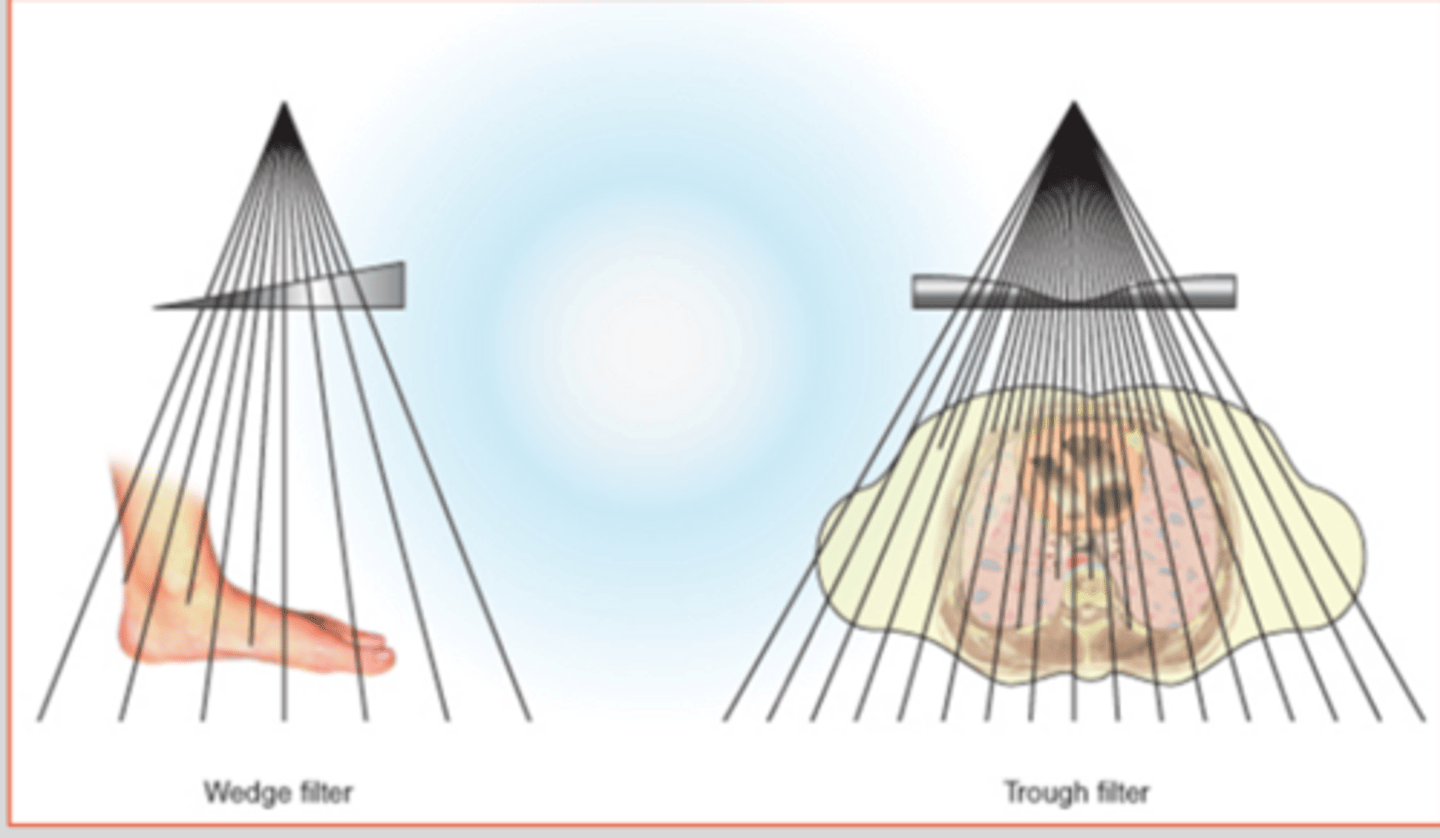
Compensating filter
Shapes of aluminum mounted onto transparent panel that slides into grooves beneath the collimator
Purpose is to compensate for unequal absorption within target tissue (not used to reduce patient dose)
Compensating filters balance
the intensity of x-ray beam to deliver more uniform exposure to the detector
Wedge (spine and foot)
Trough (chest)
ClearPbTM: clear lead, some aspect of filtration
Thoraeus Filter
Tin
Copper
Aluminum
Total filtration
the sum of inherent and added filtration
does NOT include compound or compensating filters that may be added later
National council on radiation protection and measurement (NCRP) minimum recommendations for filtering
below 50 kVp: 0.5 mm Al/Eq
50-70 kvp: 1.5 mm Al/Eq
Above 70 kVp: 2.5 mm Al/Eq!!!!
Effect of filtration on output
increased filtration causes
-increase in X-ray beam energy
-increase in X-ray penetrability
-decreases total number of photons
Exposures must be increased to compensate for increased attenuation
But there is still a patient exposure savings due to getting rid of low energy useless photons
If above 3mm Al/Eq
the reduction in patient entrance skin dose does not improve enough to offset the necessary increase in technical factors or the tube loading increase
TAKING TOO MANY PHOTONS AWAY (MOTTLE, ADJUST MAS TO COMPENSATE)
Sole purpose of protective filtration
Spare unnecessary patient exposure from primary beam
If filtration affects the remnant beam exposure to the detector
Too much filtration has been utilized