APEX Unit 3: Cardiovascular
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
Define Chronotorpy, Inotropy, Dromotropy, and Lusitropy.
Chronotropy: HR
Inotropy: Contractility
Dromotropy: Conduction velocity (how fast action potential travels per time).
Lucitropy: Rate of Myocardial Relaxation (diastole)
Describe the function of the Sodium-Potassium Pump
The sodium-potassium pump maintains the cell's resting potential. Said another way, it separates charge across the cell membrane keeping the inside the cell relatively negative and the outside of the cell relatively positive.
How it works:
- It removes the Na+ that enters the cell during depolarization
- It returns K+ that has left the cell during repolarization
- For every 3 Na+ ions it removes, it brings 2 K+ ions into the cell.
Depolarization: Na+ In
Repolarization & Resting State: K+ Out
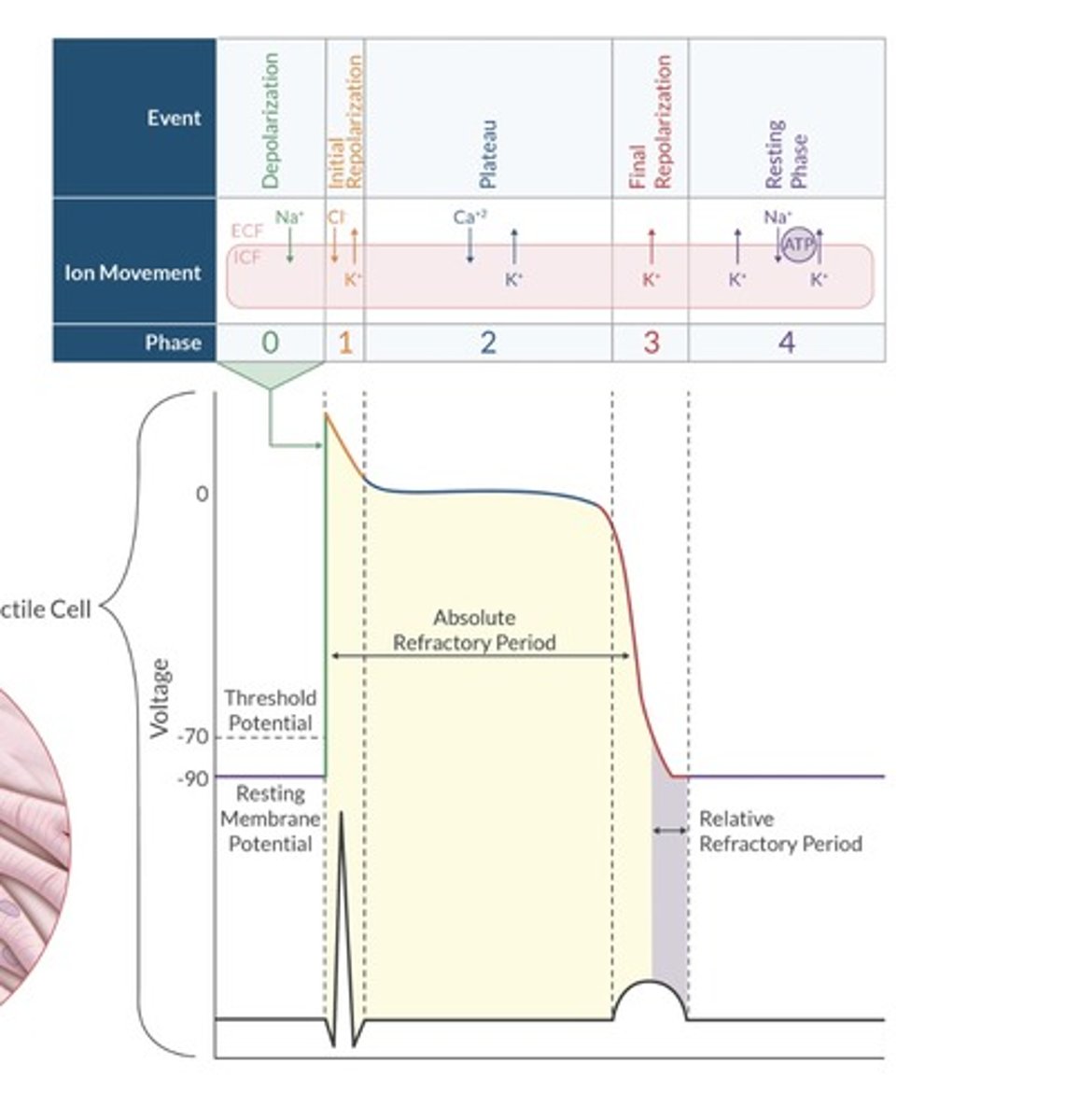
List the 5 phases of the ventricular action potential and describe the ionic movement during each phase.
Phase 0: Depolarization (Na+ in)
Phase 1: Initial Depolarization (K+ out, Cl- in)
Phase 2: Plateau (Ca+2 in)
Phase 3: Repolarization (K+ out)
Phase 4: Na+/K+ restores resting membrane potential
List the 3 phases of the SA node action potential and describe the ionic movement during each phase.
Phase 4: Spontaneous deplarization (Leaky to Na+) DETERMINES HR.
Phase 0: Depolarization (Ca+2 influx)
Phase 3: Repolarization (K+efflux)
What process determines the intrinsic heart rate, and what physiological effects alter it?
The rate of spontaneous phase 4 depolarization in the SA node determines HR.
What is the MAP formula?
MAP = SBP + (DBP x 2) / 3
What is the formula for Systemic vascular resistance (SVR)?
SVR = (MAP - CVP) / CO x 80
What is the formula for pulmonary vascular resistance (PVR)
PVR = (Mean PA pressure - PAOP) / CO x 80
Describe the Frank-Starling Relationship:
-Describes the relationship between ventricular volume (preload) and ventricular output (cardiac output)
-Increasing preload increases ventricular output, but only up to a point.
Increased stretch = increase output
Decreased stretch = decreased output.
What factors affect myocardial contractility?
Contractility (inotropy) describes the contractile strength of the heart.
Just remember that Chemicals affect Contractility - particularly Calcium.
Most examples in the table either alters the amount of Ca+2 available to bind to the myofilaments or impacts the sensitivity of the myofilaments to Ca+2.
What is afterload, how is it measured in clinical setting?
Afterload = force the ventricle must overcome to eject SV.
Measured via SVR.
What law can be used to describe ventricular afterload?
Laplace.
Wall stress = intraventricular pressure x radius / ventricular wall thickness.
Wall stress reduced by decreased intraventricular pressure, decreased radius, increased wall thickness.
List 2 conditions that set afterload proximal to the systemic circulation.
Aortic Stenosis
Coarctation of the Aorta
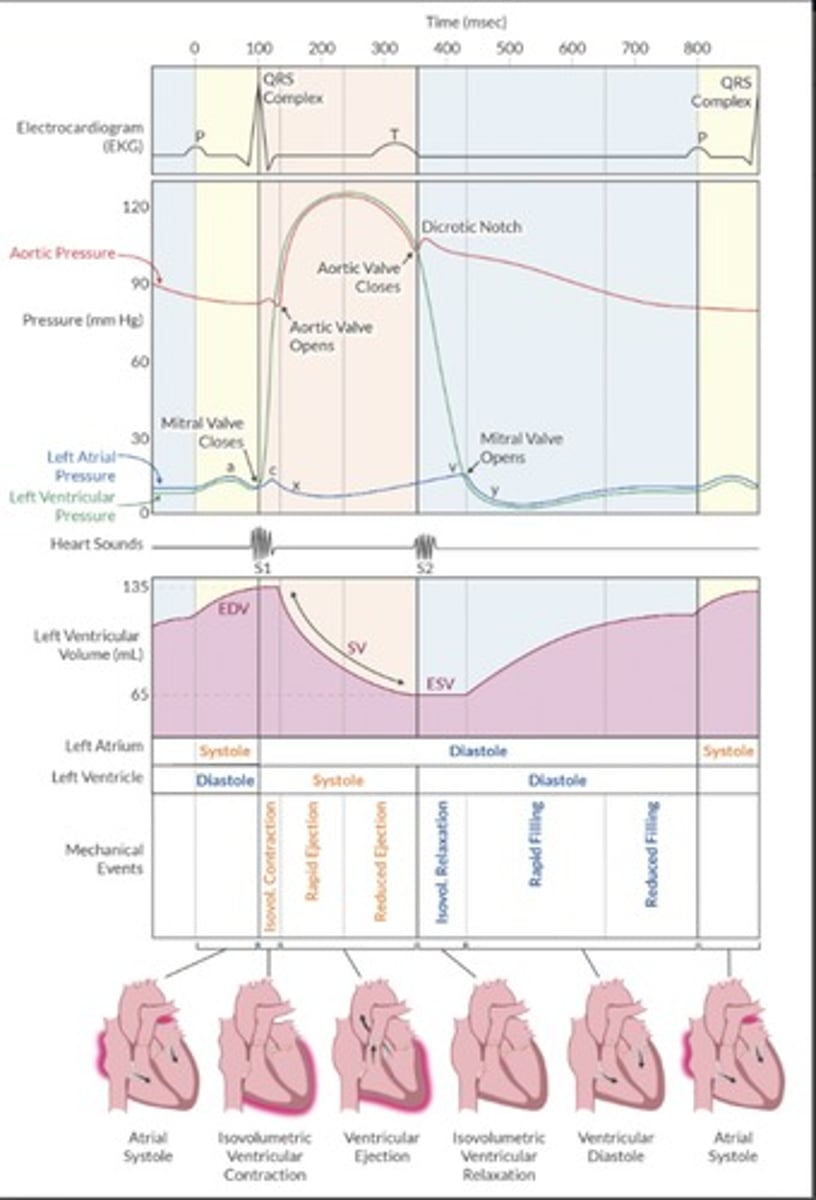
Use Wigger diagram to explain the cardiac cycle.
Know the picture. Waveforms.
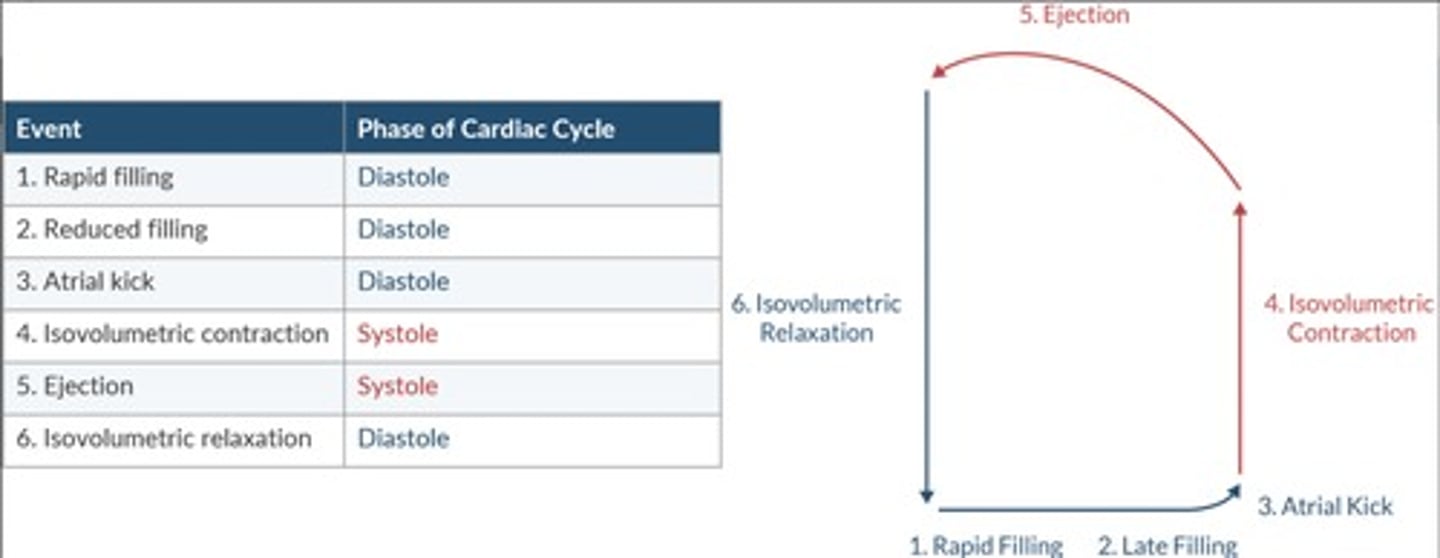
Relate the 6 stages of the cardiac cycle to the LV pressure-volume loop.
Know the picture.
How do you calculate ejection fraction?
EF % = (EDV - ESV) / EDV
Normal: > 50%
Mild: 41-49%
Moderate: 26-40%
Severe: < 25%
What is the best TEE for diagnosing myocardial ischemia?
Midpaillary muscle in SHORT AXIS
What is the equation for coronary perfusion pressure (CPP)?
CPP = DBP - LVEDP (or PAOP)
Which region of the heart is most susceptible to myocardial ischemia?
-Why?
The Left ventricle subendocardium is most susceptible.
Best perfused during diastole. As aortic pressure increases, LV tissue compresses its own blood supply and decreases its blood flow. The high compressive pressure in the LV subendocardium w/ a decreased coronary art. blood flow during stole increases coronary vascular resistance predisposing it to ischemia.
What factors affect myocardial oxygen supply and demand?
Reduce O2 delivery:
Tachycardia
Decreased aortic pressure
decreased vessel diameter
Increased end diastolic pressure
Hypoxemia
Anemia
Left shift of oxy-hgb curve (decreased P50)
Decreased capillary density
Increase O2 Demand:
Tachycardia
HTN
SNS stimulation
Increased wall tension
Increased end diastolic volume
Increased afterload
Increased contractility
Discuss Nitric Oxide pathway of vasodilation
-Nitric oxide is a smooth muscle relaxant that induces vasodilation.
1. Nitric oxide synthase catalyzes the conversation of L-arginine to nitric oxide
2. Nitric oxide diffuses from the endothelium to the smooth muscle
3. Nitric oxide activates guanylate cyclase
4. Guanylate cyclase converts guanosine triphosphate to cyclic guanosine monophosphate
5. Increased cGMP reduces intracellular calcium, leading to smooth muscle relaxation
6. Phosphodiesterase deactivates cGMP to guanosine monophosphate (turns off NO mechanism)
What are the two primary ways a heart valve can fail?
Stenosis:
-Fixed obstruction to forward flow during chamber systole.
-Chamber must generate higher than normal pressure to eject blood.
Regurgitation:
-Valve is incompetent (leaky)
-Some blood flows forward, and some backward during systole.
How does the heart compensate for pressure overload?
Volume overload?
Aortic stenosis/pressure overload/concentric hypertrophy = Sarcomeres added in parallel.
Aortic valve regurgitation (diastole)/volume overload/eccentric hypertrophy = Sarcomeres added in Series.
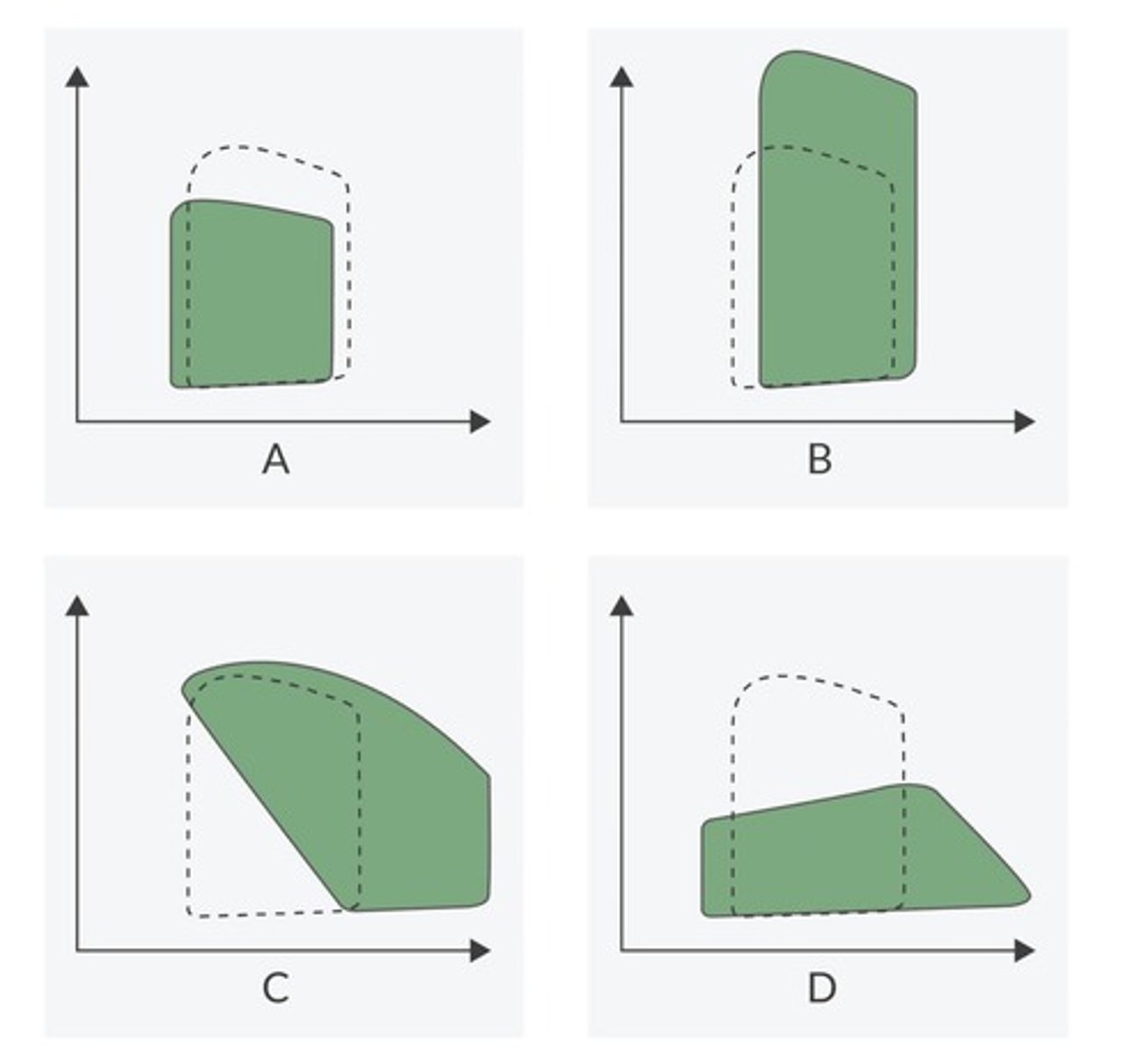
Identify Each pressure volume Loop.
A = Mitral Stenosis
B = Aortic stenosis
C = Aortic regurgitation
D = Mitral regurgitation
List the hemodynamic goals for the 4 common valvular defects.
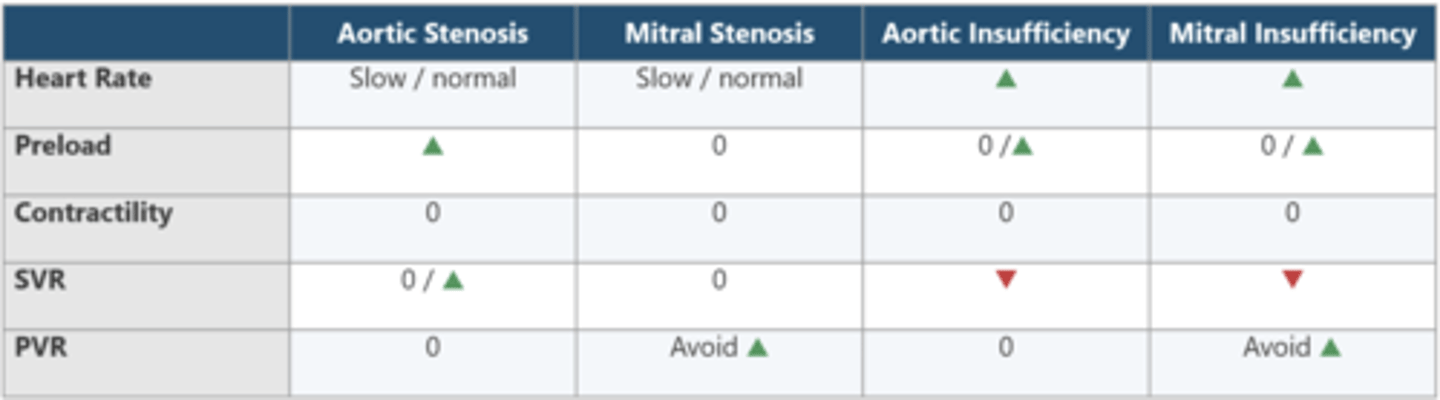
What is the most common dysrhythmia associated with MITRAL STENOSIS?
A-FIB
List 6 risk factors for perioperative cardiac morbidity and mortality for non-cardiac surgery.
High-Risk surgery
History of Ischemic heart disease (unstable angina confers greatest risk of perioperative MI)
History of CHF
History of CVA
DM
Serum creatinine > 2 mg/dL
What is the risk of perioperative MI in patient with previous MI?
General population = 0.3%
MI if > 6 months = 6%
MI if 3-6 months = 15%
MI if < 3 months = 30%
HIGHEST RISK of reinfarction is greatest within 30 days of MI
ACC/AHA recommend 4- 6 weeks before elective surgery with recent MI.
Categorize high, medium, and low risk surgical procedures according to cardiac risk.
High (Risk > 5%):
Emergency surgery (especially in elderly)
Open Aortic surgery
Peripheral vascular surgery
Long surgical procedures with significant volume shifts/blood loss.
Intermediate (Risk 1-5%):
Carotid Endarterectomy
Head and Neck surgery
Intrathoracic or intraperotoneal surgery
Ortho
Prostate
Low (Risk < 1 %):
Endo
Cataract
Superficial procedures
Breast surgery
Ambulatory surgery
How do you interpret cardiac enzymes in the patient with a suspected ischemic event?
Infarcted myocardium releases 3 key biomarkers: Creatine Kinase-MB (CKMB), Troponin I, and Troponin T.
Cardiac Tropoinins are more sensitive than CKMB for dx of MI.
How do you treat intraoperative ischemia?
Focus on making heart slower, smaller, and better perfused.
Increased O2 demand (increased HR, BP, PAOP):
-beta blocker to HR < 80 bmp
-Increase depth of anesthesia, vasodilator, Nitro
Decreased O2 supply (Low HR, BP, increased PAOP):
Anticholinergic, pacing
Vasoconstriction, reduce depth of anesthesia
Nitroglycerin, inotrope.
What factors reduce ventricular compliance?
-Age > 60 years
-Ischemia
-Pressure overload hypertrophy
-Hypertropic obstructive cardiomyopathy
-Pericardial pressure
*Higher filling pressures are required to prime the ventricle
What is the difference between HFrEF (systolic) and HFpEF (diastolic) HF?
Systolic - HF with reduced EF = ventricle doesn't empty well.
Diastolic - HF with preserved EF = Ventricle doesn't fill properly
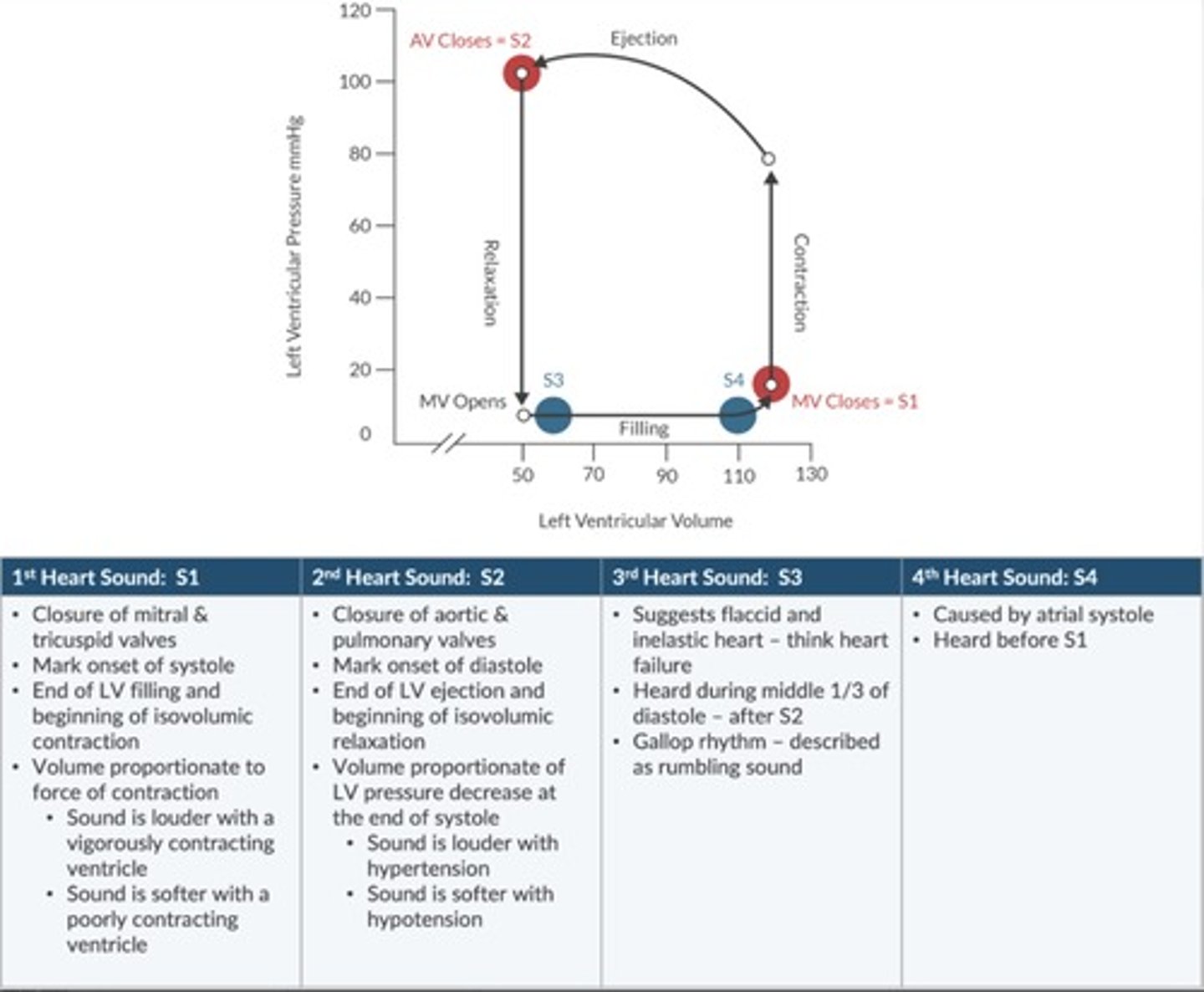
Where do the heart sounds match up on the left ventricular pressure loop?
MV closes = S1
AV closes = S2
What is the modified NYAFC of HF? (Class 1-4)
Class 1: Asymptomatic
Class 2: Symptomatic with Moderate activity
Class 3: Symptomatic with Mild activity
Class 4: Symptomatic at rest
LIst 6 complications of HTN.
- LV hypertrophy
- IHD
- CHF
- Arterial aneurysm (aorta, cerebral)
- Stroke
- ESRD
How does HTN contribute to CHF?
HTN -> increase myocardial wall tension ->
- LVH -> CHF -> infarction dysrhythmias
- increase MVO2 - Coronary insufficiency -> infarction dysrhythmias
How does HTN affect cerebral autoregulation?
Cerebral auto regulation describes the range of BP where CPP remains constant.
-Chronic HTN shifts the curve to the right. This adaptation helps the patient's brain tolerate a higher range of blood pressures, however this comes at the expense of not being able to tolerate a lower blood pressure.
What is the difference between primary HTN and Secondary HTN?
Primary (ESSENTIAL): most common and has NO identifiable cause (95% of all HTN cases).
Secondary HTN: Caused by some pathology (5% of cases).
List 7 causes of Secondary HTN
- coarctation of aorta
- renovascular disease
- hyperadrenocorticism (Cushing's)
- hyperaldosteronism (Conn's)
- pheochromocytoma
- pregnancy-induced HTN
What are the 2 classes of calcium channel blockers? List examples
Dihydropyridines: end in "-pine" Nifedipine, Nicardipine, Nimodipine, Amlodipine, Clevidipine. Target vascular smooth muscle causing vasodilation and decreased SVR.
NON-Dihydropyridines: Decrease chronotropy (HR), Inotropy (contractility), Dromotropy (Conduction velocity) and Coronary vascular resistance.
Verapamil - Phenylalkylamine
Diltiazem - benzothiazepine
Describe the pathophysiology of constrictive pericarditis.
Caused by fibrosis or any condition where pericardium becomes thicker.
During diastole ventricles can't fully relax reducing compliance and limits filling. ventricular pressure increases, creating a back pressure to peripheral circulation. Ventricles adapt by increasing mass, but impairs systolic function.
Describe anesthetic management of constrictive pericarditis.
Avoid Bradycardia
Preserve HR and contractility (Ketamine, pancuronium, VA with caution, opioids, Benzo's, and etomidate OK).
Maintain afterload.
Describe the Pathophysiology of Cardiac Tamponade.
Cardiac tamponade occurs when the buildup of pericardial fluid compresses the heart.
Limits the heart's ability to fully expand. If not treated, cardiac filling reduces enough to stop blood circulation.
TEE is best diagnostic tool. Treatement is pericardiocentesis or pericardiostomy.
What is Kussmaul's sign?
Indicates impaired RV filling d/t poorly compliant RV.
Impaired RV filling affecting = blood backup = JVD and increased CVP.
Most pronounced during inspiration.
List 2 conditions associated with Kussmaul's sign.
CONSTRICTIVE PERICARDITIS
PERICARDIAL TAMPONADE
What is pulsus paradoxus?
An exaggerated decrease in SBP during inspiration (more than 10 mmHg) → this finding suggests impaired diastolic filing
List 2 common conditions associated with Pulsus Paradous.
CONSTRICTIVE PERICARDITIS
PERICARDIAL TAMPONADE
What is Beck's Triad?
What conditions are associated with it?
Occurs in patient with acute Cardiac Tamponade.
s/s: Hypotension (Decreased SV)
JVD (impaired venous return to right heart)
Muffled Heart tones (fluid accumulation in pericardial space)
What are best anesthetic techniques for the patient with acute pericardial tamponde undergoing pericardiocentesis?
Local anesthesia is preferred technique.
Avoid:
VA
Propofol
Thiopental
High Dose Opioids
Neuraxial
Use:
Ketamine Drug of choice
Nitrous Oxide
Benzo's
Opioids
List 7 patient factors that warrant antibiotic prophylaxis against infective endocarditis.
-Previous infective endocarditis
-Prosthetic heart valve
-Unreported cyanotic congenital heart disease
-Repaired congenital heart defect if repair is < 6 mo. old
-Repaired congenital heart disease w/ residual effects
-Heart transplant with valvuloplasty
List 3 surgical procedures that warrant antibiotic prophylaxis against infective endocarditis.
-Dental procedures involving gingival manipulation
-Respiratory procedures that perforate mucosal lining.
-Biopsy of infective lesions
What are 3 key determinants of flow though the LVOT
Systolic LV volume
Force of contraction
Transmural pressure gradient
What factors reduce cardiac output in the patient with obstructive hypertrophic cardiomyopathy?
Things that distend the LVOT are good for cardiac output, while things that narrow LVOT are bad.
How long should elective surgery be delayed in the patient after percutaneous coronary intervention? Bare metal stent, CABG, Drug eluding stent?
Angioplasty w/out stent: 2 - 4 weeks
Bare metal stent: 30 days (3 months preferred)
Drug Eluding Stent: 12 Months
CABG: 6 weeks (3 months preferred)
What is the difference between alpha-stat and pH-stat blood gas measurements during CPB?
ALl about patient Temperature.
Alpha stat: Does NOT correct for patient temp.
pH-stat: corrects for patient temp.
Why is a left ventricular vent used during CABG?
LV vent removes blood from the LV. this blood comes from the Thebesian veins and bronchial circulation (anatomic shunt).
How does the intra-aortic balloon pump function thoughtout the cardiac cycle?
How does it help the patient?
Improves myocardial O2 supply while reducing O2 demand.
Diastole: Pump INFLATES augmenting coronary perfusion
Inflation correlates with dicrotic notch on aortic pressure waveform.
Systole: Pump DEFLATION reduces afterload and improves CO.
Deflation correlates with R wave on EKG.
4 contraindications to Baloon-pump.
Severe aortic insufficiency
Depending aortic disease
Sever PVD
Sepsis
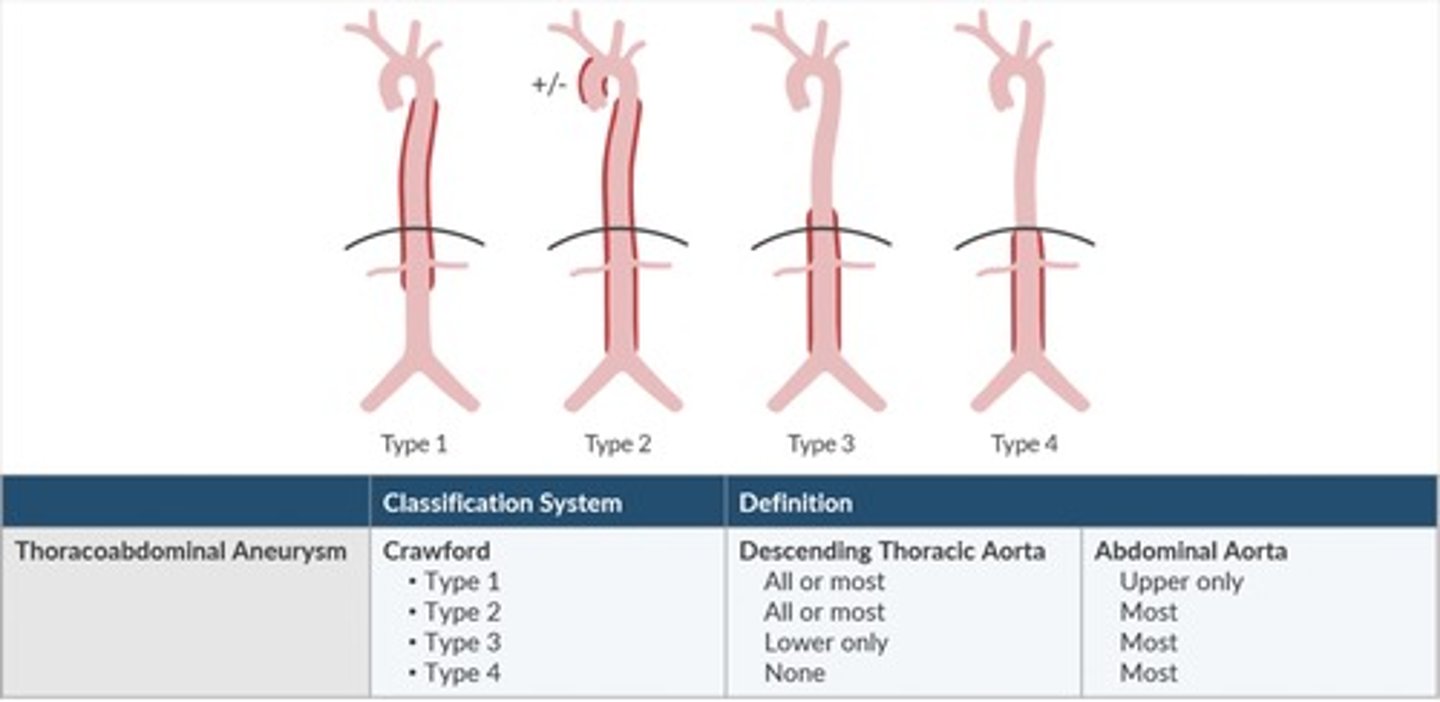
Describe the Crawford classification system of aortic aneurysms.
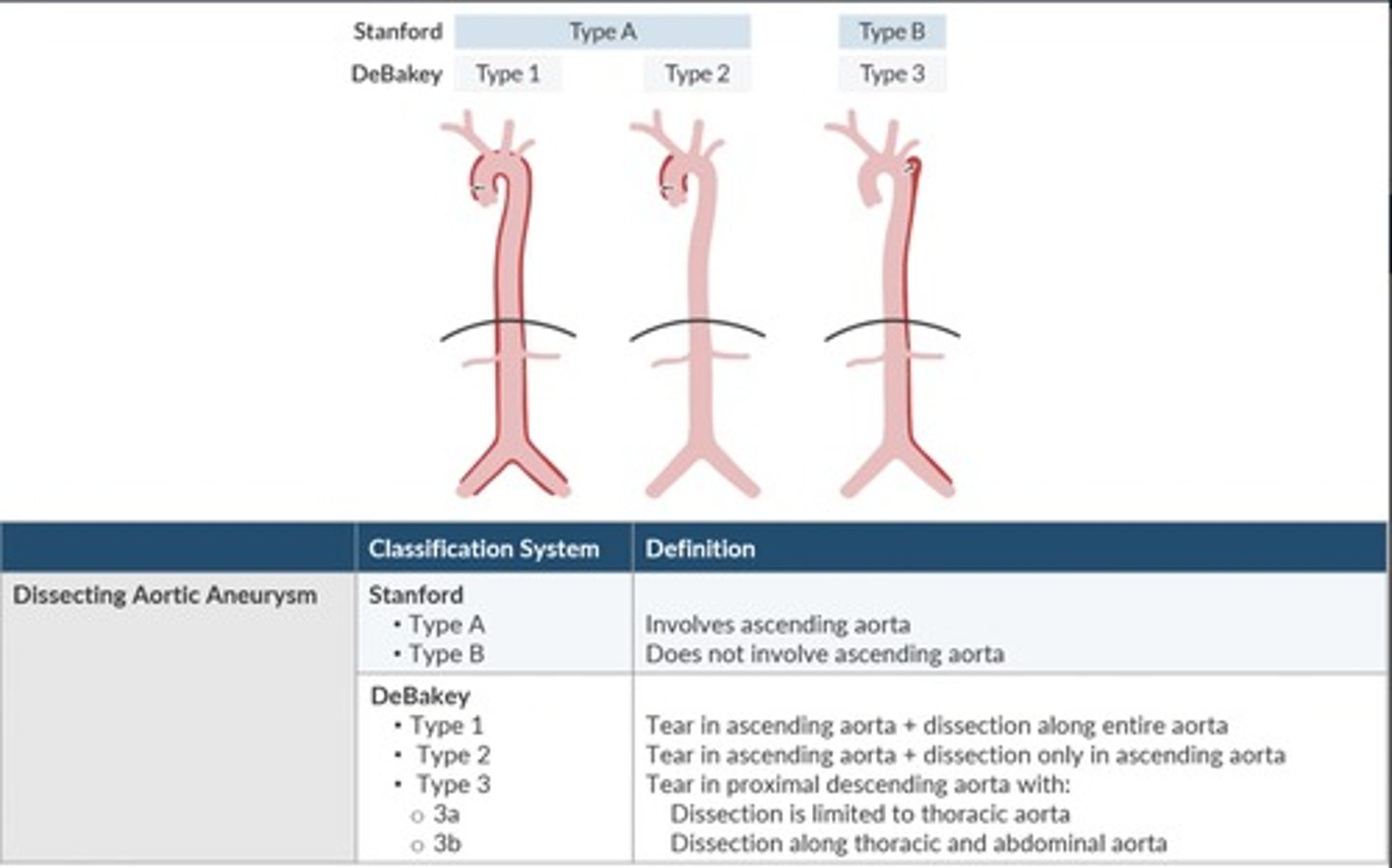
Describe the DeBakey and Stanford classification systems of aortic dissection.
Which law describes the relationship between aortic diameter and risk of aortic rupture in the patient with an abdominal aortic aneurysm?
-When is surgical correction for an abdominal aortic aneurysm recommended?
Laplace.
Diameter of the AAA correlates with risk of rupture
Wall tension = transmural pressure x vessel radius
Increased diameter -> increased transmural pressure -> Increased wall tension.
Mortality increases significantly when AAA = 5.5cm.
Surgical correction is recommended when the aneurysm EXCEEDS 5.5cm or if it grows more than 0.6-0.8cm/yr.
How does the aortic cross clamp contribute to the risk of anterior spinal artery syndrome?
Aortic cross clamp placed ABOVE artery of ADAMKIEWICZ may cause ischemia to lower portion of anterior spinal cord.
-Can result in Beck's Syndrome.
How does anterior spinal artery syndrome present?
-Flaccid paralysis of the lower extremities
-Bowel and bladder dysfunction
-Loss of temperature and pain sensation
-Preserved touch and proprioception
What is amaurosis fugax?
-Blindness in one eye
-Sign of impending stroke. Emboli travel from the internal carotid artery to the ophthalmic artery, which impairs perfusion of the optic nerve and causes retinal dysfunction.
Patient undergoing carotid endarterectomy with EEG monitoring. What does this monitor tell you, and what conditions can lead to false conclusions?
Monitors cortical electrical funtion
Risk of cerebral hypo-perfusion with loss of amplitude, decreased Beta wave, and/or appearance of slow wave activity.
Causes of false-negatives:
-Extreme hypercarbia
-Hypoxia
-Cerebral ischemia
-Anesthetic overdose
-Opioids
What regional blocks may be done for patient undergoing Carotid Endarterectomy?
What levels must be blocked?
Cervicle Plexus block
Local infiltration
Regional Must cover C2-C4
What reflex can be activated during Carotid Endarterectomy? or following carotid balloon inflation?
Baroreceptor Reflex
A patient in the PACU develops a hematoma following a right endartereacotmy. Her airway is completely obstructed. What is the best treatment at this time?
Patient requires Emergent decompression of surgical site.
Cricothyroidotomy may be required.