Alcoholic and Metabolic Liver Diseases
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
What is the pathophysiology of alcoholic steatosis?
Excess NADH from alcohol metabolism inhibits β‑oxidation → triglyceride accumulation in hepatocytes.
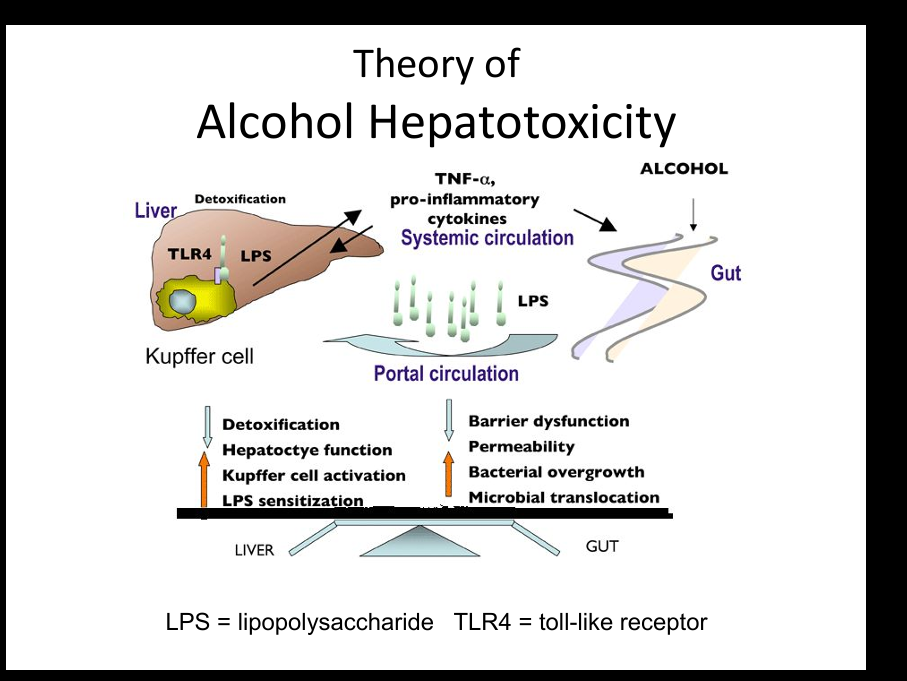
What immune mechanism contributes to alcoholic hepatitis?
Gut permeability ↑ → LPS enters portal blood → activates Kupffer cells → TNF‑α release → inflammation.
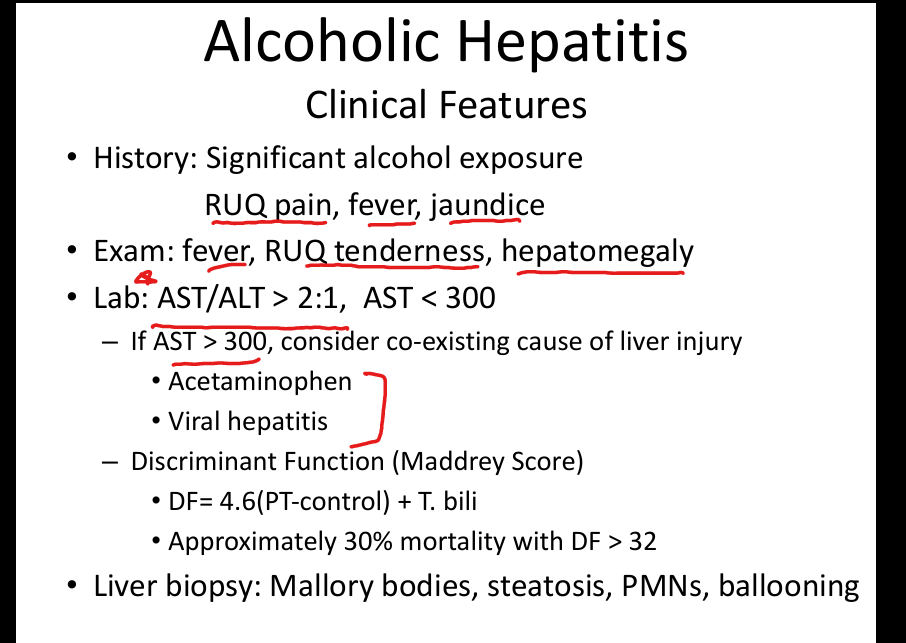
What is the AST/ALT pattern in alcoholic hepatitis?
AST:ALT > 2:1, AST usually < 300 U/L.
Why is AST < 300 in alcoholic hepatitis?
Alcohol deficiency of pyridoxal phosphate (B6) limits ALT production.
What are the clinical features of alcoholic hepatitis?
Fever, RUQ pain, jaundice, tender hepatomegaly.
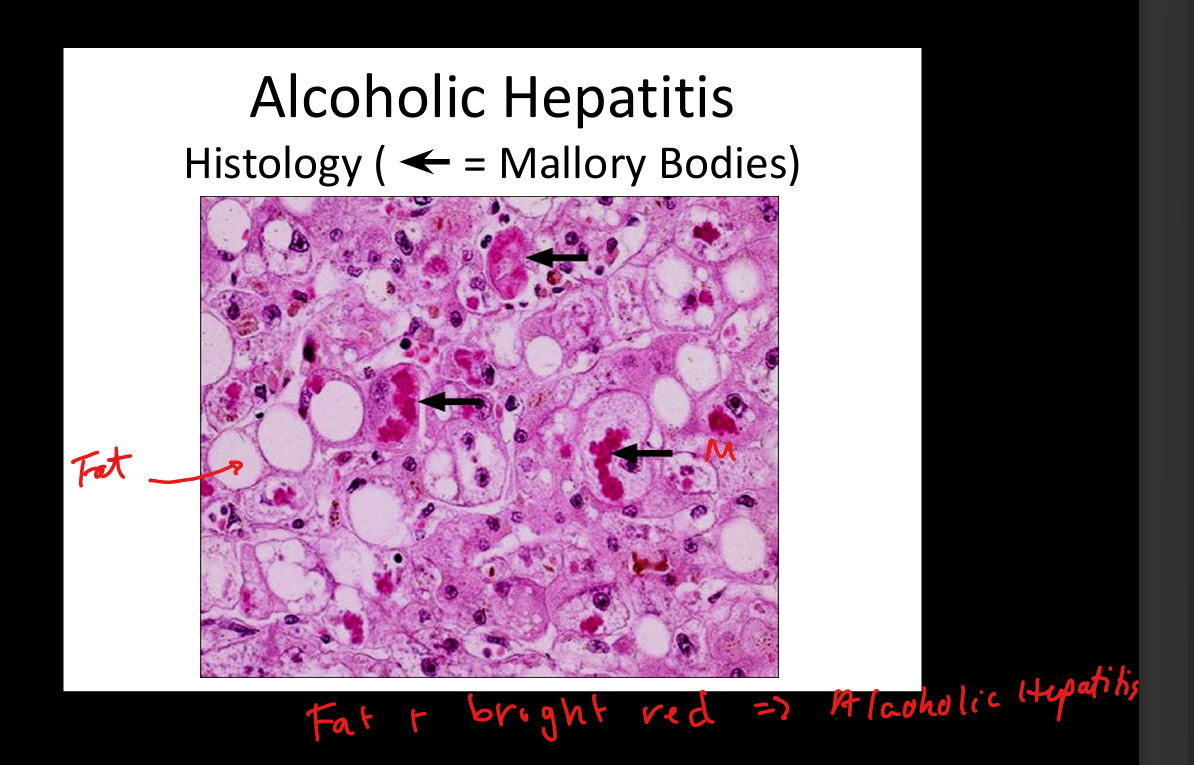
What histologic findings are seen in alcoholic hepatitis?
Mallory bodies, ballooning degeneration, neutrophilic infiltrate, steatosis.
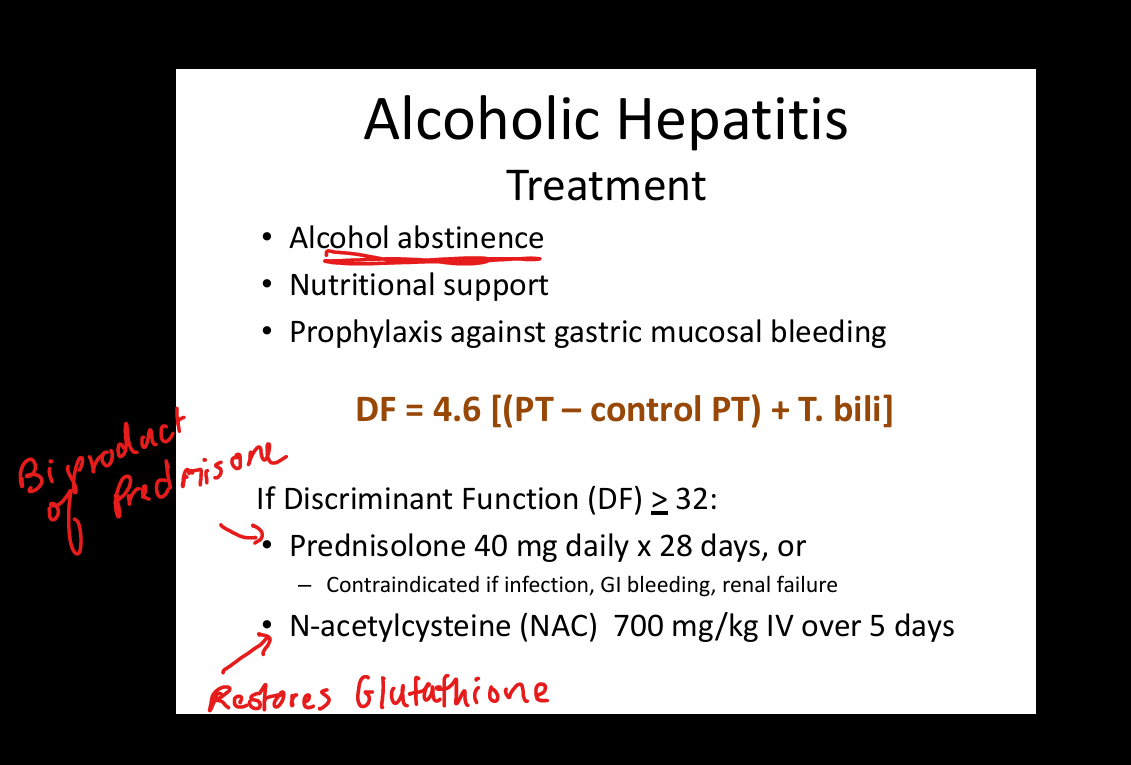
What is the treatment for severe alcoholic hepatitis?
Stop drinking; Prednisolone OR NAC if steroids contraindicated.
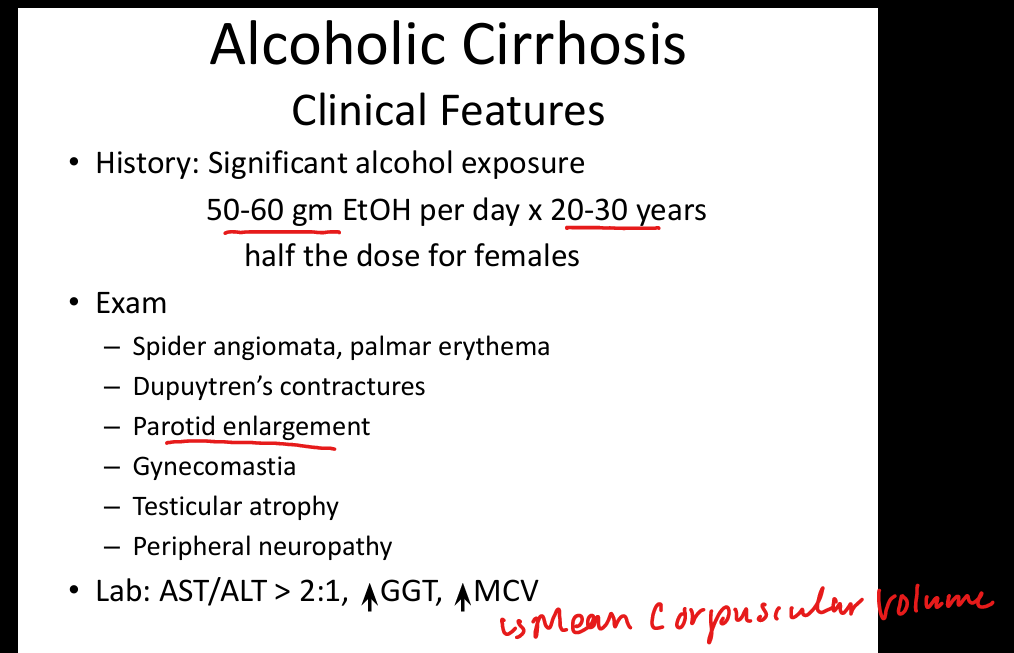
What is the typical alcohol exposure leading to cirrhosis?
50–60 g/day(3.5-4.5 drinks) for 20–30 years (half for women).
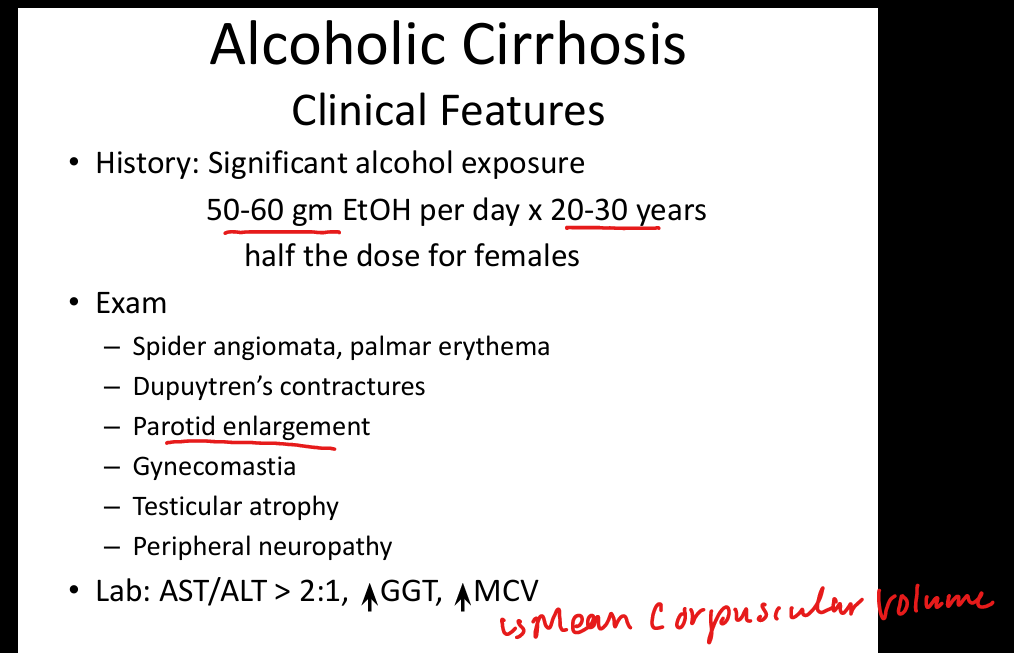
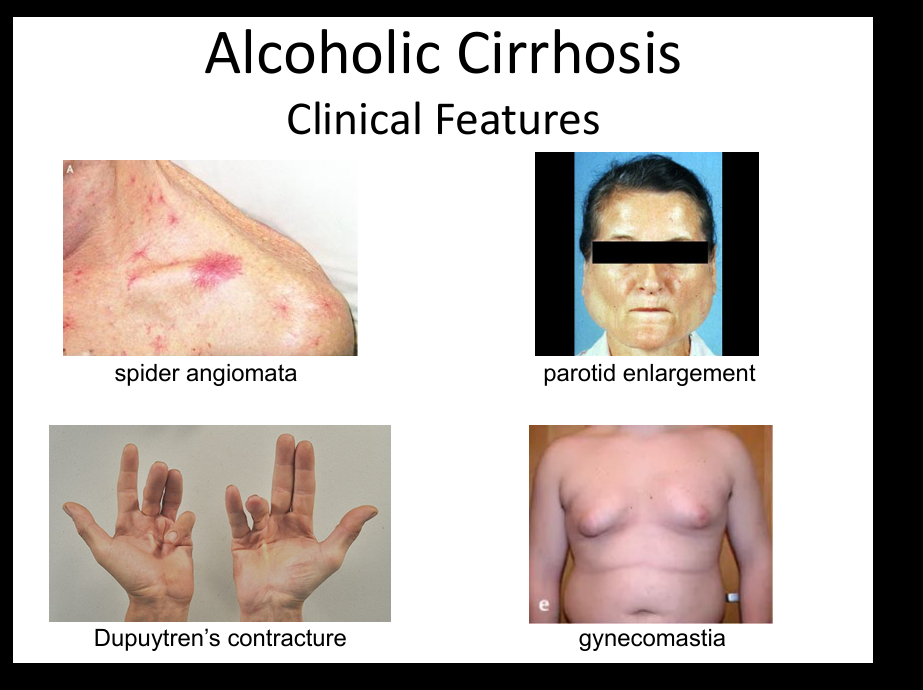
What are physical exam findings in alcoholic cirrhosis?
Spider angiomas, palmar erythema, parotid enlargement, gynecomastia, testicular atrophy, Dupuytren contracture.
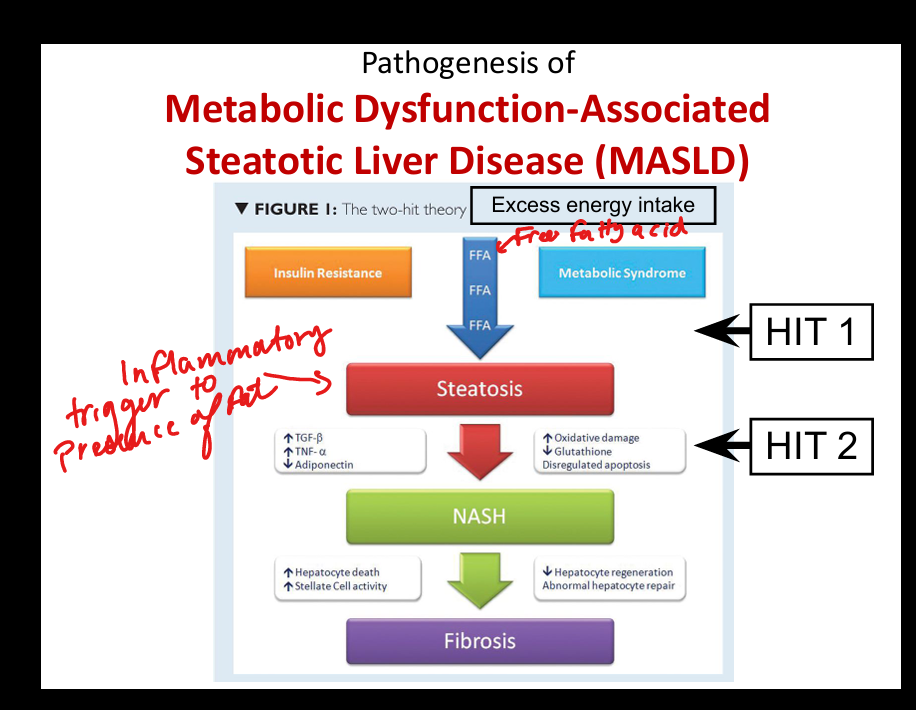
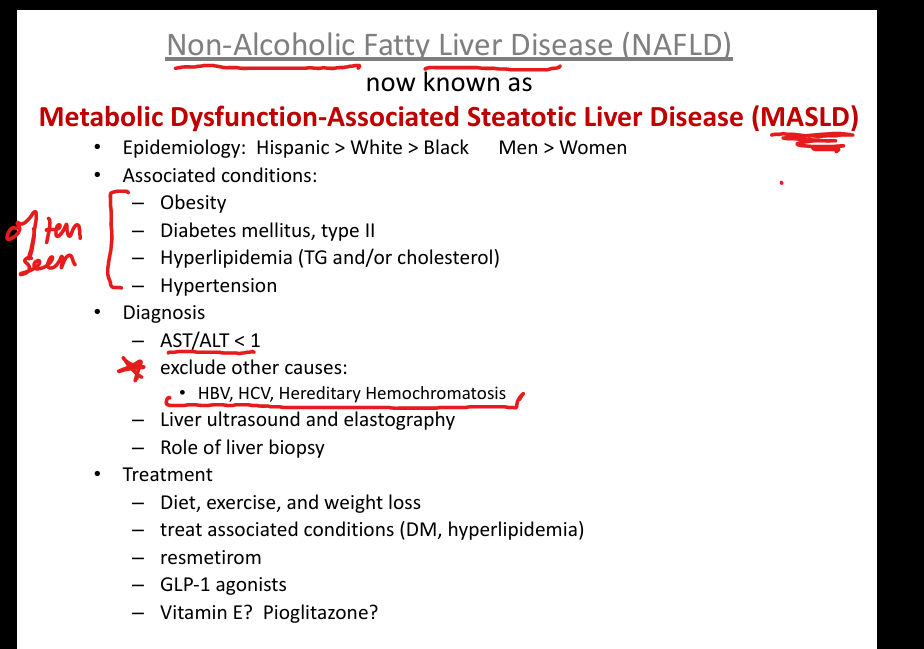
What is MASLD?
Metabolic dysfunction‑associated steatotic liver disease (formerly NAFLD).
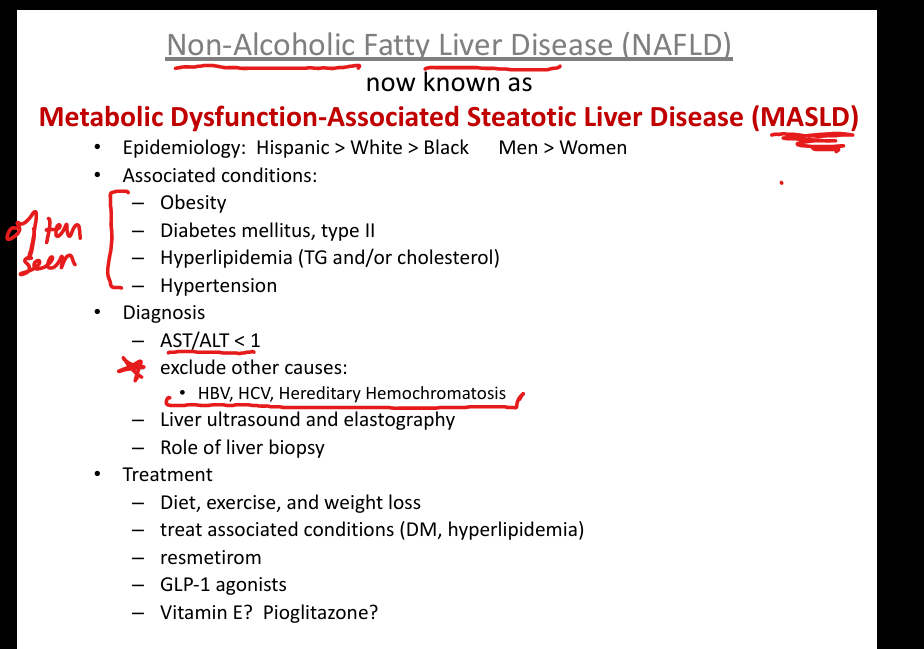
What conditions are associated with MASLD?
Obesity, type 2 diabetes, hyperlipidemia, hypertension.
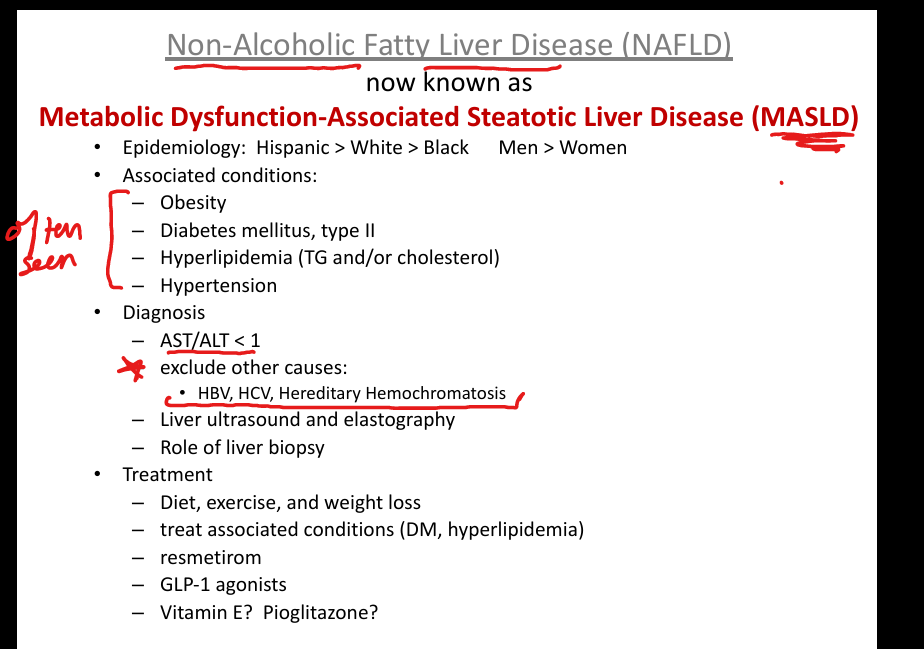
What is the AST/ALT pattern in MASLD?
ALT > AST (AST/ALT < 1).
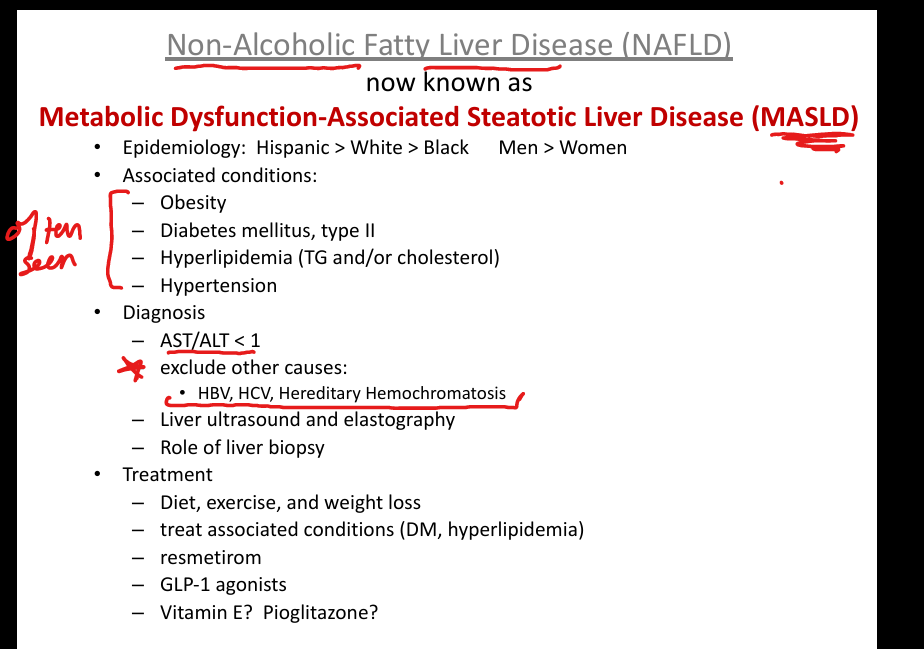
What is the first‑line treatment for MASLD?
Weight loss (≥10%), diet, exercise, treat metabolic syndrome.
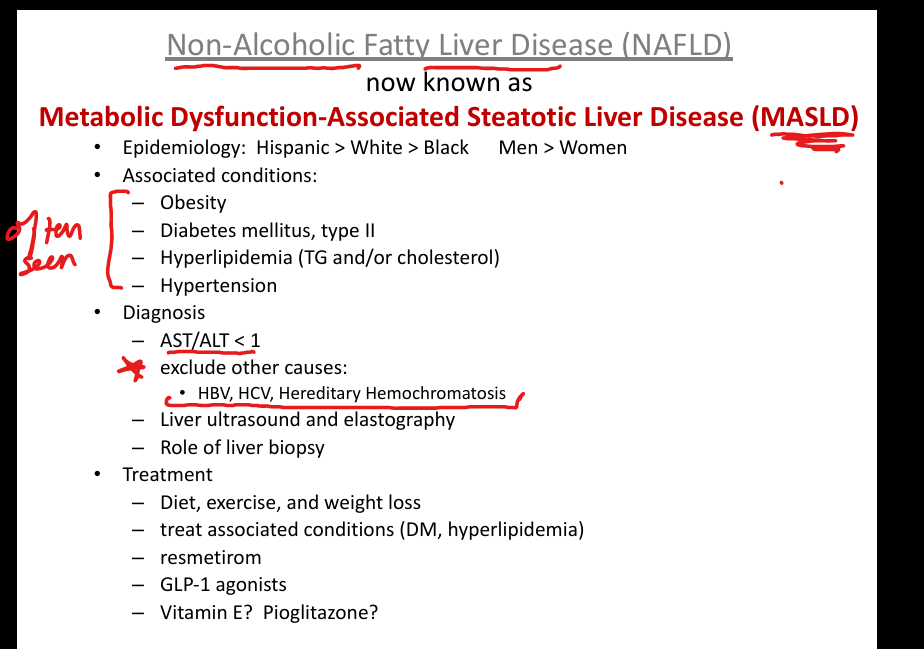
What medications may help MASLD?
GLP‑1 agonists, resmetirom, pioglitazone, vitamin E (non‑diabetics).
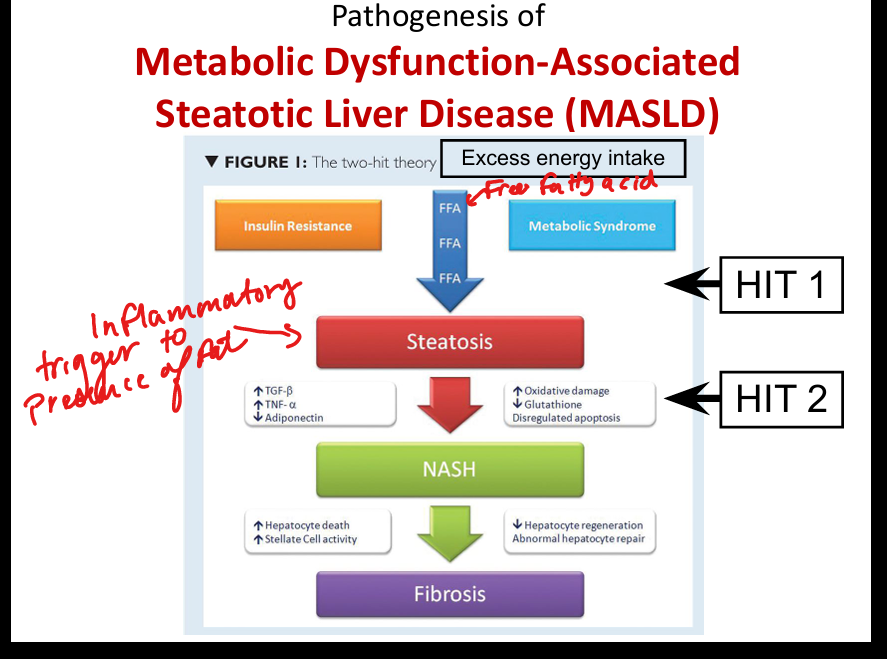
What is the pathogenesis model of MASLD?
Two‑hit theory: steatosis (insulin resistance) → oxidative stress/inflammation → NASH(Non Alcoholic SteatoHepatitis) → fibrosis.
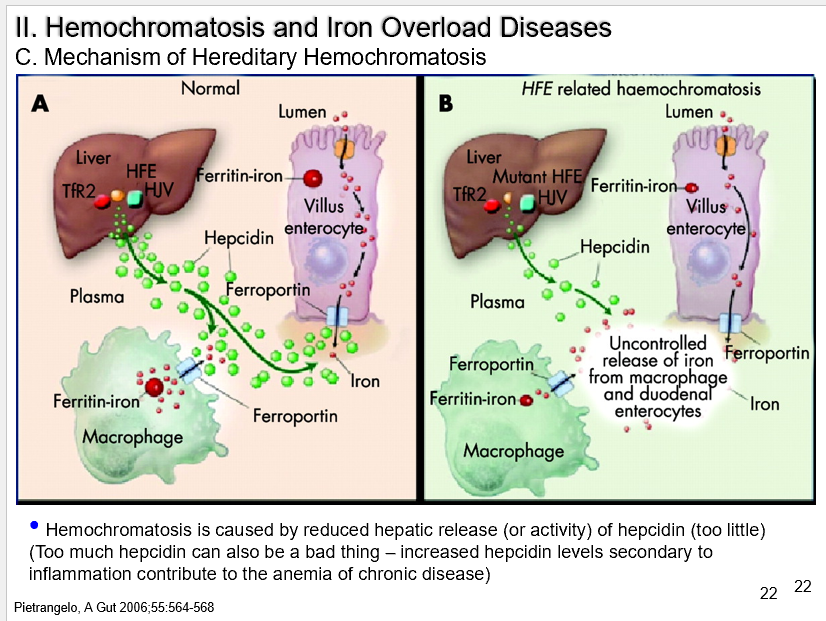
What is hereditary hemochromatosis?
Autosomal recessive HFE mutation → ↓ hepcidin release(used to transport iron)→ ↑ iron absorption → iron overload.
What are the classic symptoms of hemochromatosis?
Bronze(hyperpigmentation) diabetes, arthropathy(joint disease), cardiomyopathy, cirrhosis, fatigue, impotence.
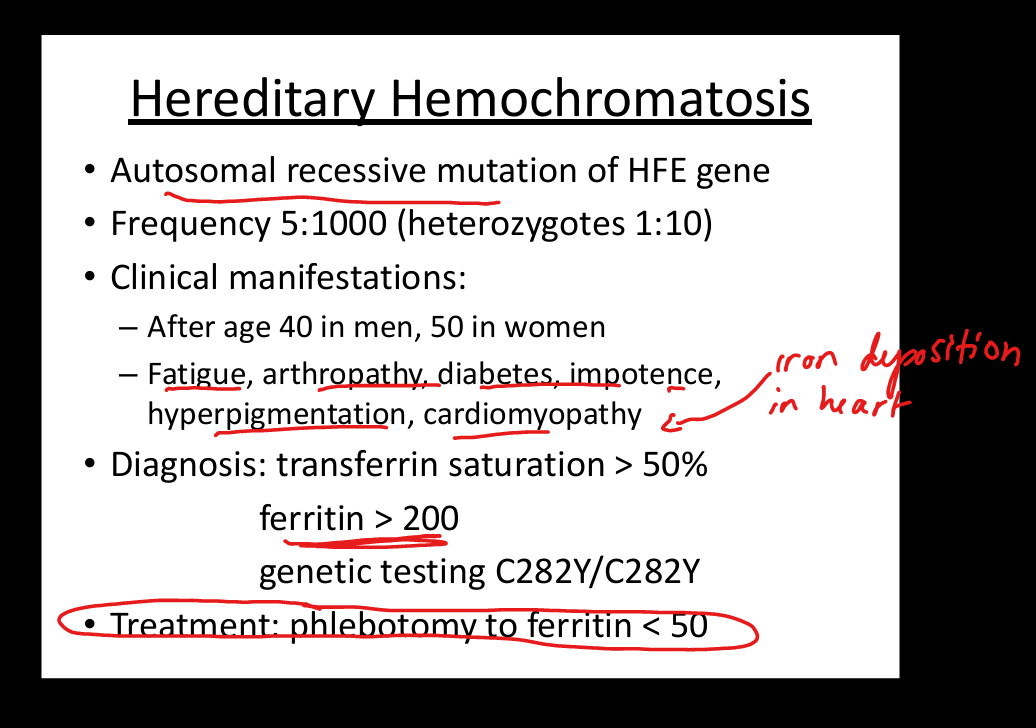
What lab findings suggest hemochromatosis?
Transferrin saturation > 50%, ferritin > 200.
What is the treatment for hemochromatosis?
Phlebotomy to ferritin < 50.
What causes secondary iron overload(Hemochromatosis)?
Due to excess iron intake: Transfusions, sideroblastic anemia, iron cookware/beer brewing.
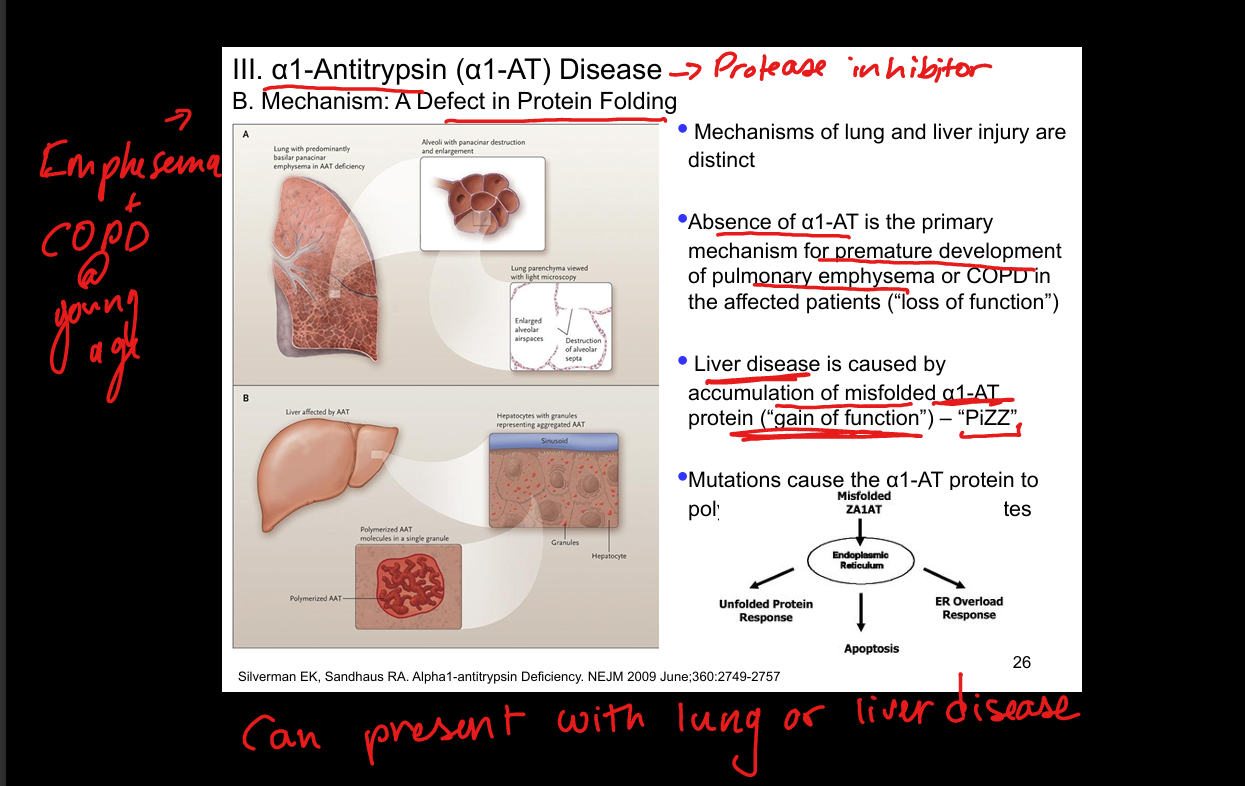
What is alpha‑1 antitrypsin deficiency? Liver vs Lung
Codominant disorder → misfolded A1AT(protease inhibitor) accumulates in hepatocytes → liver disease because of lack of protease inhibitor;
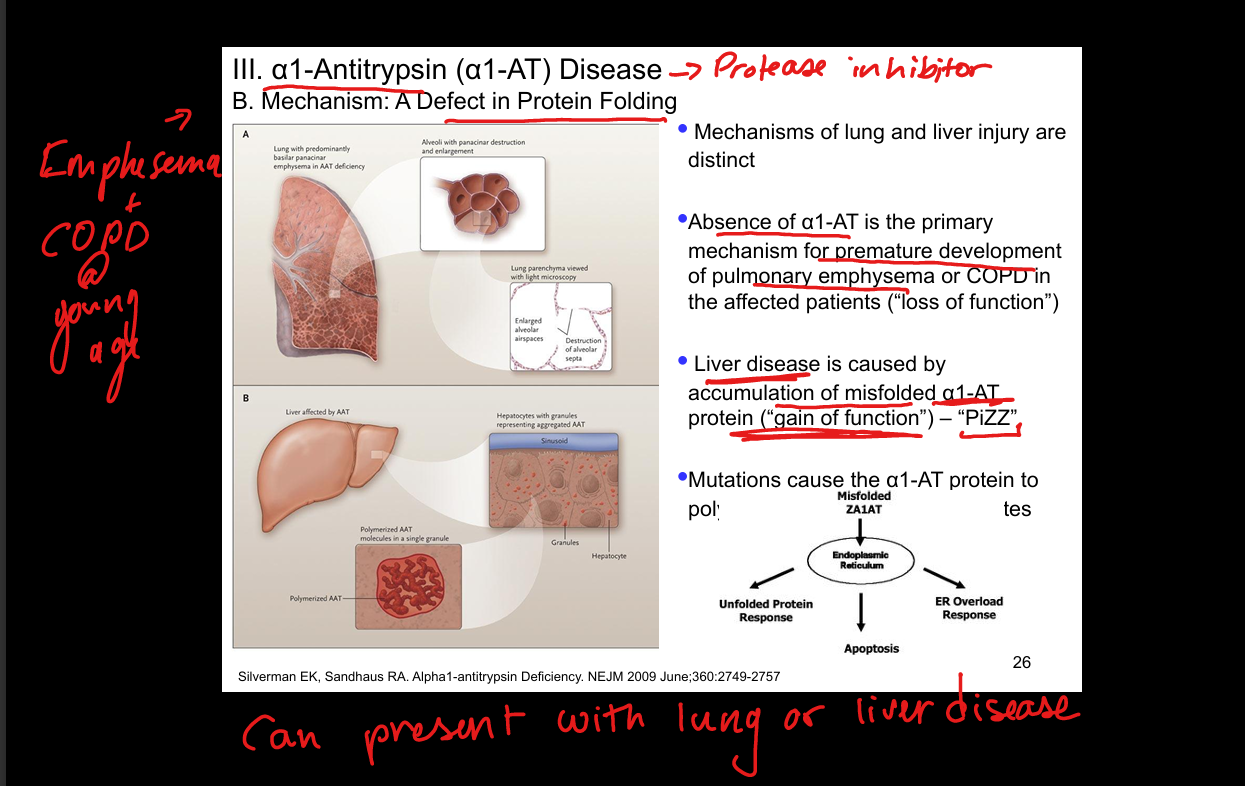
What phenotype is pathogenic in A1AT deficiency?
ZZ phenotype. PiZZ (Protease inhibitor defect of ZZ phenotype)
What is the treatment for A1AT liver disease?
Liver transplantation.
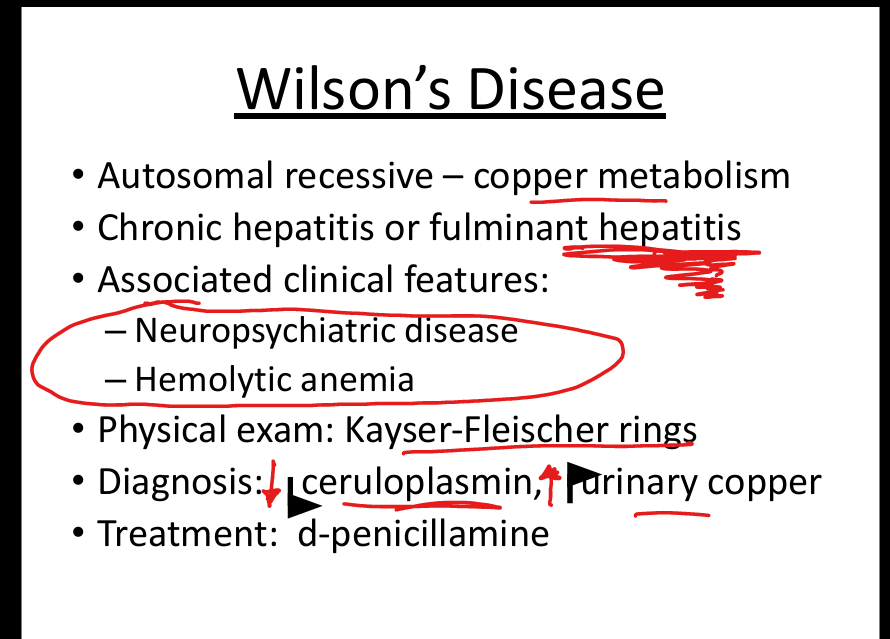
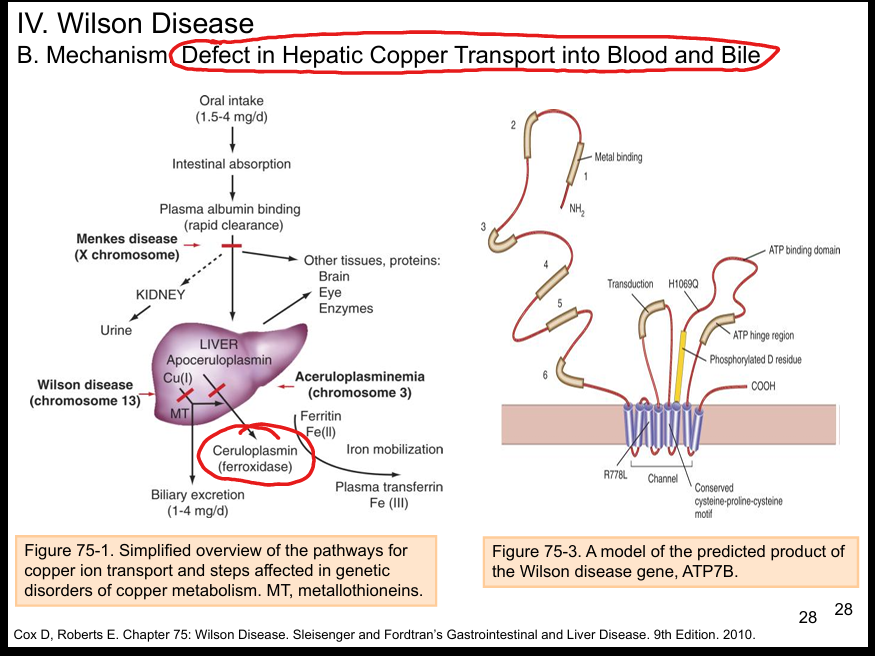
What is Wilson disease?
Autosomal recessive ATP7B mutation → impaired copper excretion → copper accumulation.
What are clinical features of Wilson disease?
Neuropsychiatric symptoms, hepatic failure, hemolytic anemia.
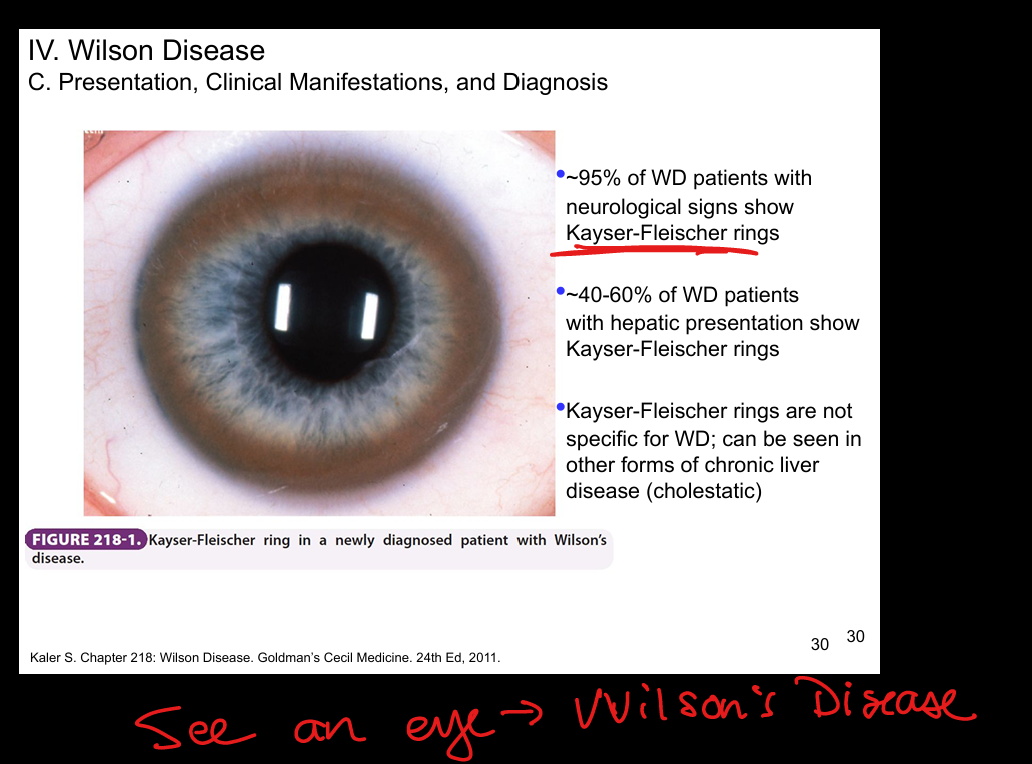
What eye finding is seen in Wilson disease?
Kayser‑Fleischer rings. (brown copper deposits in the eyes)
What labs diagnose Wilson disease?
Low ceruloplasmin, ↑ urinary copper.
What is the treatment for Wilson disease?
D‑penicillamine (binds and removes copper).