Ableism, Disability, and Veteran Health
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
What is Disability according to the CDC?
any condition of the body or mind that makes it more difficult for the person with the condition to do certain activities and interact with the world around them

What is Disability according to the Americans with Disabilities Act?
a person who has a physical or mental impairment that substantially limits one or more major life activities

What is Disability according to the World Health Organization?
refers to the interaction between individuals with a health condition and personal and environmental factors
What is Disability according to the Scope (UK)?
people are disabled by barriers in society, not by their impairment or difference in which barriers can be physical….Or they can be caused by people's attitudes to difference, like assuming disabled people can't do certain things
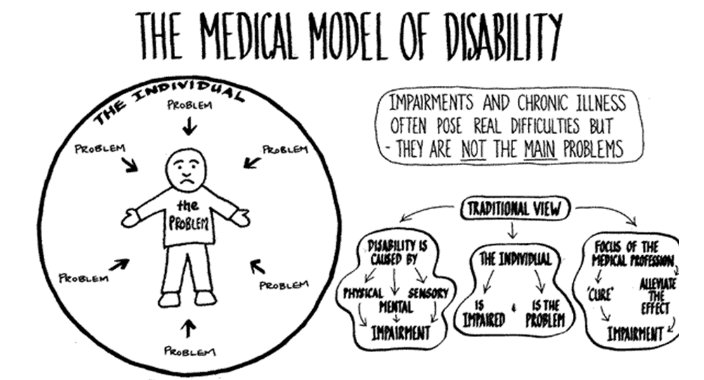
Medical Model:
sees disability as a problem that needs medical intervention and the individual needs to be changed
“fixing” the disability
being disabled is negative
society remains the same
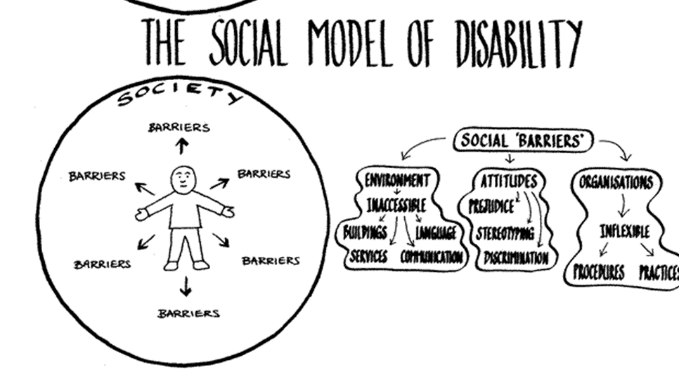
Social Model:
sees environment as causing an impairment to become disabling and disability is not inherent to the individual
Environment/society needs to be changed
being disabled is neither positive nor negative
society evolves to become more inclusive
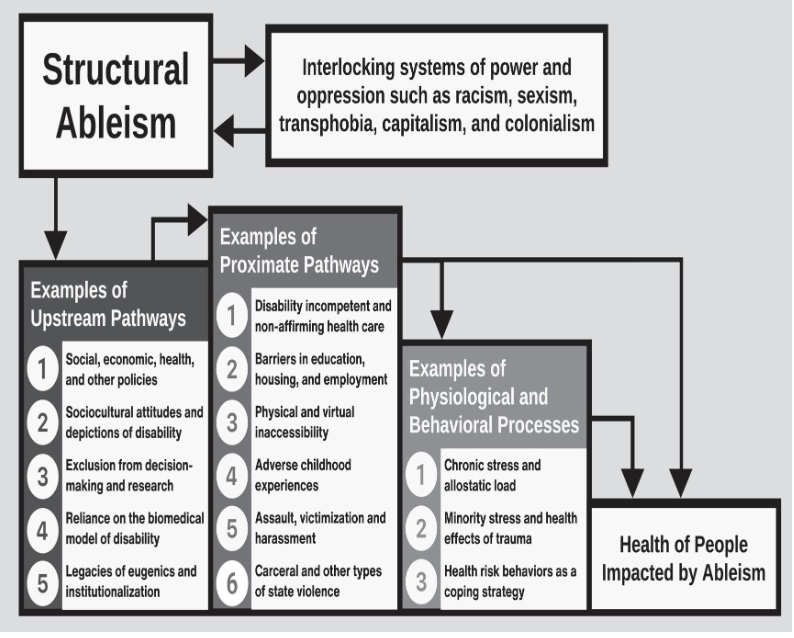
Strutural ableism:
a system of historical and contemporary policies, institutions, and societal norms and practices that devalue and disadvantage people who are disabled, neurodivergent, chronically ill, and/or living with mental illness and privilege people who are positioned as able-bodied and able-minded
explains how systems, institutions, and policies reproduce inequality
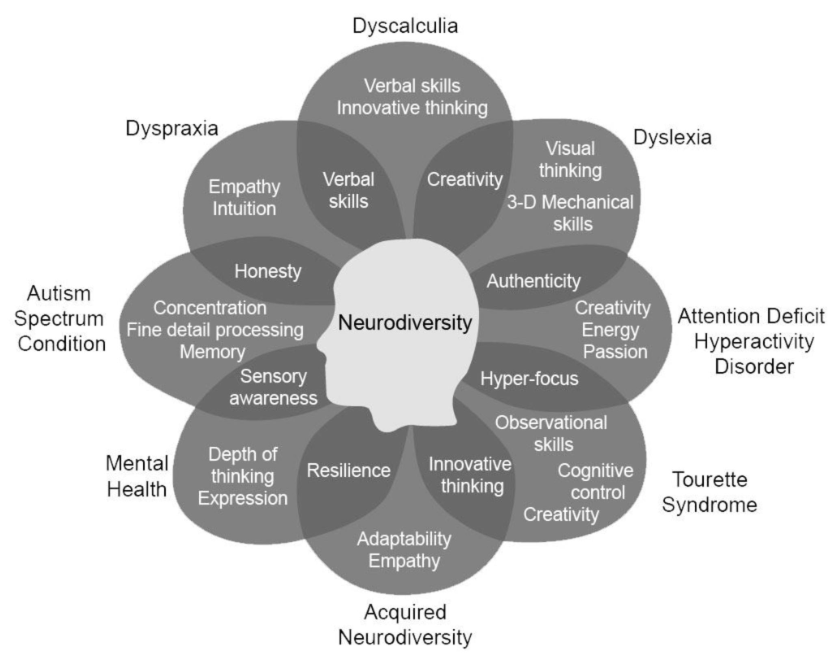
Neurodiversity:
often applied to conditions affecting behavior, mood or thought processes (e.g. autism, depression, mania, psychosis) and there's no “correct” way for the brain to work
wide range of ways that people perceive and respond to the world, and these differences are to be embraced and encouraged
Diverging from social norms is not indicative of pathology
May or may not be covered under the American Disabilities Act
Ableism in Healthcare:
inaccessible medical facilities and equipment and we see that staff assume people with disabilities view all symptoms or traits as a disease
behaviors, such as the failure of a health care provider to discuss reproductive health issues based on assumptions about a person’s ability to conceive
Stereotypes → study found that 82% of doctors in the United States believed that people with disabilities had worse quality of life than non- disabled people

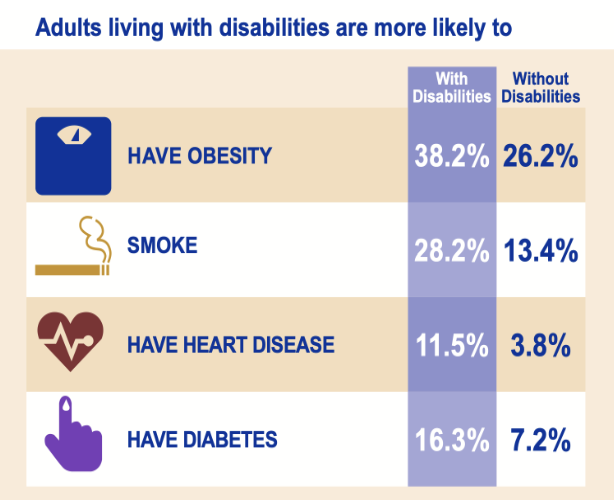
Health Disparities in Disability:
people with disabilities are more likely to report poor health and experience higher rates of chronic health conditions than nondisabled people and those with multiple disabilities had worse health outcomes and that people with hearing disabilities fared better on most outcomes than people with vision, physical, or cognitive disabilities
Who counts as a Veteran?
person who served in the active military, naval, or air service and was discharged or released under conditions other than dishonorable
character of discharge is itself a structural determinant of health
Veterans with non-honorable discharges are excluded from most VA care and benefits, and that exclusion is not distributed equally across the population
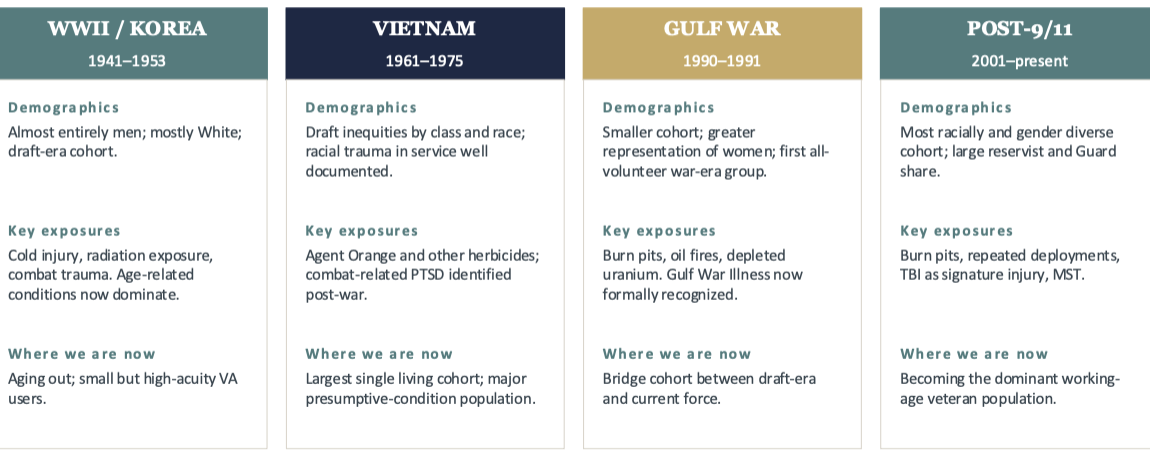
True or False: Veterans are not one cohort.
True, different eras carry different demographics, exposure histories, and policy contexts into the VA system today
How is health shaped before service?
has selection into service
Socioeconomic background
Educational opportunity
Adverse childhood experiences
Neighborhood and rurality
How is health shaped during service?
has service-related exposures
Combat and operational stress
Environmental and chemical exposures
Military sexual trauma
Discrimination within ranks
How is health shaped after service?
has a reintegration context
Employment, income, housing
Geographic access to care
Eligibility, paperwork, and bureaucracy
Social support and community
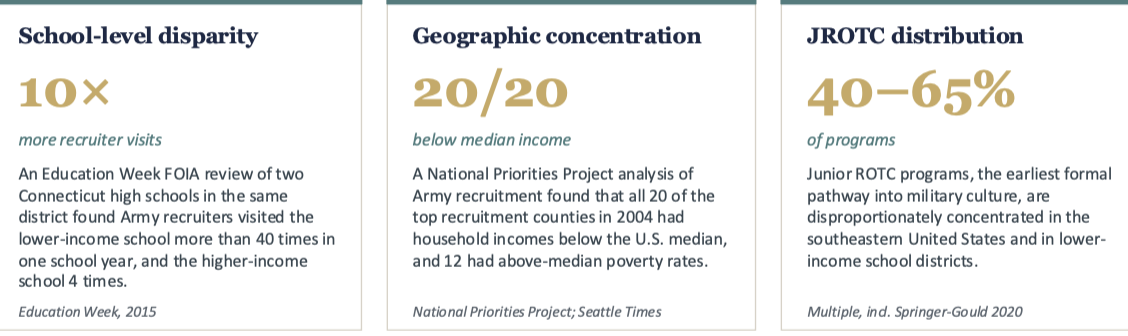
Recruitment is what?
is patterned, not random which is important because the disparities we've seen today don't begin in uniform in which communities that supply the most recruits are also the communities with fewer civilian opportunities, more constrained healthcare access, and more pre-existing structural disadvantage
service does not erase those conditions; it carries them forward
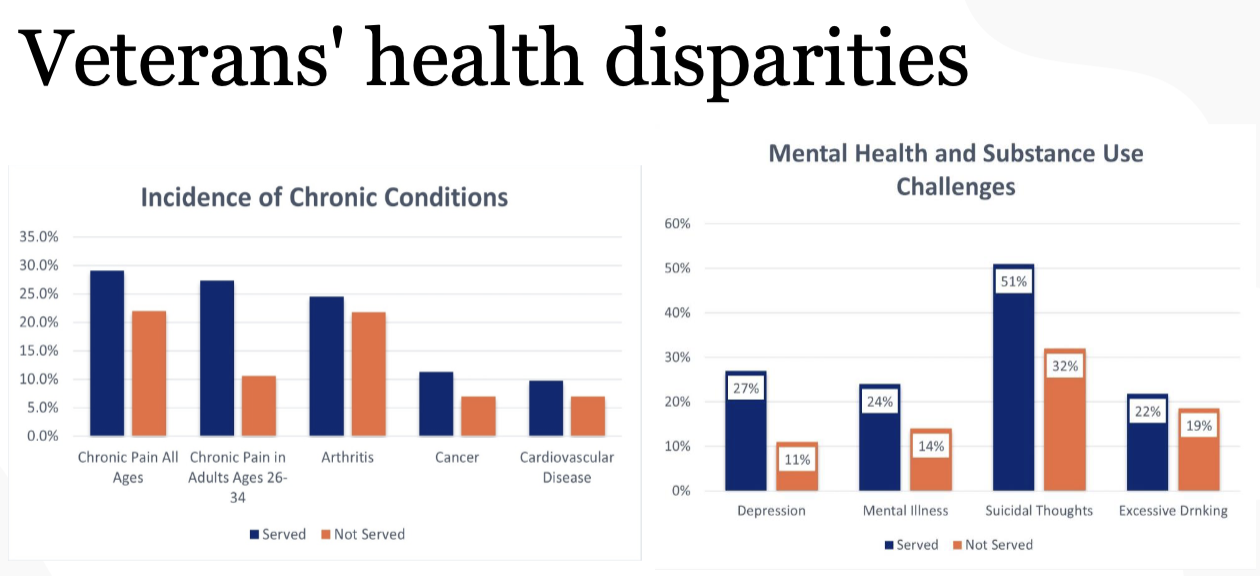
What are some of the burdens veterans have?
physical, mental, and social distinctiveness
musculoskeletal, toxic exposures, traumatic brain injury
PTSD, substance use, housing and employment

Veterans Health Administration (VA):
largest integrated health care system in the U.S. where Veterans with a qualifying discharge (other than dishonorable) are generally eligible and most enlistments after September 7, 1980 require 24 continuous months of active service, or the full period the person was called to active duty
priority for care is then assigned by service-connected status, income, and other factors
Why are there still disparities despite having the VA?
even within a high-performing integrated system, the structures around it shape who gets care and what that care looks like
eligibility design
geographic access
workforce and wait times
fragmentation across systems

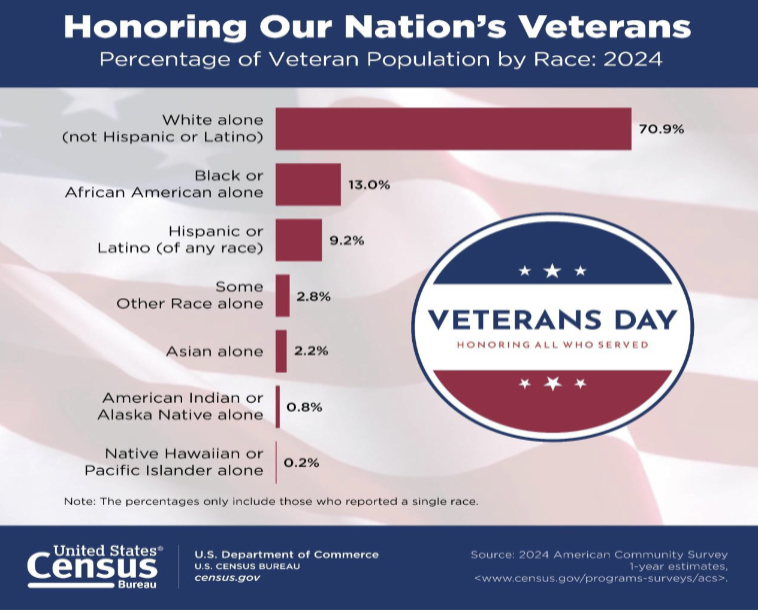
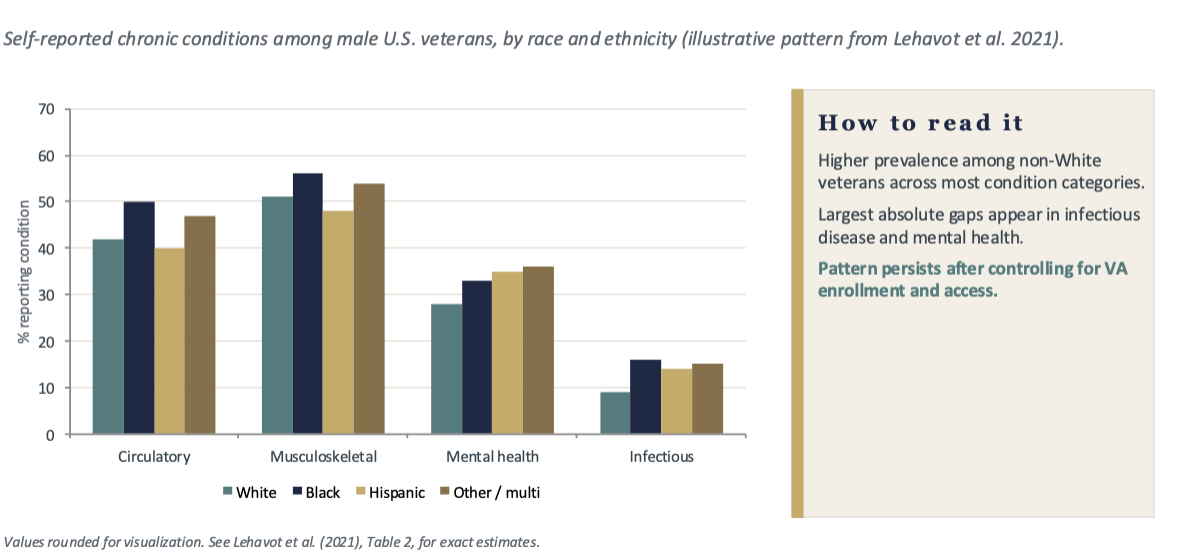
What are the disparities by race and ethnicity?
Self-rated health → Black, Hispanic, and other-race veterans report worse self-rated health than White veterans, after age standardization
Disease burden differs by group → Compared with White men, Black and other-race men report more circulatory, musculoskeletal, mental health, and infectious disease conditions; Hispanic men report higher mental health and infectious disease burden
Combat exposure and utilization → Minority veterans report greater combat exposure and higher VA utilization, suggesting both heavier upstream exposure and continued reliance on VA care
Disparities persist despite comparable VA access → Differences remain even where access is, on paper, equal. This is the central finding of the access vs. equity distinction
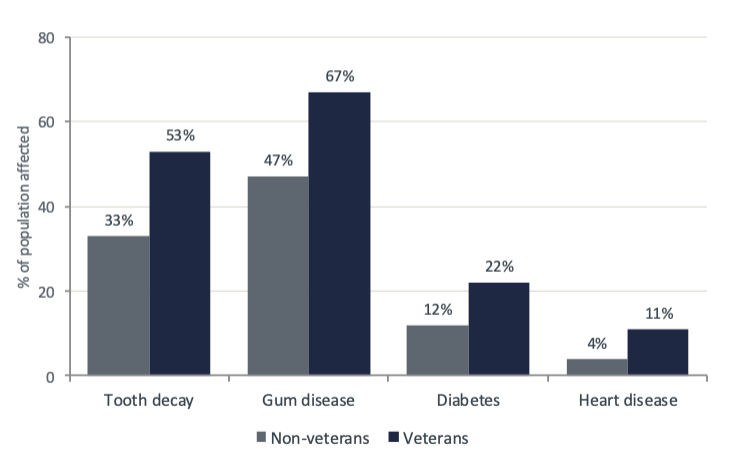
Dental care Gap in Veterans:
we see Oral health gap in Veterans are roughly 60% more likely to have tooth decay and 42% more likely to have gum disease than non-veterans which stacks of Periodontal disease worsens glycemic control and cardiovascular risk → untreated oral disease is a chronic disease accelerant
Chronic disease gap
Women and connection to Veterans:
among women veterans, lifetime PTSD prevalence is the highest of any demographic group studied, even after adjustment for age and race
Reproductive, maternal, and gynecologic services were a late addition to the VA model and remain unevenly available across facilities
MST is a recognized service-connected exposure with downstream effects on PTSD, depression, and chronic pain. Disclosure and care pathways differ markedly by facility
Women veterans face documented gaps in service-connected disability ratings and post-service economic outcomes relative to their service profile

What can we do for Veterans?
Sustained, predictable VA funding
Community-based bridges
Wraparound housing and employment
Integrated, identity-affirming MH care
