Neuro Exam 2
1/192
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
193 Terms
gray matter is located _________ in the spinal cord and contains ___________
centrally, cell bodies
ventral horn of spinal cord
contains motor nuclei for innervation of skeletal muscle located primarily in laminae IX
cervical enlargement
C3-T1
- contains more grey matter in ventral horns for brachial plexus
- contains more white matter bc of ascending and descending tracts
lumbar enlargement
L1-S2
- contains more grey matter in ventral horns for lumbo sacral plexus
* there is not significantly more white matter bc this portion only contains ascending tracts of lumbosacral region
anterior spinal artery supplies the ventral ______ of the spinal cord
2/3
posterior spinal arteries supply dorsal ______ of the spinal cord
1/3
radicular arteries of the aorta supply ?
T3 and above
great radicular artery of adamkiewicz
supplies T9-T12
- provides blood supply to lumbar and sacral cord
vulnerable zone
area highly susceptible to stroke, mid thoracic area (T4-T8)
transverse cord syndrome
-entire cord affected equally at that level
- affects all ascending and descending tracts
- paralysis below lesion
anterior cord syndrome
- can be caused by infarct to to anterior spinal artery, or lesion/ trauma
- ALS damaged bilaterally and damage to LCST
LMNs begin in the __________, so damage causes LMN signs ____________ of the lesion and UMN signs ___________
anterior horn, at the level, below
posterior cord syndrome
- can be caused by damage to the posterior spinal artery
- damage to DCML only

a patient with transverse cord syndrome would have what signs?
-loss of pain and temp (ALS)
- loss of proprioception, vibration, and light discriminative touch (DCML)
- LMN signs at lesion and UMN signs below (LCST)
*paralysis below lesion

a patient with anterior cord syndrome would have what signs?
- loss of pain and temperature (ALS)
- LMN signs at lesion and UMN signs below (LCST)
a patient with posterior cord syndrome would have what signs?
- loss of proprioception, vibration, and light discriminative touch (DCML)
central cord syndrome
- medial aspects of the cord are damaged, causing more UE signs than LE (because of somatotopy)

a patient with central cord syndrome would have what signs?
- loss of proprioception, vibration, light touch (DCML)
- loss of pain and temperature (ALS)
- LMN signs at level of lesion and UMN signs below (LCST)
more prominent in the UE than the lower
brown- sequard (hemicord) syndrome
- only one side of the spinal cord is damaged
- causes ipsilateral loss in LCST and DCML
*remember ALS crosses over in the spinal cord so information cannot get in at the level of lesion and information ascending from other side cannot continue

a patient with hemicord syndrome would have what signs ?
-ipsilateral weakness (LCST)
- ipsilateral loss of vibration, proprioception, light touch (DCML)
- ipsilateral loss of pain and temperature at the level of the lesion, contralateral loss below the level of the lesion (ALS)
complete impairment is classified as ______ on the ASIA scale
AIS A
incomplete impairment is classified as ___________ on the ASIA scale
AIS B, C or D
normal classification on the ASIA scale
AIS E
ASIA overview
-sensory exam: sharp/dull, light touch, deep anal sensation
- motor exam
- classification
__________ is tested at all levels, ___________ is only tested from C5-T1 and L2-S1
sensory, motor
steps for ASIA classification
1. determine sensory level
2. determine motor level
3. determine neurological level of injury
4. determine if complete or incomplete injury
4a. determine ZPP
5. determine AIS grade
determining sensory level ASIA
test light touch and sharp dull at each dermatome level compared to face
- sensory level is the most caudal intact dermatome for both pin prick and light touch sensation
ex. c4= 2, c5= 1 c6=0
level would be c4
grading system for sensory system
0= absent, cant distinguish sharp vs dull
1= impaired, feels different than face
2= normal
C2 dermatome
1 cm lateral to the occipital protuberance/ 3cm behind the ear
C3 dermatome
supraclavicular fossa, at the mid clavicular line
C4 dermatome
over the acromioclavicular joint
T2 dermatome
apex of axilla
thoracic dermatomes should always be tested ___________
at the midclavicular line, closer to center of the body
S3 dermatome
over the ischial tuberosity or infragluteal fold
S4/S5 dermatome
in the perianal area less than 1 cl lateral to the mucocutaneous junction
deep anal pressure
if S4/S5 light touch and pin prick sensation is absent, check for sensation to pressure in the internal anorectal wall
determining motor level
10 key muscles are tested (same as myotome testing)
- graded 0-5
- lowest key muscle function that has a grade of atleast 3 given the muscle above is a 5
ex. c5=5, c6=3, c8=2 motor level is c6
asterisk on ASIA exam
used when an impairment is already present in the patient that impacts the examination results, not related to spinal cord injury
*if present above level of lesion it is normal, if it is below the level of the lesion it is considered not normal
voluntary anal contraction
when testing DAP, ask patient to squeeze finger to test sacral motor function
- could be only sign that someone has an incomplete injury
motor grades are found to be C5= 5, C6= 4, C7= 3, C8= 2
what is the motor level?
C6
special considerations for motor testing
when there is no myotome that is testable the motor level is presumed to be the same as the sensory level, if testable motor function above is also normal
all sensation from C2- C4 is normal, when performing the motor test C5= 4 and C6= 3
what is the motor level?
C5
determining neurological level of injury
most caudal segment of the cord with intact sensory and motor levels
motor level is found to be C6 on the right and C6 on the left, sensory level is found to be C4 on the right and C5 on the left
what is the neurological level of injury?
C4
if there is no VAC or DAP, and all S4-5 sensory scores are 0 the injury is _________
complete
(N0000N)
zone of partial preservation
for injuries with absent VAC or DAP only- record most caudal level with any innervation
AIS B
injury is motor complete, but sensory incomplete
VAC is a no
AIS C
motor injury is incomplete and less than half of the key muscles below the NLI are a grade 3 or better
AIS D
motor injury is incomplete, but at least half of the key muscles below the NLI are a grade 3 or better
A patient has 5 key muscles below their NLI. Two of the muscles on the right have a grade of 3 or higher, and four of the muscles on the left have a 3 or higher.
How would you score and what is the AIS grade?
6/ 10 = 60%
AIS D
layers of the scalp
-skin
-subcutaneous connective tissue
- galea aponeurotica
- loose areolar connective tissue
- pericranium
meningeal layers folds into the cranial cavity to form ___________
falx cerebri and tentorium cerebelli
epidural space
space between the skull and dura
subdural space
space between dura mater and arachnoid mater
subarachnoid space
between arachnoid and pia mater
- always filled with CSF
- contains major arteries of the brain
t or f: the subdural and epidural spaces are true spaces filled with CSF
false
arachnoid trabeculae
fine filament connecting the arachnoid to the pia mater
flow of CSF
produced in choroid plexus
lateral ventricles
foramen of monro
third ventricle
cerebral aqueduct
fourth ventricle
foramen of magendie
epidural hematoma cause
usually from temporal bone fracture and middle meningeal artery rupture
- initially no sxs but can elevate to ICP, herniation, and death within hours
lucid interval
Period of consciousness after head injury
subdural hematoma cause
rupture of bridging veins which are susceptible to shear injury as they cross arachnoid into dura
- crescent shape forms as blood spreas
chronic subdural hematoma
common in elderly as brain is able to move more freely due to atrophy and bridging veins are susceptible to shear (can occur from minimal trauma)
- venous blood collects for weeks to months = vague sxs
- HA, cognitive impairment, unsteady gait
acute subdural hematoma
occurs from a traumatic injury with high impact velocity
- serious and worse prognosis
subarachnoid hemorrhage on CT scan
blood will be seen in the contours of the brain sulci
traumatic subarachnoid hemorrhage
bleeding into CSF from damaged vessels due to contusion and traumatic injury
- severe HA due to meningeal irritation from blood in CSF
- deficits are usually from other cerebral injuries present
spontaneous subarachnoid hemorrhage
caused by rupture of arterial aneurysm, usually in the anterior circulation (Acomm, Pcomm, MCA)
- sudden catastrophic headache
- can have neurodeficit, impaired LOC, coma and death
- risk of rebleeding
delayed cerebral vasospasm
concern for spontaneous subarachnoid hemorrhage
- occurs 3-4 days after and peaks at 10 days
- occurs in about 50% of patients leading to ischemia and infarction
traumatic intracerebral hemorrhage
-contusions of cerebral hemispheres occur where cerebral gyri are immediately adjacent to ridges of the skull
-most common at temporal and frontal poles
- coup/ contrecoup
hydrocephalus
- excess CSF fluid in intracranial cavity
- caused by excess CSF production, obstruction of flow, or decrease in reabsorption (must be drained)
- sxs of shuffling gait, incontinence, mental decline
increased intracranial pressure
-can happen suddenly or slowly leading to irreversible brain injury or death
- key sxs- altered mental status, lower consciousness and irritable
- can be lowered by meds, ventricular drainage, induced coma, hemicraniectomy
headache
- can be caused by mechanical traction, inflammation, irritation or other structures with innervation
- can be classified as vascular, tension-type, or secondary
brain parenchyma has no pain receptors so pain is felt by __________
tissue around the brain
vascular headache
likely from inflammatory, autonomic, sertogenic, neuroendocrine, or other influences on blood vessel diameter
migraine
type of vascular headache, common with family history
- multiple triggers such as food, stress, sleep
- proceeded by aura/ blurry vision
- worse with light, noise, sudden head movement
cluster headache
occurs in a specific part of the head, goes away and comes back
tension headache
steady dull ache in a band like sensation lasting for a few hours
- chronic can happen daily for years and associated with stress or trauma
- treated with relaxation and NSAID
secondary headache
headache with an identifiable underlying cause such as trauma, hemorrhage,, low CSF pressure, epidural abscess, meningitis
dominant hemisphere
the side of the brain that provides analytic, language, logic, and math skills; in most individuals, the left hemisphere
- includes brocas and wernickes area
nondominant hemisphere
the side of the brain associated with sensitivity to the emotional tone, intuition, creativity, and spatial processing; in most individuals, the right hemisphere
- includes association cortex
primary visual cortex
located on the medial occipital lobe
anterior circulation of the brain
aorta/ brachiocephalic arteries→ common carotid→ internal carotid
posterior circulation of the brain
subclavian → vertebral → basilar→ posterior cerebral (PCA)
circle of willis
-internal carotid
- MCA
- ACA
- Acomm
-Pcomm
- PCA
the internal carotid artery gives off _________
- middle cerebral artery
- anterior cerebral artery
the vertebral artery gives off________
- PICA
- basilar
branches of the basilar artery
-anterior inferior cerebellar artery
-superior cerebellar arteries
- posterior cerebral arteries
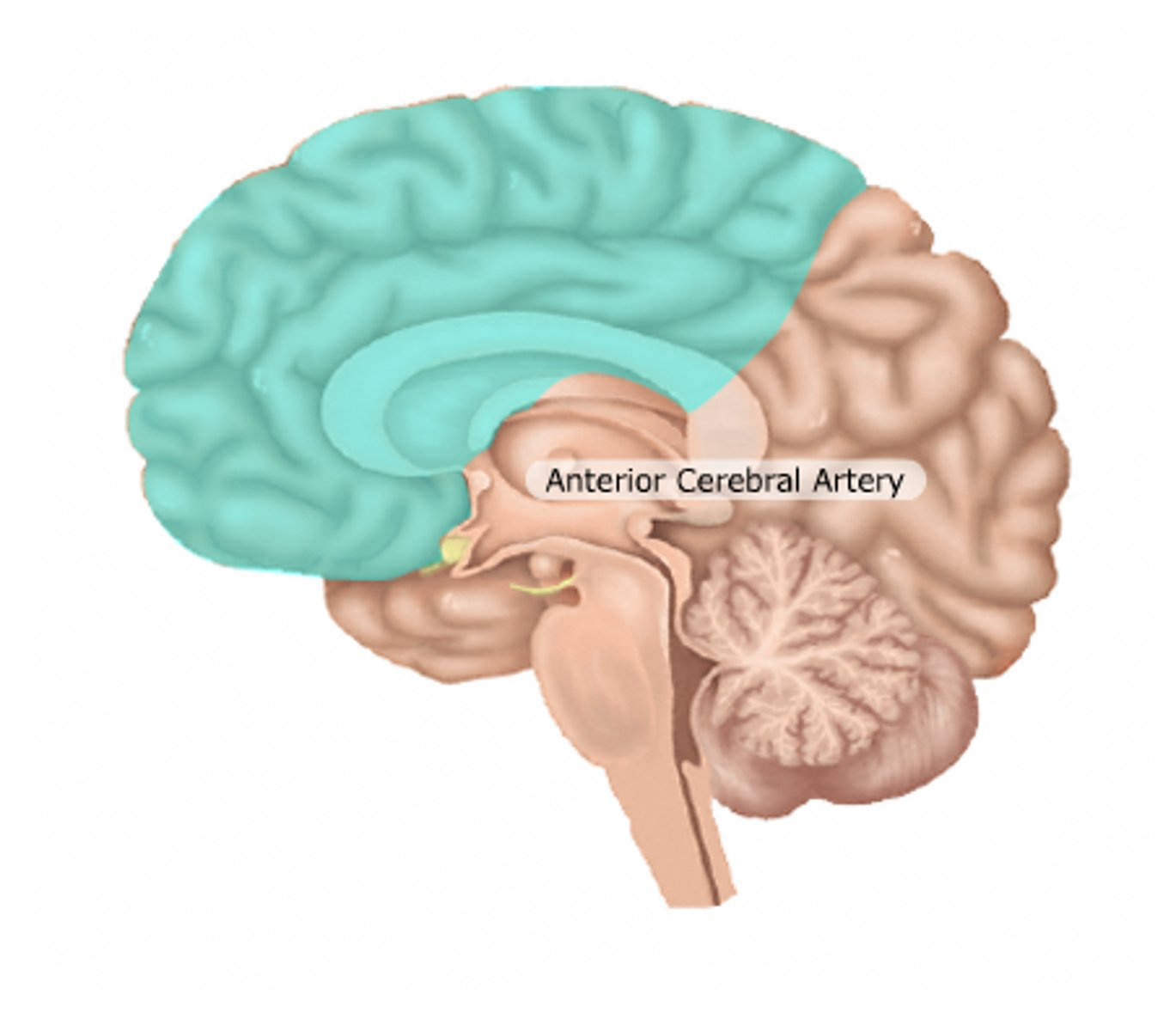
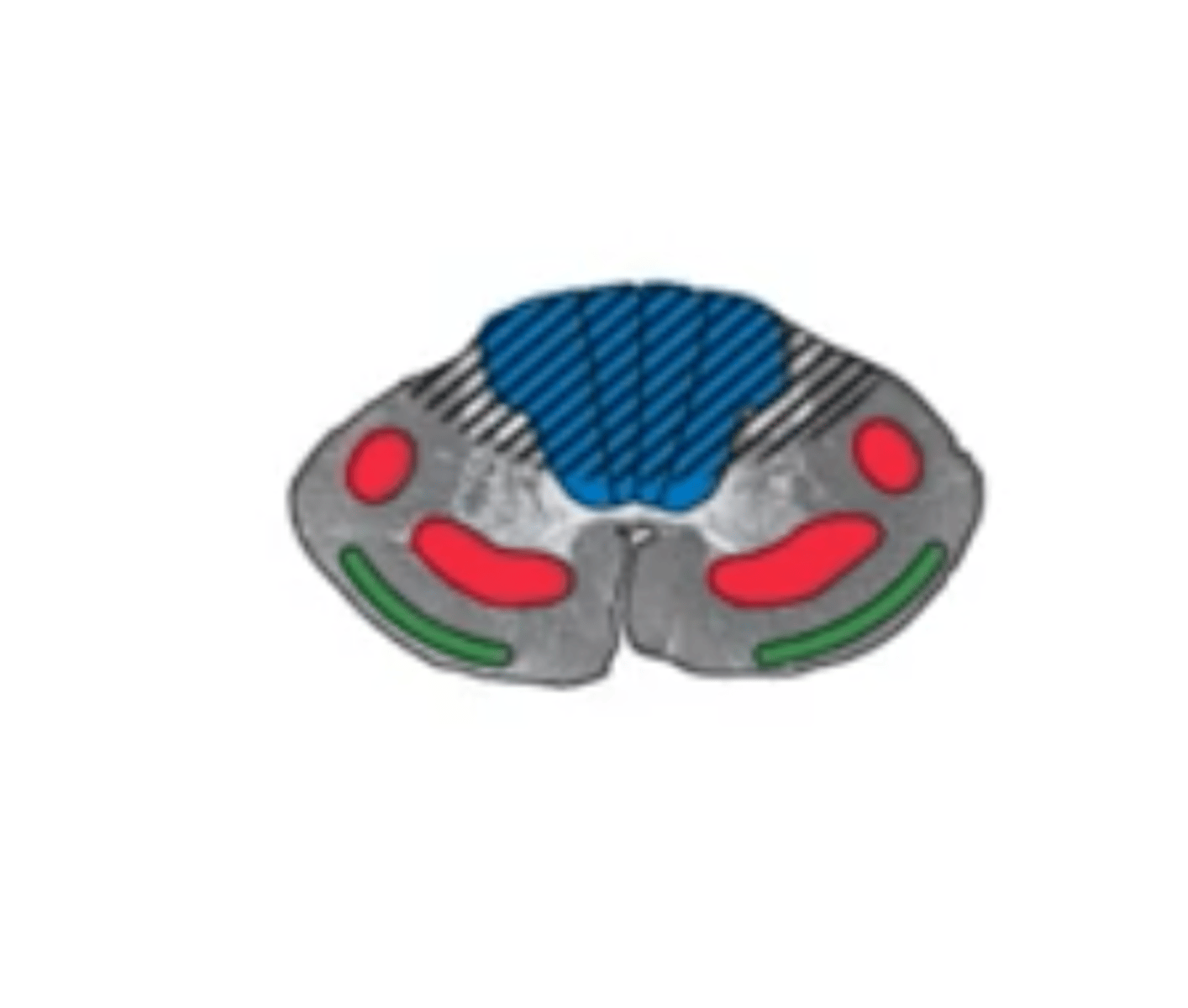
vascular territory of anterior cerebral artery
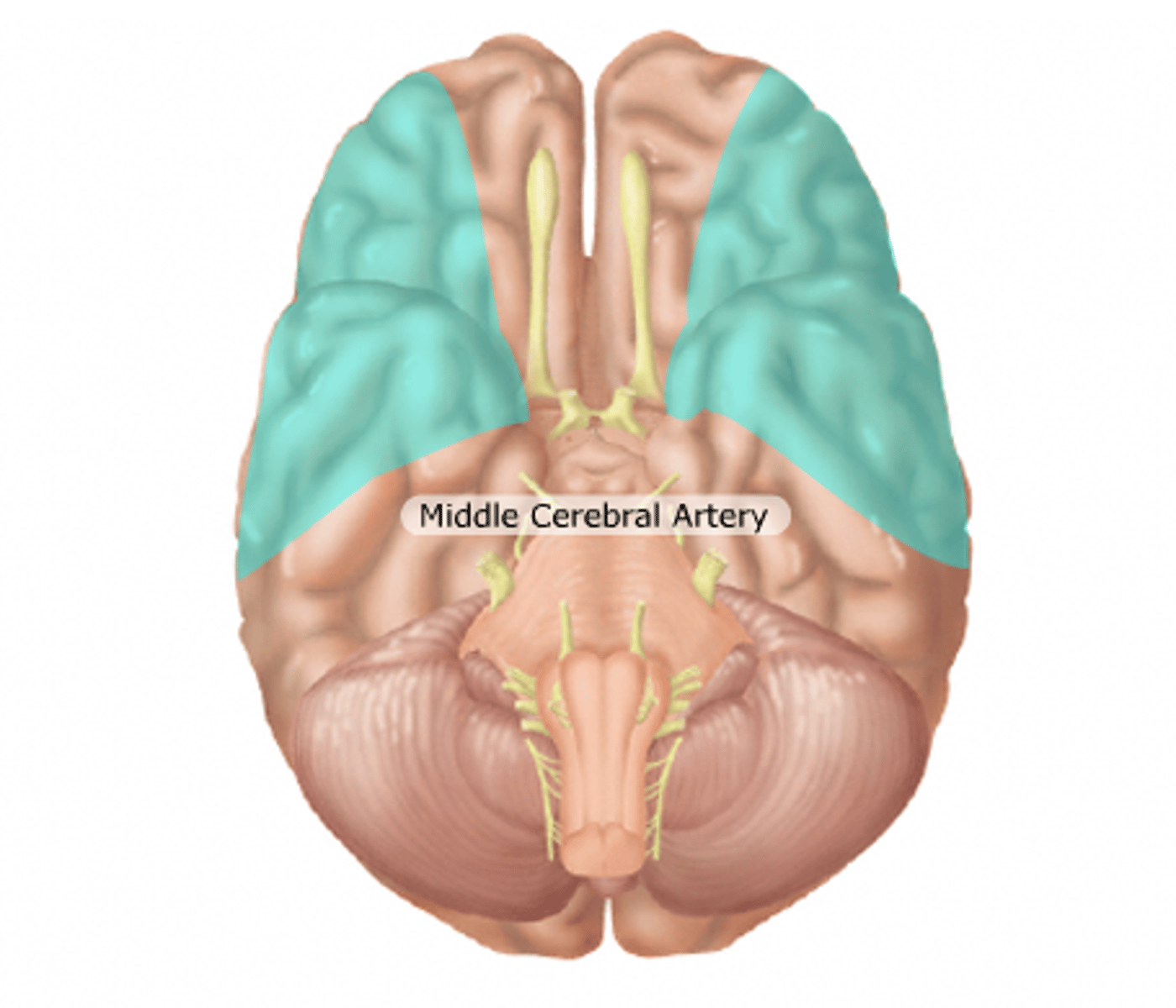
vascular territory of middle cerebral artery
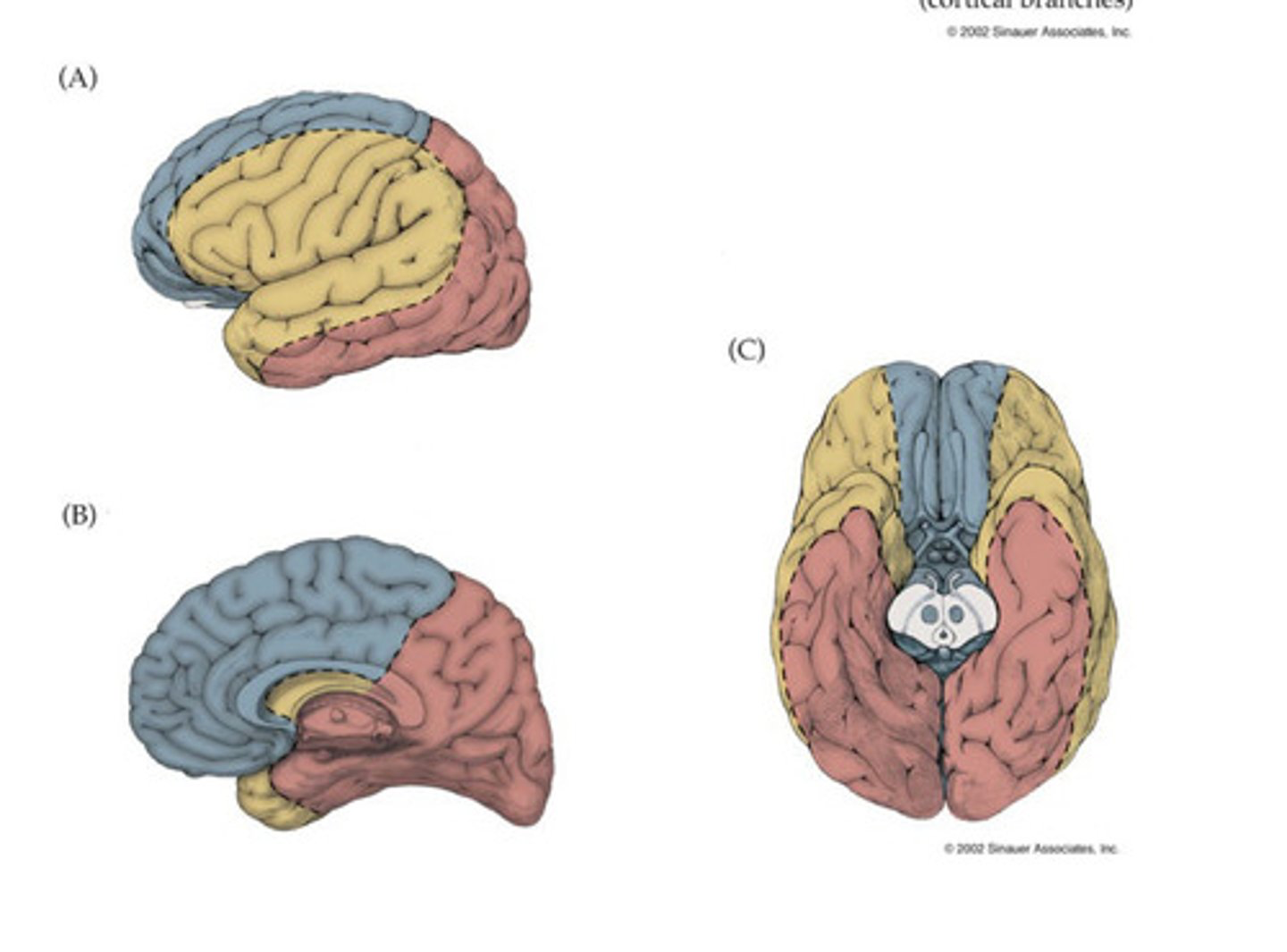
vascular territory of posterior cerebral artery
red
embolus
clot breaks loose and travels through the blood vessels, usually from a CV issue, sudden
thrombosis
clot formed locally on BV wall, usually from atherosclerosis, vessel occludes and causes more stuttering course, series of TIAs
large vessel infarct
-Involve major BV on surface of brain such as MCA and its main branches
-Often caused by emboli
small vessel infarct
Involve small, penetrating vessels that supply deep structures,
-also known as LACUNAR infarcts
-associated w/ small vessel disease caused by chronic hypertension
cortical lesion
presence of signs such as aphasia and corticosensory loss
stroke risk factors
HTN, diabetes, high cholesterol, smoking, cardiac disease, prior/ family history
MCA infarct
most common site of stroke
- can occur at stem (before branching), superior division, inferior division, or deep territory
left MCA superior division infarct
-right face and arm weakness UMN
- non fluent or broca's aphasia
- right face or arm cortical sensory loss
left MCA inferior division infarct
- wernicke's aphasia
- right visual field deficit
- right face and arm cortical type sensory loss
- confusion
- mild right side weakness
- absent motor findings
left MCA deep territory infarct
- right pure motor hemiparesis UMN
- cortical deficits, aphasia
Left MCA stem infarct
- right hemiplegia
- right hemianesthesia
- right homonymous hemianopia
- global aphasia
- left gaze preference