KNES 373 Final Exam Review Part 4
1/61
Earn XP
Description and Tags
lectures 22, 23, 24, 25, 26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
The velocity of blood flow is ____________ related to the total-cross sectional area of the blood vessels (greater CSA = slower BF).
inversely
Blood flow is slowest in the ___________. Why?
capillaries, to allow time for exchange of gases + nutrients
Cardiac muscle fibers are ___________ than skeletal muscles. Myocardium muscles are _____________, meaning they are all ___________ muscle fibers. The fibers are connected end-to-end by ________________, and the connected fibers contract at the same time.
shorter, homogenous, type I, intercalated discs
There are no satellite cells in the myocardium. Why?
satellite cells are necessary for muscle fiber type diversity, and there are only type I fibers in the myocardium
What is calcium-induced calcium release in the myocardium?
depolarization causes release of a little bit of calcium, which causes more calcium to release from the sarcoplasmic reticulum
The myocardium generates its own electrical signals due to anatomical coupling of the myocardial cells via _______________.
gap junctions
What are the specialized myocardial cells that coordinate the heart’s excitations?
sinoatrial (SA) node
atrioventricular (AV) node
AV bundles of His
Purkinje fibers
The __________ is the first part of the heart that reacts to Na+ because it is leaky to Na+.
SA node
The SA node is a group of specialized cardiac muscle fibers that do not _____________. The tissues are adapted to only generate ______________.
contract, automatic impulses
Explain the intrinsic control of heart rate + myocardium electrical activity.
SA node depolarized at a faster rate than other myocardial cells because it is leaky to Na+ compared to K+
the electrical pulses initiated by the SA nodes are spread to the AV nodes then the AV bundle
the delay between the AV node to the AV bundle is important to allow blood from the atria to completely empty to ventricles before contraction
the terminal branches of the AV bundle are the Purkinje fibers which transmit the impulses to the ventricles
What are the components of extrinsic control of the heart?
parasympathetic nervous system
sympathetic nervous system
endocrine system
The vagus nerve originates from the _______________ and sends signals to the _________ and _________ by releasing acetylcholine. Vagal tone (at rest) sets HR around ________ bpm.
medulla oblongata, SA node, AV node, 60-80
How does the sympathetic nervous system have extrinsic control over the heart?
increases the rate of depolarization of the SA node
increases HR
How does the endocrine system have extrinsic control over the heart?
epinephrine + norepinephrine from the adrenal glands
triggered by sympathetic stimulation during stress
Diastole is ____________ as long as the duration of systole. Passive flow is _____% of this phase and contraction of atria is ______% of this phase.
twice, 70, 30
~________ ms after atrial contraction, the ventricles contract. At rest systole ejects _______ of the blood out of the ventricles. The blood is forced out of the ventricles when the ventricular pressure exceeds the pressure of the ______________ and ____________.
100, 2/3, pulmonary artery, aorta
Which component of the cardiac cycle reduces the most during exercise?
diastole
_____________ establish ‘bulk flow’ and driving pressure. ____________ regulate blood flow to specific regions.
Arteries, arterioles
What is stroke volume?
volume of blood pumped during one heart beat
What is ejection fraction?
fraction (percentage) of blood pumped out of the left ventricle relative to total volume of left ventricle
What factor is the only one that doesn’t change between trained and untrained people?
ejection fraction
How does stroke volume compare between trained and untrained people?
SV is higher for trained compared to untrained
What is the Fick equation?
oxygen uptake is equal to the product of cardiac output + oxygen extraction
V = Q x a-vO2
a-vO2 difference _______________ with exercise intensity. Why?
increases
the difference between arterial O2 content and venous O2 content gets bigger because:
steady arterial O2 content (increased ventilation ensures nearly complete arterial saturation)
declining venous O2 content (more O2 being taken up by muscles)
What are the components of the peripheral input part of extrinsic regulation?
mechanical (muscle + vasculature)
chemical (group III/IV afferents)
During submaximal exercise, Q and HR increase _____________ with increases in work rate/intensity. How does SV differ?
linearly
SV demonstrates an initial increase followed by only small changes or a plateau at around 30-50% VO2max
SV = ?
EDV (end-diastolic volume) - ESV (end-systolic volume)
What 2 factors affect EDV? What 2 factors affect ESV?
EDV (amount of blood in ventricles before contraction):
venous return
ventricular distensibility
ESV (amount of blood in ventricles after contraction):
ventricular contractility
aortic (or pulmonary artery) pressure
Venous return is aided by what 3 things?
muscle pump (blood in veins is squeezed towards heart by contracting muscles)
respiratory pump (thoracic cavity like a vacuum)
valves located in veins (maintain direction of BF towards heart)
What is the Frank-Starling Law?
stretching ventricle increases force of contraction
a greater EDV yields a greater SV (within physiological limits)
How can Q increase linearly with exercise intensity if SV eventually plateaus?
Q = SV x HR
heart rate still continues to increase linearly with intensity
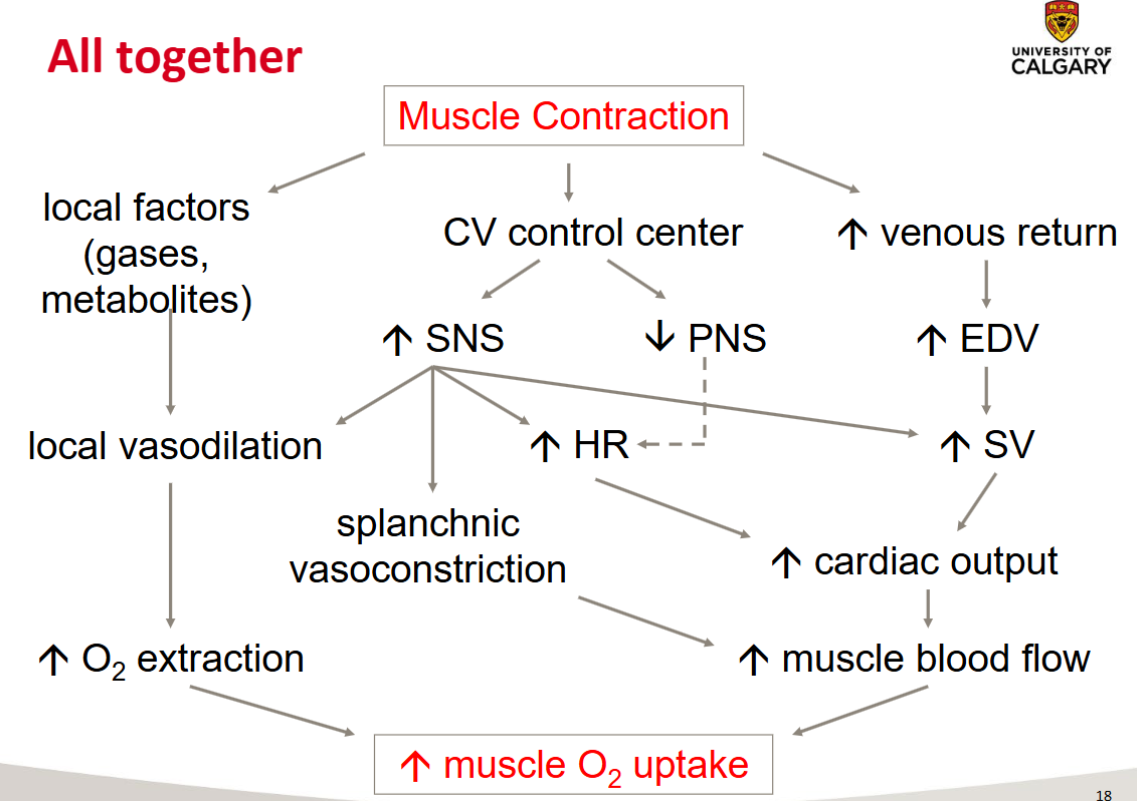
Draw the ‘all together’ slide 18 diagram.
What are the systemic adaptations from exercise?
increased blood plasma volume
increased O2 carrying capacity of the blood
increased cardiac output
What are the skeletal muscle adaptations from exercise?
increased capillarization
increased mitochondrial content
Expansion of plasma volume is observed within _____________ and ____________. Increases in red blood cell volume + total O2 carrying capacity ensue after a few ____________ of training. The resulting increase in blood volume facilitates _______________ leading to higher EDV and __________. Ventricular compliance may result from ___________ and ____________ of training.
hours, days, weeks, venous return, SV, months, years
Maximum heart rate is ________________ by exercise training.
not affected
Skeletal muscle adaptations are noticed within ____________ of training.
weeks
There is little ‘room’ for increasing a-vO2 difference, so VO2max improvements are essentially determined by increases in ________ along with the relatively preserved oxygen-carrying capacity of the blood.
stroke volume
What shows the least difference between trained and untrained people?
a-vO2 difference
VO2max is highly correlated with _________________.
maximal cardiac output
Cardiac output improves by greater _____________ and lower _________________ to a given submaximal workload.
stroke volume, heart rate
What is the role of phlebotomy on VO2max and cardiac output during cycling?
phlebotomy reduced VO2max and CO back to pre-training levels
changes in blood variables are highly relevant to training adaptations because of ‘greater capacity’ to send oxygenated blood
What are the muscle-specific morphological adaptations to training?
greater capillary/fiber ratio
better redistribution of blood flow
shorter transit time for gas exchange
greater intramuscular ‘fat’ storage
greater fat utilization during submaximal exercise
In untrained people, the __________________ is the limiting factor, in trained people the ______________ is the limiting factor.
mitochondria respiration (since O2 delivery is greater than needed), oxygen delivery (since mitochondria activity is extremely high)
What is repeated bout effect?
muscle rapidly adapts to the damage from eccentric exercise to prevent further damage, so after a second bout of eccentric exercise, the result is less muscle stiffness and soreness compared to the first bout
less swelling of muscle
smaller increase in CK
What is the sequence of muscle damage from eccentric exercise?
1) overstretched sarcomeres
2) disrupted sarcomeres
3) E-C coupling disruption
4) local contracture
5) swelling + soreness
What occurs in the overstretched sarcomere phase?
in the descending phase of the length-tension curve (eccentric contraction) weaker sarcomeres are stretched beyond myofilament overlap
What occurs during the disrupted sarcomeres phase?
overstretched half-sarcomeres fail to re-interdigitate (interlock) at rest
number of disrupted sarcomeres grows until membrane damage occurs
What is the popping-sarcomere hypothesis?
uncontrolled extension of half-sarcomeres in each myofibril
occurs one at a time, in order from weakest to strongest
each sarcomere is stretched until half-sarcomere is popped
What occurs in the E-C coupling disruption phase?
damage to elements of the E-C coupling machinery
damage process: t-tubule rupture
torn t-tubule ends would be leading to inactivation of some sarcomeres
fall in muscle tension (force output)
What occurs in the local contracture phase?
after a period of eccentric exercise, there is a rise in passive tension in the muscle (stiffness)
potential mechanisms:
increase in resting Ca2+ levels in muscle fibers damaged by eccentric contractions
shortening of parallel, non-contractile elements in the muscle (titin)
What occurs in the swelling and soreness phase?
pain sensitive receptors (afferent III/IV neurons) are responsive to mechanical deformation and the intramuscular substances which would cause pain
DOMS occurs because of accumulation of immune system cells activating nociceptors
When is DOMS at its peak?
48-72 hours post eccentric exercise
The pain experienced during muscle contraction after eccentric exercise is related to what?
damage + shortening of the non-contractile elements (stiffness)
damage to muscle fiber membranes (shown by an increase in CK enzyme)
activation of group III/IV afferents
What is the mechanism underlying RBE?
longitudinal addition of sarcomeres (sarcomeres added in series)
Eccentric contraction training results in more sarcomeres in series, which results in a shift of the length-tension curve to the ____________, towards _____________ lengths so that soreness isn’t experienced the next time.
right, longer
What are the 3 predictors for performance in endurance events?
1) VO2 max
2) % of VO2 max associated with the lactate threshold (MLSS/CP)
3) efficiency (or economy) → amount of O2 consumption required for a given submaximal exercise intensity
The adaptability of the cardiorespiratory system is the _________ compared to the periphery (mitochondria, capillarization, vasodilation in exercising muscles) which is the __________ adaptable.
least, most
VO2max is strongly correlated with endurance performance in a ________________ population (i.e. Calgary marathon with wide range of VO2 max values between people). VO2max is not the strongest predictor of performance in a _______________ population like the Olympics, because all athletes have the same or very close VO2max values. What is a better predictor for that population?
heterogenous, homogenous, economy
Lactate thresholds occur at _____________ exercise intensities in highly trained athletes, thus the accumulation of blood lactate is __________ when compared to a less fit endurance athlete.
higher, delayed
Highly trained individuals are able to sustain a greater ______________ throughout a race/event.
% of their VO2max
What is the determinant for better performance in cyclists with the same VO2max?
lactate threshold + economy